Beruflich Dokumente
Kultur Dokumente
Articulo 9
Hochgeladen von
Lucero BallesterosCopyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
Articulo 9
Hochgeladen von
Lucero BallesterosCopyright:
Verfügbare Formate
The n e w e ng l a n d j o u r na l of m e dic i n e
Review Article
Dan L. Longo, M.D., Editor
Colorectal Adenomas
Williamson B. Strum, M.D.
S
ince the last review of colorectal adenomas in the Journal,1 a From the Scripps Clinic Medical Group,
wealth of new data has emerged that is improving our understanding of their La Jolla, CA. Address reprint requests to
Dr. Strum at the Scripps Clinic Medical
clinical significance. In the past 10 years, several large studies, performed Group, 10666 N. Torrey Pines Rd., La Jolla,
predominantly in the United States, have evaluated persons at average risk for CA 92017, or at fstrum@aol.com.
colorectal adenomas. The new evidence that these studies have provided regarding N Engl J Med 2016;374:1065-75.
the biology of adenomas, their prevalence and incidence, the relevance of risk DOI: 10.1056/NEJMra1513581
profiles, and controversies in screening and surveillance is germane to clinical Copyright 2016 Massachusetts Medical Society.
decisions and identifies potential targets for the improved management of these
important premalignant lesions.
A denom a s a nd Se ssil e Ser r ated P oly ps
In 2016, it is estimated that 134,000 persons in the United States will be found to
have colorectal cancer and that 49,000 will die from it.2 Approximately 15% of
persons with colon cancer are younger than 50 years of age.3 Adenomas of the
colon are estimated to be present in 20 to 53% of the U.S. population older than
50 years of age, with a prevalence of 3.4 to 7.6% for advanced histopathological
features and 0.2 to 0.6% for adenocarcinomas.3-10 Adults in the United States have
a lifetime risk of approximately 5% for adenocarcinoma.3,10 Adenomas are catego-
rized as either conventional adenomas or sessile serrated polyps and are recognized
as precursors in the majority of cases of colorectal cancer.10 In persons younger
than 60 years of age, slightly more than half of adenomas are located in the distal
colon; in persons 60 years of age or older, a slightly higher percentage of adeno-
mas are found in the proximal colon.4 Adenomas may be flat, sessile, subpedun-
culated (having a very short stalk, or peduncle), or pedunculated.10,11
Sequencing studies have traced the evolution of most conventional adenomas
and sessile serrated polyps into carcinomas through one of two major pathways:
the chromosomal instability pathway or the microsatellite instability pathway. In
both pathways, approximately 25 genes that are commonly affected by somatic
mutations become the major drivers of most cancers. These genes include APC and
TP53, the most commonly mutated tumor-suppressor genes, and KRAS, PI3KCA,
BRAF, and NRAS, the most commonly mutated oncogenes. Approximately 85% of
colorectal cancers are thought to evolve from conventional adenomas through a
median of approximately 60 mutations per tumor that go beyond the genes that
are major drivers; this process is referred to as the adenoma-to-carcinoma sequence.
A minority of colorectal cancers (approximately 15%) develop through an alterna-
tive hypermutation pathway, with a median of 700 subtle mutations that are im-
plicated in altering protein products and that result in high-frequency microsatel-
lite instability. Molecular alterations include hypermethylation of CpG islands that
leads to the CpG island methylator phenotype (CIMP), which, in association with
BRAF mutations and dysfunction owing to hypermethylation of the MLH1 DNA
n engl j med 374;11 nejm.org March 17, 2016 1065
The New England Journal of Medicine
Downloaded from nejm.org at CALIF INSTITUTE OF TECHNOLOGY on March 16, 2016. For personal use only. No other uses without permission.
Copyright 2016 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
mismatch-repair gene, results in microsatellite studies involving patients with colonic adeno-
instability, rendering the epithelial cells prema- mas have consistently confirmed the relationship
lignant. This sequence of events is termed the of size to the likelihood of cancer.4,8 Size is used
serrated neoplasia pathway.10,12-15 That an exten- to classify adenomas into three classes: diminu-
sive succession of multiple somatic mutations tive (1 to 5 mm in diameter), small (6 to 9 mm),
confers a growth advantage on a mutant cell is a and large (10 mm). By definition, adenomas are
putative model of cancer that implicates chance considered advanced on the basis of size alone if
as well as causality.16 they are 10 mm or more in diameter, and adeno-
Sessile serrated polyps are heterogeneous mas that are smaller than 1 cm in diameter are
lesions that differ from conventional adeno- considered to be advanced if they contain at least
mas.10,17-20 They are characterized by exaggerated, 25% villous features, high-grade dysplasia, or
saw-toothed, luminal serrations with dilatation, carcinoma. Adenomas with 25 to 75% villous
branching, and distortion in the bases of the features are considered to be tubulovillous, and
colonic crypts and are usually found in the proxi- those with villous architecture of more than
mal colon. The most serious subtypes are sessile 75% are classified as villous adenomas (Fig. 2).10
serrated polyps and traditional serrated adeno- In a study involving 13,992 participants who
mas, although the most common type is a benign underwent screening colonoscopy, 5891 nontumor-
hyperplastic polyp.10,20 The microscopic features ous polyps were removed; of these, 3469 (59.0%)
are subject to interpretation, and the degree of were adenomatous and 920 (15.6%) were ad-
variability of classification among pathologists vanced. Diminutive polyps made up 64% of all
is high.21 The lesions are recognized endoscopi- polyps, of which 1.1% were advanced adenomas,
cally as flat and oblong; often they are covered and included one cancer. Small polyps made up
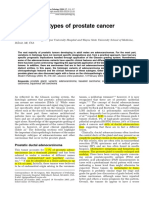
with mucus and are thus difficult to see (Fig. 1).
