Das könnte Ihnen auch gefallen
- MMO IndianDokument5 SeitenMMO IndianSuci NourmalizaNoch keine Bewertungen
- Closed ReductionDokument3 SeitenClosed ReductionSuci NourmalizaNoch keine Bewertungen
- MMO IndianDokument5 SeitenMMO IndianSuci NourmalizaNoch keine Bewertungen
- Closed Reduksi NasalDokument5 SeitenClosed Reduksi NasalSuci NourmalizaNoch keine Bewertungen
- Kementerian Kesehatan Politeknik Kesehatan Surakarta Jurusan KeperawatanDokument6 SeitenKementerian Kesehatan Politeknik Kesehatan Surakarta Jurusan KeperawatanrudimarwanNoch keine Bewertungen
- Malunion NonunionDokument4 SeitenMalunion NonunionSuci NourmalizaNoch keine Bewertungen
- The Normal Range of Mouth Opening in Kurdish Population and Its Correlation To Age, Sex, Height, and WeightDokument6 SeitenThe Normal Range of Mouth Opening in Kurdish Population and Its Correlation To Age, Sex, Height, and WeightSuci NourmalizaNoch keine Bewertungen
- Unfavorable OutcomeDokument15 SeitenUnfavorable OutcomeSuci NourmalizaNoch keine Bewertungen
- TrismusDokument6 SeitenTrismusSuci NourmalizaNoch keine Bewertungen
- MMO IndianDokument5 SeitenMMO IndianSuci NourmalizaNoch keine Bewertungen
- Assessment of Mouth Opening Limitation in Myogenic Temporomandibular Disorder PatientsDokument5 SeitenAssessment of Mouth Opening Limitation in Myogenic Temporomandibular Disorder PatientsSuci NourmalizaNoch keine Bewertungen
- Assessment of Mouth Opening Limitation in Myogenic Temporomandibular Disorder PatientsDokument5 SeitenAssessment of Mouth Opening Limitation in Myogenic Temporomandibular Disorder PatientsSuci NourmalizaNoch keine Bewertungen
- Maxillofacial Trauma Challenges in ED Diagnosis and ManagementDokument20 SeitenMaxillofacial Trauma Challenges in ED Diagnosis and ManagementSuci NourmalizaNoch keine Bewertungen
- Management of Lefort Fractures: Vijay Ebenezer, R. Balakrishnan and Anatha PadmanabhanDokument4 SeitenManagement of Lefort Fractures: Vijay Ebenezer, R. Balakrishnan and Anatha PadmanabhanSuci NourmalizaNoch keine Bewertungen
- 10 1 1 945 5006 PDFDokument2 Seiten10 1 1 945 5006 PDFSuci NourmalizaNoch keine Bewertungen
- 10 1016@j Joms 2008 06 050Dokument6 Seiten10 1016@j Joms 2008 06 050Suci NourmalizaNoch keine Bewertungen
- An Adolescent With Limited Mouth Opening: AnswerDokument1 SeiteAn Adolescent With Limited Mouth Opening: AnswerSuci NourmalizaNoch keine Bewertungen
- Sciencedirect: Prevalence and Etiology of Midfacial Fractures: A Study of 799 CasesDokument6 SeitenSciencedirect: Prevalence and Etiology of Midfacial Fractures: A Study of 799 CasesSuci NourmalizaNoch keine Bewertungen
- 5 9y3Dokument5 Seiten5 9y3Suci NourmalizaNoch keine Bewertungen
- 11case AksDokument4 Seiten11case AksSuci NourmalizaNoch keine Bewertungen
- 2 3 Evaluation of Two Different Methods of Arch Bar Application: A Comparative Prospective StudyDokument12 Seiten2 3 Evaluation of Two Different Methods of Arch Bar Application: A Comparative Prospective StudySuci NourmalizaNoch keine Bewertungen
- 10 1016@j Joms 2008 06 050Dokument6 Seiten10 1016@j Joms 2008 06 050Suci NourmalizaNoch keine Bewertungen
- IMF Screws As An Alternative To Arch Bar Fixation in Management of Mandibular FractureDokument2 SeitenIMF Screws As An Alternative To Arch Bar Fixation in Management of Mandibular FractureSuci NourmalizaNoch keine Bewertungen
- Clinical Follow Up 2010Dokument8 SeitenClinical Follow Up 2010Suci NourmalizaNoch keine Bewertungen
- 2 3 Evaluation of Two Different Methods of Arch Bar Application: A Comparative Prospective StudyDokument12 Seiten2 3 Evaluation of Two Different Methods of Arch Bar Application: A Comparative Prospective StudySuci NourmalizaNoch keine Bewertungen
- Unilateral Mandibular Condylar Fractures-Non-Surgical TreatmentDokument5 SeitenUnilateral Mandibular Condylar Fractures-Non-Surgical Treatmentdra.hadleyNoch keine Bewertungen