The factors that increase the risk of malig- A
nant features in sessile serrated polyps are
similar to those in conventional adenomas.
These factors include a large size of the polyp
and, in the patient, older age, a history of smok-
ing, a family history of cancer, and nonuse of
nonsteroidal antiinflammatory drugs (NSAIDs).
There is a slightly higher rate of sessile serrat-
ed polyps, as well as some evidence of more
aggressive biologic features, among women than
among men.13,17,20
Studies of end-stage colon cancer have shown
B
that malignant conditions that are identified
within the first 5 years after colonoscopy are
twice as likely to be characterized by CIMP and
microsatellite instability as those identified after
5 years.17,19 In prevalence studies, sessile serrated
polyps are reported in 1 to 18% of patients (aver-
age, approximately 6 to 12%).15,17,18,22 Their true
prevalence has not been established, and more
study is needed to determine their prevalence,
relevance, and natural history.
Figure 1. Sessile Serrated Polyp.
Panel A shows the typical endoscopic features of a polyp
cl inic a l signific a nce with a flat, sessile, and oblong appearance (arrow).
of a denom a Si ze Panel B shows the characteristic microscopic features
(hematoxylin and eosin staining) of exaggerated serra-
Size has long been recognized as one of the tions, aberrant crypts, with branching and dilatation,
most important markers of the potential of the which often lead to a boot-shaped irregularity (inset).
adenoma to contain cancer.10,14,23 Large clinical
1066 n engl j med 374;11 nejm.org March 17, 2016
The New England Journal of Medicine
Downloaded from nejm.org at CALIF INSTITUTE OF TECHNOLOGY on March 16, 2016. For personal use only. No other uses without permission.
Copyright 2016 Massachusetts Medical Society. All rights reserved.
Colorectal Adenomas
A Diminutive Polyp B Small Polyp C Large Polyp
Figure 2. Three Classes of Adenoma According to Size.
Top panels show endoscopic photographic images, and bottom panels microscopic features of benign adenomas
(hematoxylin and eosin staining) that differ in size. Each pair of photographic and microscopic images shows the
same polyp. Panel A shows a 4-mm adenoma. Adenomas that are 5 mm in diameter or smaller make up 45 to 71%
of all detected adenomas; 7 to 16% of the adenomas in this size range have advanced histopathological features,
and as many as 0.05% are malignant. Panel B shows an 8-mm adenoma. Adenomas that are 6 to 9 mm in diameter
make up 21 to 23% of all detected adenomas; 10 to 34% of these small adenomas have advanced histopathological
features, and as many as 0.2% are malignant. Panel C shows a 20-mm adenoma. Adenomas that are 10 mm or larger
in diameter make up 8 to 22% of all detected adenomas. All adenomas in this class are considered to be advanced
on the basis of their size; 37 to 54% have advanced histopathological features, and 3.2 to 11% are malignant.
20% of all polyps, of which 1.3% were advanced with immediate removal or follow-up CT colo-
adenomas, and included two cancers. Large nography in 3 years is a reasonable option.25-27 In
polyps accounted for the remaining 16% of all a study of combined CT colonography and colo-
polyps, of which 13.2% were adenomas; all noscopy involving 6283 patients, advanced adeno-
these polyps were considered to be advanced be- mas of 6 to 9 mm in diameter, with no cancers,
cause of their size, and one third had additional were reported in 0.2% of patients.26 Follow-up
advanced histopathological features, including testing with use of CT colonography offers a
25 cancers.8 Thus, polyps that were less than 1 cm unique opportunity for the study of the volumet-
in diameter represented 84% of all colon polyps ric growth rates and natural history of these
removed and 15% of all advanced adenomas; small and predominantly benign adenomas.28
they accounted for 3 of the 74 cancers found in The evidence that more than 99% of diminu-
the 13,992 people in the final study group tive and small lesions are benign has led inves-
(0.02% of participants). As polyp size increased tigators to consider alternatives to submitting all
to 10 mm or more, the risk of advanced histo- polyps for histopathological analysis. These strat-
pathological features and cancer increased pro- egies include resecting and discarding diminu-
portionally. In this study and three others,7,24,25 tive polyps or making an endoscopic diagnosis
27 to 47% of all the subcentimeter polyps that of unlikely to become cancerous and leaving
were removed were nonadenomatous. them in place29,30; using data on polyps larger
Radiologists conducting examinations with than 9 mm as a surrogate marker for advanced
diagnostic computed tomographic (CT) colonog- adenomas to the exclusion of subcentimeter
raphy do not customarily report lesions that are polyps, which have advanced histopathological
less than 6 mm in diameter and consider lesions features in less than 3%4831; and recommending
that are between 6 and 9 mm in diameter to be wider use of noninvasive screening approaches,
sufficiently benign such that either colonoscopy particularly for persons in whom the risk of
n engl j med 374;11 nejm.org March 17, 2016 1067
The New England Journal of Medicine
Downloaded from nejm.org at CALIF INSTITUTE OF TECHNOLOGY on March 16, 2016. For personal use only. No other uses without permission.
Copyright 2016 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
Table 1. Recommendations for Surveillance and Screening Intervals in Persons with Average Risk at Baseline, 2012.*
Recommended Quality of Evidence Presence of New
Most Advanced Findings at Baseline Surveillance Supporting the Evidence Stronger
Colonoscopy Interval Recommendation Than in 2006
yr
No polyps 10 Moderate Yes
Hyperplastic polyps <10 mm in rectum 10 Moderate No
or sigmoid colon
12 tubular adenomas <10 mm 510 Moderate Yes
310 tubular adenomas 3 Moderate Yes
>10 adenomas <3 Moderate No
1 tubular adenomas 10 mm 3 High Yes
1 villous adenomas 3 Moderate Yes
Adenoma with high-grade dysplasia 3 Moderate No
Serrated lesions
1 sessile serrated polyps <10 mm 5 Low NA
with no dysplasia
1 sessile serrated polyps 10 mm or 3 Low NA
1 sessile serrated polyp with dysplasia
or traditional serrated adenoma
Serrated polyposis syndrome 1 Moderate NA
* Recommendations are from Lieberman et al.34 The recommendations assume that the baseline colonoscopy was com-
plete and adequate and that all visible polyps were completely removed. Sizes of polyps are diameters. NA denotes not
applicable.
The rating of evidence relies on expert consensus regarding whether new research is likely to change the confidence
level of the recommendation.
The serrated polyposis syndrome is defined, according to the World Health Organization,20 as meeting one of the follow-
ing criteria: at least 5 serrated polyps that are proximal to the sigmoid colon, with 2 or more that are 10 mm or more in
diameter; any serrated polyps that are proximal to the sigmoid colon plus a family history of the serrated polyposis syn-
drome; or more than 20 serrated polyps of any size throughout the colon.
advanced pathologic features is considered low.32,33 cancers.7,8,25 When adenocarcinoma is found in
The approach of documenting diminutive polyps an adenoma, the pathological examination em-
with a high-resolution photograph, followed by phasizes the distance between the cancer and
a resect-and-discard or diagnose-and-leave strat- the margins of the polyp, the size of the lesion,
egy, deserves further study.29,30 the degree of differentiation of the tumor, and the
degree of lymphatic and vascular invasion.10,14,23
Guidelines for surveillance after the removal of
Pathol o gic a l Fe at ur e s a nd
Their Effec t on Surv eil l a nce adenomas recommend a follow-up colonoscopy
at 3 years if any index adenoma (adenoma ob-
Histopathological examination of colon polyps served during the initial examination) is ad-
defines their neoplastic nature and potential and vanced, defined as 10 mm or more in diameter,
is the best measure of their degree of severity; if 25% or more of an adenoma of any size has
diminutive and small adenomas are considered to villous features or high-grade dysplasia, or if 3 to
be advanced if they contain at least 25% villous 10 adenomas of any size are present (Table 1).34
features, high-grade dysplasia, or carcinoma.10,14,23 Surveillance studies from a pooled analysis of
Since as many as 1 in 10 of diminutive-to-small data from 9167 patients and from follow-up
lesions contain advanced histopathological fea- studies of the incidence of advanced adenomas
tures, they make up the largest group of ad- provide data that may be summarized as follows.
vanced adenomas (70 to 83%), even though they First, after an advanced adenoma is found at
are the smallest in size and contain the fewest baseline, the overall incidence of advanced ade-
1068 n engl j med 374;11 nejm.org March 17, 2016
The New England Journal of Medicine
Downloaded from nejm.org at CALIF INSTITUTE OF TECHNOLOGY on March 16, 2016. For personal use only. No other uses without permission.
Copyright 2016 Massachusetts Medical Society. All rights reserved.
Colorectal Adenomas
nomas within 4 years averages 11%. Second, the cancer is diagnosed began to decline 30 years
rate of advanced adenomas is highest at 24% for ago, the rate of decline has accelerated in the
index adenomas (those 20 mm in diameter), is past few years; a decrease of 2.8% per year from
next highest at 19% if there are five or more 2003 to 2012 was noted in both men and women
index adenomas of any size at baseline, and be- in almost all major racial and ethnic groups.2,3
comes progressively lower with less advanced Meanwhile, the percentage of patients with newly
neoplasia at baseline. Third, the rates of discov- diagnosed colorectal cancer who are younger
ery of cancer at the time of a follow-up surveil- than 50 years of age has increased to 15%.3,45,46
lance colonoscopy range from 0.3 to 0.9%, with A study involving 3558 persons from 20 to 89
an average of 0.6% slightly higher than the years of age who underwent consecutive autop-
rate at the initial screening. Fourth, after a sies between 1985 and 2004 showed that the
negative surveillance examination, subsequent prevalence of adenomas in this deceased popula-
examinations yield progressively fewer advanced tion was 1.72% in the third decade of life and
adenomas.35-38 increased to 3.59% in the fifth decade. The rate
These results can be compared with those of then increased sharply after 50 years of age,
a study involving 17,525 patients who underwent which conforms to the customary assumption
colonoscopy and were then reexamined 1 to that the rise in the prevalence of adenomas and
5 years and 5 to 10 years later.31 Among the carcinomas increases dramatically after 50 years
15,719 patients who had negative findings on of age.47
an initial uncompromised colonoscopy (defined In screening studies that have evaluated per-
as a complete examination with an adequate sons who were 40 to 49 years of age, 2.0 to 5.6%
bowel preparation and no lesions found) and are found to have an advanced adenoma or large
who were reexamined after 1 to 5 years and 5 to polyp. The largest such study reported an inci-