- Unilateral Mandibular Condylar Fractures-Non-Surgical TreatmentDokument5 SeitenUnilateral Mandibular Condylar Fractures-Non-Surgical Treatmentdra.hadleyNoch keine Bewertungen
- Biomechanical evaluation of maxillary Lefort Ι fracture with bioabsorbable osteosynthesis internal fixationDokument9 SeitenBiomechanical evaluation of maxillary Lefort Ι fracture with bioabsorbable osteosynthesis internal fixationSuci NourmalizaNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Sydney System For The Classification of Chronic GastritisDokument8 SeitenSydney System For The Classification of Chronic GastritisJuniorNoch keine Bewertungen
- Vaginal Exam GuidelineDokument6 SeitenVaginal Exam GuidelinerohitNoch keine Bewertungen
- Mallet Finger Suturing TechniqueDokument5 SeitenMallet Finger Suturing TechniqueSivaprasath JaganathanNoch keine Bewertungen
- 4.2 MDS01 - Definition Table of The MDS Items - Ver0.94Dokument7 Seiten4.2 MDS01 - Definition Table of The MDS Items - Ver0.94AriniDwiLestariNoch keine Bewertungen
- Ebj M3 Rle24Dokument6 SeitenEbj M3 Rle24Ayen PaloNoch keine Bewertungen
- Times Leader 03-17-2013Dokument77 SeitenTimes Leader 03-17-2013The Times LeaderNoch keine Bewertungen
- Hansson Pin System Brochure P002 28 20131023Dokument24 SeitenHansson Pin System Brochure P002 28 20131023ElenaNoch keine Bewertungen
- GNU HealthDokument1 SeiteGNU Healthbhupendrapawar279Noch keine Bewertungen
- Leptospirosis, Typhoid and Other FeversDokument37 SeitenLeptospirosis, Typhoid and Other FeverskarageeNoch keine Bewertungen
- Farmakologi Anti KankerDokument75 SeitenFarmakologi Anti KankerromzikerenzNoch keine Bewertungen
- Wikipedia - Acanthosis Nigricans (CHECKED)Dokument6 SeitenWikipedia - Acanthosis Nigricans (CHECKED)pixoguiasNoch keine Bewertungen
- Alcon Cheatsheet PDFDokument1 SeiteAlcon Cheatsheet PDFSoham SahaNoch keine Bewertungen
- Nursing Care PlanDokument7 SeitenNursing Care Planrockerespi1283Noch keine Bewertungen
- NURS612 Exam 1 Review-Chen Walta - Week1-3Dokument15 SeitenNURS612 Exam 1 Review-Chen Walta - Week1-3A Marie100% (1)
- Ect BrochureDokument2 SeitenEct Brochureapi-283706202Noch keine Bewertungen
- Patient and Family Discharge Checklist: Patient Name: Reason For AdmissionDokument7 SeitenPatient and Family Discharge Checklist: Patient Name: Reason For Admissiondwirabiatul adwiyahaliNoch keine Bewertungen
- Understanding Neurology - A Problem-Orientated Approach PDFDokument241 SeitenUnderstanding Neurology - A Problem-Orientated Approach PDFAshabul AnharNoch keine Bewertungen
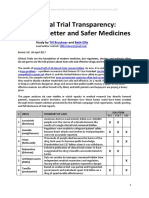
- Clinical Trial Transparency - A Key To Better and Safer Medicines (Till Bruckner and Beth Ellis 2017)Dokument21 SeitenClinical Trial Transparency - A Key To Better and Safer Medicines (Till Bruckner and Beth Ellis 2017)Till BrucknerNoch keine Bewertungen
- PPTDokument27 SeitenPPTmonicanasutionNoch keine Bewertungen
- Bryan 3-24-17Dokument12 SeitenBryan 3-24-17Bryan VandentoornNoch keine Bewertungen
- Yesterday's Tomorrow - Suvika PDFDokument223 SeitenYesterday's Tomorrow - Suvika PDFSindhu Jhaveri100% (2)
- Post Partum HemorrhageDokument40 SeitenPost Partum HemorrhageGita GirsangNoch keine Bewertungen
- IsosorbideDokument2 SeitenIsosorbideSNoch keine Bewertungen
- NCP Acute PainDokument2 SeitenNCP Acute PainNecheal BaayNoch keine Bewertungen
- Nsg241 Study Guide Exam 5Dokument76 SeitenNsg241 Study Guide Exam 5NatalieAndersonNoch keine Bewertungen
- Colon Prep in Gynecology Surgical - Dr. ExcellenaDokument18 SeitenColon Prep in Gynecology Surgical - Dr. ExcellenaEndrianus Jaya PutraNoch keine Bewertungen
- Trauma From OcclusionDokument63 SeitenTrauma From OcclusionAvita RathNoch keine Bewertungen
- Episodic SOAP Note Template - RX PedsDokument11 SeitenEpisodic SOAP Note Template - RX PedsBrianne Foster75% (4)
- Clostridium Difficile Infection and Fecal BacteriotherapyDokument9 SeitenClostridium Difficile Infection and Fecal BacteriotherapyAnonymous nEC4alrPjGNoch keine Bewertungen