10 years, the reported incidence of large polyps dence of large polyps of at least 5% among men
(which are surrogate markers for advanced ade- who were white, black, or Hispanic and among
nomas) was 3.1% among the patients examined black women.4,48 There is no consensus that per-
within 1 to 5 years and 3.7% among those ex- sons in this age range who are at average risk
amined within 5 to 10 years. Overall, 501 large should be screened. However, clinicians are
polyps (>9 mm in diameter) were identified (in- advised to recognize the rising prevalence of
cidence, 3.2%), as well as one established cancer colorectal cancer in this age group and to be pre-
(incidence, 0.006%). Among the 1806 patients pared to pursue any suspicious symptoms, as well
(10.3%) who had a compromised initial colonos- as to be aware of the possibility of a hereditary
copy, primarily because of inadequate bowel disorder.15,49
preparation or an incomplete examination, and
underwent a repeat colonoscopy within 1 year, Sex, Race, and Ethnic Background
117 patients (6.5%) had polyps that were larger On the basis of data representing 327,785 adults
than 9 mm in diameter and 2 (0.11%) had an who were 40 years of age or older and who had
established cancer.31 The authors concluded that an average risk of colorectal cancer, the risk fac-
repeated colonoscopy within 10 years after an tors for advanced adenomas can be defined more
uncompromised baseline examination is of little clearly.4 Age remains critical, since the risk of
benefit to patients. Other follow-up studies that large polyps and advanced adenomas increases
have been conducted after negative initial colo- progressively with age among both men and
noscopic examinations have yielded similar fa- women, beginning to accelerate at 50 years of
vorable results.6,19,39-41 age. Blacks have a higher risk of advanced ade-
nomas than whites from 50 to 65 years of age,
and Hispanics have a lower risk than non-His-
Fac t or s A ffec t ing R isk
panics from 50 to 80 years of age. The preva-
Age lence of large polyps among white men who are
Older age remains closely correlated with the 50 to 54 years old was 6.2%, and it was similar
incidence of both adenomas and colorectal can- among black men of the same age, black women
cer.6,10,19,27,42-44 Although the number of patients and Hispanic men who were 55 to 59 years of
older than 50 years of age in whom colorectal age, white women who were 65 to 69 years of
n engl j med 374;11 nejm.org March 17, 2016 1069
The New England Journal of Medicine
Downloaded from nejm.org at CALIF INSTITUTE OF TECHNOLOGY on March 16, 2016. For personal use only. No other uses without permission.
Copyright 2016 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
age, and Hispanic women who were 70 to 74 years nizes this apparent advantage as well.3 Reviews
of age. Related studies have shown similar re- have noted that the effect of estrogen and pro-
sults.19,27,43 Age, sex, race, and ethnic background gestin, calcium, vitamin D, folate, and statins in
clearly define the sharpest boundaries among preventing adenomas is limited to nonexistent.55-57
persons in different classifications and provide
demarcations for the assignment of risk.
Guidel ine s a nd Scr eening
Body-Mass Index, Lifestyle, Diet, Screening for adenomas and early-stage colorec-
and Medications tal cancer is endorsed by the U.S. Preventive Ser-
The search for additional markers of risk has vices Task Force, the American Cancer Society,
involved evaluation of risk factors including the the American College of Physicians, and other
medical history of first-degree relatives with authoritative organizations.2,3,58,59 The decline in
colorectal cancer, personal history of smoking mortality from colorectal cancer since 1975 has
and alcohol consumption, presence of obesity been attributed primarily to three factors: screen-
(body-mass index [the weight in kilograms divid- ing (responsible for 53% of the decline); im-
ed by the square of the height in meters], 30), proved lifestyle, including better diet and exer-
quantity of red meat in the diet, and previous cise, use of hormone-replacement therapy and
detection of polyps, as well as protective factors NSAIDs, and less smoking and alcohol con-
including the consumption of fruits and vegeta- sumption (responsible for 35%); and better treat-
bles, regular physical exercise, use of hormone- ment (responsible for 12%).2,3 Guidelines in the
replacement therapy, current or past regular United States recommend that screening for
use of NSAIDs (at least two times per week for colon adenomas and carcinomas be initiated at
1 year), and favorable prior screening examina- the age of 50 years for men and women who are
tions.50 A study involving 4143 patients who were at average risk, with follow-up at specified inter-
scheduled for an initial colonoscopy validated a vals according to whether the initial screening
risk-assessment score that was based on age, identifies an absence of neoplasia, advanced neo-
sex, family history, smoking history, and waist plasia, or cancer (Table 2). Screening methods
circumference and that was used to assign some include the fecal occult-blood test, stool DNA
patients to undergo less invasive tests, such as test, sigmoidoscopy, barium enema with the use
flexible sigmoidoscopy and fecal occult-blood of air contrast, CT colonography, and optical
testing.51 colonoscopy. In the U.S. population, 59% of
Among attempts to identify medications that persons 50 years of age or older are current with
can prevent or forestall colon cancer, the most recommended screening, which indicates a mod-
promising has been the regular use of aspirin, est rise since 2000 that is due exclusively to
which inhibits cyclooxygenase-2 and induces colonoscopy testing.
apoptosis in adenomatous tissue. However, this There are two types of high-sensitivity fecal
effect has required long-term use of aspirin, for occult-blood tests: guaiac-based and immuno-
10 years or longer, and the side effect of gastro- chemical (also called the fecal immunochemical
intestinal bleeding has had a dampening effect test [FIT]). The guaiac-based test measures blood
on its implementation.52 In 2015, the U.S. Pre- from any source, including dietary meat. FIT uses
ventive Services Task Force published a draft an antibody specific to human hemoglobin and
recommendation statement that aspirin therapy can be calibrated quantitatively but is more ex-
is a viable approach to the prevention of colorec- pensive than the guaiac-based fecal occult-blood
tal cancer, as well as cardiovascular disease. test and has not been standardized (e.g., the test
These guidelines apply to persons who have no measures nanograms of hemoglobin per milli-
increased risk of bleeding, have a life expectancy liter of buffer, and the result is converted to
of at least 10 years, and are willing to take a micrograms of hemoglobin per gram of stool;
low-dose aspirin (81 mg) once a day. The great- different brands of the test may use different
est benefit is expected in persons 50 to 59 years quantities of stool or buffer for testing; thus, a
of age (a grade B recommendation) and in per- positive report may reflect a wide difference in
sons 60 to 69 years of age (a grade C recommen- the concentration of hemoglobin per gram of
dation).53,54 The American Cancer Society recog- stool).60 Randomized trials with the use of the
1070 n engl j med 374;11 nejm.org March 17, 2016
The New England Journal of Medicine
Downloaded from nejm.org at CALIF INSTITUTE OF TECHNOLOGY on March 16, 2016. For personal use only. No other uses without permission.
Copyright 2016 Massachusetts Medical Society. All rights reserved.
Colorectal Adenomas
Table 2. Guidelines for Screening for the Early Detection of Colorectal Adenomas and Carcinoma in Women and Men at Average Risk.*
Interval of
Testing Category and Test Advantages Limitations Examinations
Structural examination
Optical colonoscopy Examines entire colon; permits biopsy and Sedation needed; risk of serious 10 yr
removal of polyps; requires cessation of adverse events in 0.3 to 0.6%
anticoagulation; has 90% sensitivity for of patients examined; can be
detecting lesions 10 mm in diameter expensive
CT colonography Examines entire colon; quick; has few com- Low-dose radiation; may detect in- 5 yr
plications; can detect extracolonic abnor- significant extracolonic lesions
malities; has 90% sensitivity for polyps
10 mm in diameter; equivalent to optical
colonoscopy
Flexible sigmoidoscopy Simple and quick; less bowel preparation Visualization limited to lower third 5 yr
needed than for colonoscopy and CT of colon; recommended for use
colonography; has few complications; with annual fecal occult-blood
reduces incidence of colon cancer in the testing
distal colorectum and mortality from
colorectal cancer
Barium enema with the use of Examines entire colon; quick; has few com- Full bowel preparation needed; 5 yr
air contrast plications less sensitive than optical colo-
noscopy and CT colonography;
low dose of radiation
Stool-based examination
Guaiac-based fecal occult- Simple; can be applied widely; slightly more Limited sensitivity; necessitates re- 1 yr
blood test effective when combined with flexible petitive testing
sigmoidoscopy every 5 yr
FIT Specific for human hemoglobin; sensitivity Has not been standardized; thresh- 1 yr
of 74% for colorectal cancer and 24% for old for positive report may vary
advanced adenomas; more effective when with different test kits; requires
combined with flexible sigmoidoscopy more technical analysis than
guaiac-based fecal occult-blood
test and is more expensive
Stool DNA test Improved multitarget DNA test; sensitivity High cost relative to other stool- Uncertain
of 92% for colorectal cancer and 42% for based tests
advanced adenomas
* Screening of men and women at average risk is recommended to begin at 50 years of age. Tests that have the best chance to detect both pre-
cancerous adenomas and early cancer are preferred, and examination should visualize parts or all of the colon. The recommended time interval
should be reexamined after uncompromised baseline examination. Some persons are at increased risk for colorectal cancer owing to a family
history of one or more first-degree relatives with colorectal cancer, a genetic syndrome, or a chronic disease, including inflammatory bowel dis-
ease. Persons at increased risk should begin screening at an earlier age than others and should have shorter intervals between examinations.
The initiation of screening and choice of test may be influenced by a persons risk profile. FIT denotes fecal immunochemical test.
Structural examinations are capable of detecting both cancer and precancerous adenomas, can prevent as well as detect colorectal cancer,
require a full bowel preparation, often require sedation, are invasive, and may cause serious complications.
Colonoscopy has been shown to reduce the incidence of and mortality from colorectal cancer.
Stool-based examinations are more sensitive for detecting cancers than precancerous adenomas, do not require bowel preparation, can be
done at home, are low in cost and noninvasive, do not detect most adenomas, trigger colonoscopy if positive, and may produce false-posi-
tive results.
The Food and Drug Administration has approved the use of stool DNA testing at 3-year intervals.
guaiac-based fecal occult-blood test have shown and BMP3 has been shown to have a 92% sensi-
its efficacy in detecting cancer and reducing tivity for detecting colorectal cancer, but it is
mortality from colon cancer by 15 to 33% in the inferior (sensitivity, 42%) for detecting advanced
short term, but its use has not affected all-cause adenomas. These results were compared with
mortality in the long term.61,62 concurrent detection with use of the FIT, which
Multitarget stool DNA testing for mutant had a sensitivity of 74% for colorectal cancer and
KRAS and for aberrant methylation in NDRG4 24% for advanced adenomas. However, the spec-
n engl j med 374;11 nejm.org March 17, 2016 1071
The New England Journal of Medicine
Downloaded from nejm.org at CALIF INSTITUTE OF TECHNOLOGY on March 16, 2016. For personal use only. No other uses without permission.
Copyright 2016 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
Table 3. Rates of Detection of Advanced Adenomas and Colorectal Cancer by FIT and Stool DNA Testing, as Compared
with Optical Colonoscopy.*
Advanced
Adenomas Cancers
Trial and Test Participants Detected P Value Detected P Value
no. no. (%) no. (%)
Quintero et al. 61
Optical colonoscopy 5,059 493 (9.7) 27 (0.5)
FIT 10,507 252 (2.4) <0.001 36 (0.3) 0.09
Imperiale et al. 5
Optical colonoscopy 9,989 757 (7.6) 65 (0.7)
FIT 9,989 180 (1.8) <0.001 60 (0.6) 0.13
Stool DNA 9,989 321 (3.2) <0.001 48 (0.5) 0.13
* The studies were selected on the basis of their large numbers of participants, their randomized, controlled designs, and
the comparison of the results of FIT or stool DNA testing with those of optical colonoscopy. FIT was positive in the study
by Quintero et al.61 at the level of 75 ng or more of hemoglobin per milliliter of buffer and in the study by Imperiale et al.5
at the level of more than 100 ng of hemoglobin per milliliter of buffer. All P values were determined by means of Pearsons
chi-square analyses.
ificity of the FIT for nonadvanced or negative a further examination after 3 years.25-27,65-67 A deci-
findings (96.4%) was superior to that of the sion analysis suggests that this approach may
stool DNA test (89.8%). The authors indicated result in more cancers and deaths than would
that the role of stool DNA testing in screening occur with immediate removal.68 Barium enema
for colorectal cancer requires that additional fac- with the use of air contrast has been replaced for
tors be assessed, including performance charac- the most part with the more sensitive optical
teristics of alternative tests, testing intervals, colonoscopy and CT colonography, but it remains
complications, costs, acceptance by the patient of an option when these tests are unavailable.
this type of stool test (e.g., DNA analysis), and Optical colonoscopy makes possible the diag-
adherence by the patient to the stool-collection nosis of cancer and the removal of precancerous
and submission process.5 The FIT and stool DNA adenomas. Although randomized trials have not
tests are moderately sensitive for cancer but much been conducted, observational and casecontrol
less sensitive than colonoscopy for precancerous studies strongly suggest that optical screening by
adenomas (Table 3). Randomized trials of assess- means of colonoscopy can reduce the incidence
ment by means of flexible sigmoidoscopy have of and mortality from distal and proximal colorec-
shown reductions in the incidence of and mor- tal cancers. These results are more robust for
tality from colorectal cancer of the distal colon distal than proximal colorectal cancer,19,69 and
by 21% and 26%, respectively, but no evidence of this effect on incidence and mortality can last
such reductions in the proximal colon.63,64 up to 15 years.6,19,31,41,70
Screening with CT colonography evaluates the Optical colonoscopy is associated with a 2 to
entire colon and is free from complications from 9% risk of an interval cancer (one that is detected
bleeding or perforation.65-67 The disadvantages of between scheduled colonoscopies)6,19,44,71,72,73 and
this method include the inability to remove an a risk of major complications. The rate of bleed-
identified polyp, which may require a second ing is 0.1 to 0.6% and the rate of perforation is
bowel preparation and procedure, and the detec- 0.1 to 0.3%; these risks increase with age.74 The
tion of incidental extracolonic lesions, which may majority of cancers that are not detected during
lead to unnecessary risks and costs. The proce- colonoscopy are in the proximal colon.6,19,73 The
dure is equivalent to optical colonoscopy for the appearance of interval cancers is often due to
detection of polyps larger than 5 mm in diameter. the progression of adenomas or adenocarcino-
In view of the low rate of advanced histopathologi- mas that were present at the most recent exami-
cal findings among polyps smaller than 10 mm nation but were not detected or were incom-
in diameter, patients are often followed up with pletely removed, inadequate time devoted to the
1072 n engl j med 374;11 nejm.org March 17, 2016
The New England Journal of Medicine
Downloaded from nejm.org at CALIF INSTITUTE OF TECHNOLOGY on March 16, 2016. For personal use only. No other uses without permission.
Copyright 2016 Massachusetts Medical Society. All rights reserved.
Colorectal Adenomas
examination, or the presence of biologically ag- of these adenomas are advanced and 0.2 to 0.6%
gressive tumors with a rapid growth rate.6,19,71 are cancerous. The size of the adenoma corre-
Multiple studies show a correlation among inter- lates most closely with the likelihood of ad-
val cancers, examinations lasting less than 6 to vanced pathologic findings and is significantly
8 minutes, and rates of detection of adenomas related to older age, male sex, and the predict-
below 20%.6,19,72,73,75 Although these shortcom- ability of metachronous advanced adenomas.
ings are being evaluated71,75,76 and should be cor- Multiple screening tests are available, but none
rectable, it remains to be proven that the rate of is perfect. Colonoscopy is widely used for the
interval cancers will fall. detection and removal of adenomas and is effec-
An age of 76 years or older and the presence tive in reducing the incidence of and mortality
of serious coexisting conditions with a life ex- from proximal and distal colon cancer. Studies
pectancy of less than 10 years are considered to of the importance of sex, race, ethnic back-
be contraindications to screening and surveil- ground, and age suggest that improved stratifi-
lance.71,77,78 Persons between 76 and 85 years of cation and the definition of low-risk profiles
age who have never undergone screening are could lead to wider use of less invasive screening
exceptions if they are in satisfactory health. Al- techniques. Subcentimeter adenomas are the least
though the risk of colorectal cancer continues serious type and could be a target in efforts to
with advancing age, the risks of complications reduce the volume and costs of histopathological
of colonoscopy also increase with age. Screening examinations.
is not appropriate after 85 years of age or at any Studies of the incidence of adenomas within
stage at which risk exceeds benefit. 5 years after the removal of an advanced adenoma
However, studies indicate that these guide- show that such adenomas are identified, on aver-
lines are not closely observed. An analysis of age, in 11% of patients and cancer is identified
Medicare claims data for 57,597 beneficiaries in 0.6%; these rates can be compared with rates
who were 66 years of age or older and who un- of 3.1% and 0.014%, respectively, among persons
derwent at least one colonoscopy showed that 1 to 5 years after an uncompromised index colo-
nearly 25% had an estimated life expectancy of noscopy with negative findings. These yields
less than 10 years.79 Similarly, evaluation of the confirm that large adenomas and multiple ade-
care received by 3627 patients enrolled in the nomas are the most serious risk factors for the
Prostate, Lung, Colorectal, and Ovarian Cancer subsequent development of metachronous ad-
screening trial and by 1455 patients in the Veter- vanced adenomas. After an initial uncompro-
ans Affairs health care system who underwent mised colonoscopy with negative findings, the
colonoscopic reexamination indicated nonadher- rates of detection of advanced adenomas are
ence to guidelines among patients at low risk and uniformly low, with correspondingly low rates of
underuse of colonoscopies among patients at cancer.
high risk.80,81 These findings indicate that im- Enhanced strategies are being used to reduce
provement in the selection of persons for sur- the rate of advanced adenomas and carcinomas
veillance and screening is eminently feasible. in the interval between examinations, but proof
of the success of these modifications is needed.
C onclusions Approaches to the prevention of adenomas with
diet, lifestyle changes, and medications have been
Data reported during the previous decade are slow to evolve, since no clearly effective mea-
improving our understanding of the natural his- sures have been identified. Diets that are low in
tory and management of colonic adenomas and fat, regular physical exercise, maintenance of an
have identified strengths and exposed weakness- appropriate body-mass index, and avoidance of
es in the general approach to their detection and smoking remain critical to everyones health. As
removal. Colorectal cancers evolve by the malig- we move into an era in which increased benefit
nant transformation of conventional adenomas will be required from health carerelated expen-
and sessile serrated polyps or adenomas. Studies ditures, improvements in risk stratification, ad-
of the prevalence of adenomas have shown that enoma detection, surveillance intervals, and up-
they are identified in as many as 50% of asymp- take of screening should hasten our journey on
tomatic persons who undergo screening by means the pathway to prevention of colorectal cancer as
of colonoscopy or CT colonography; 3.4 to 7.6% a common disease.
n engl j med 374;11 nejm.org March 17, 2016 1073
The New England Journal of Medicine
Downloaded from nejm.org at CALIF INSTITUTE OF TECHNOLOGY on March 16, 2016. For personal use only. No other uses without permission.
Copyright 2016 Massachusetts Medical Society. All rights reserved.
The n e w e ng l a n d j o u r na l of m e dic i n e
Disclosure forms provided by the author are available with the I thank Dr. Emma Du for assistance with preparation of the
full text of this article at NEJM.org. figures and Mr. Clarence Sandbakken for research assistance.
References
1. Levine JS, Ahnen DJ. Adenomatous genetic testing in hereditary colorectal nography: a longitudinal study of natural
polyps of the colon. N Engl J Med 2006; cancer. Gastroenterology 2015;149(5):1191- history. Lancet Oncol 2013;14:711-20.
355:2551-7. 203.e2. 29. Hassan C, Pickhardt PJ, Rex DK. A re-
2. Cancer facts & figures 2016. Atlanta: 16. Luzzatto L, Pandolfi PP. Causality sect and discard strategy would improve
American Cancer Society, 2016 (http://www and chance in the development of cancer. cost-effectiveness of colorectal cancer
.cancer.org/acs/groups/content/@research/ N Engl J Med 2015;373:84-8. screening. Clin Gastroenterol Hepatol
documents/document/acspc-047079.pdf). 17. Sweetser S, Smyrk TC, Sinicrope FA. 2010;8:865-9.
3. Colorectal cancer facts & figures Serrated colon polyps as precursors to 30. ASGE Technology Committee. ASGE
2014-2016. Atlanta: American Cancer colorectal cancer. Clin Gastroenterol Technology Committee systematic review
Society, 2014 (http://www.cancer.org/acs/ Hepatol 2013;11:760-7. and meta-analysis assessing the ASGE
groups/content/documents/document/acspc 18. Kahi CJ, Hewett DG, Norton DL, Eckert PIVI thresholds for adopting real-time
-042280.pdf). GJ, Rex DK. Prevalence and variable de- endoscopic assessment of the histology of
4. Lieberman DA, Williams JL, Holub JL, tection of proximal colon serrated polyps diminutive colorectal polyps. Gastroin-
et al. Race, ethnicity, and sex affect risk for during screening colonoscopy. Clin Gas- test Endosc 2015;81(3):502.e1-502.e16.
polyps >9 mm in average-risk individuals. troenterol Hepatol 2011;9:42-6. 31. Lieberman DA, Holub JL, Morris CD,
Gastroenterology 2014;147:351-8. 19. Nishihara R, Wu K, Lochhead P, et al. Logan J, Williams JL, Carney P. Low rate
5. Imperiale TF, Ransohoff DF, Itzkowitz Long-term colorectal-cancer incidence and of large polyps (>9 mm) within 10 years
SH, et al. Multitarget stool DNA testing mortality after lower endoscopy. N Engl J after an adequate baseline colonoscopy
for colorectal-cancer screening. N Engl J Med 2013;369:1095-105. with no polyps. Gastroenterology 2014;
Med 2014;370:1287-97. 20. Stover DC, Ahnen D, Burt R, et al. Ser- 147:343-50.
6. Corley DA, Jensen CD, Marks AR, et al. rated polyps of the colon and rectum and 32. Corley DA. The future of colon cancer
Adenoma detection rate and risk of serrated polyposis. In: Bosman FT, Car- screening: what do we recommend and
colorectal cancer and death. N Engl J Med neiro F, Hruban RH, Theise ND, eds. will it be too much, too little, or just
2014;370:1298-306. WHO classification of tumours of the right? Gastroenterology 2011;141:1956-8.
7. Tsai FC, Strum WB. Prevalence of ad- digestive system. 4th ed. Lyon, France: 33. Dominitz JA, Robertson DJ. Tailoring
vanced adenomas in small and diminutive International Agency for Research on colonoscopic screening to individual risk.
colon polyps using direct measurement of Cancer, 2010:160-5. Gastroenterology 2014;147:264-6.
size. Dig Dis Sci 2011;56:2384-8. 21. Odze RD, Batts K, Goldstein N. In- 34. Lieberman DA, Rex DK, Winawer SJ,
8. Lieberman D, Moravec M, Holub J, terobserver variation in the diagnosis of Giardiello FM, Johnson DA, Levin TR.
Michaels L, Eisen G. Polyp size and ad- hyperplastic and serrated colonic polyps. Guidelines for colonoscopy surveillance
vanced histology in patients undergoing Mod Pathol 2007;20:Suppl 2:125A. after screening and polypectomy: a con-
colonoscopy screening: implications for 22. Hazewinkel Y, Tytgat KM, van Eeden S, sensus update by the US Multi-Society
CT colonography. Gastroenterology 2008; et al. Incidence of colonic neoplasia in pa- Task Force on Colorectal Cancer. Gastro-
135:1100-5. tients with serrated polyposis syndrome enterology 2012;143:844-57.
9. Barclay RL, Vicari JJ, Greenlaw RL. Ef- who undergo annual endoscopic surveil- 35. Martnez ME, Baron JA, Lieberman
fect of a time-dependent colonoscopic lance. Gastroenterology 2014;147:88-95. DA, et al. A pooled analysis of advanced
withdrawal protocol on adenoma detec- 23. Robert ME. The malignant colon polyp: colorectal neoplasia diagnoses after colo-
tion during screening colonoscopy. Clin diagnosis and therapeutic recommenda- noscopic polypectomy. Gastroenterology
Gastroenterol Hepatol 2008;6:1091-8. tions. Clin Gastroenterol Hepatol 2007;5: 2009;136:832-41.
10. Hornick JL, Odze RD. Polyps of the 662-7. 36. Pinsky PF, Schoen RE, Weissfeld JL, et
large intestine. In: Odze RD, Goldblum 24. Gupta S, Balasubramanian BA, Fu T, al. The yield of surveillance colonoscopy
JR, eds. Surgical pathology of the GI tract, Genta RM, Rockey DC, Lash R. Polyps by adenoma history and time to examina-
liver, biliary tract, and pancreas. 3rd ed. with advanced neoplasia are smaller in tion. Clin Gastroenterol Hepatol 2009;7:
Philadelphia: Elsevier/Saunders, 2015:621- the right than in the left colon: implica- 86-92.
42. tions for colorectal cancer screening. Clin 37. Laiyemo AO, Pinsky PF, Marcus PM,
11. Soetikno RM, Kaltenbach T, Rouse Gastroenterol Hepatol 2012;10:1395-401. et al. Utilization and yield of surveillance
RV, et al. Prevalence of nonpolypoid (flat 25. Benson M, Dureja P, Gopal D, Reichel- colonoscopy in the continued follow-up
and depressed) colorectal neoplasms in derfer M, Pfau PR. A comparison of op- study of the polyp prevention trial. Clin
asymptomatic and symptomatic adults. tical colonoscopy and CT colonography Gastroenterol Hepatol 2009;7:562-7.
JAMA 2008;299:1027-35. screening strategies in the detection and 38. Robertson DJ, Burke CA, Welch HG,
12. Fearon ER, Carethers JM. Molecular recovery of subcentimeter adenomas. Am et al. Using the results of a baseline and a
subtyping of colorectal cancer: time to ex- J Gastroenterol 2010;105:2578-85. surveillance colonoscopy to predict recur-
plore both intertumoral and intratumoral 26. Kim DH, Pickhardt PJ, Taylor AJ, et al. rent adenomas with high-risk characteris-
heterogeneity to evaluate patient outcome. CT colonography versus colonoscopy for tics. Ann Intern Med 2009;151:103-9.
Gastroenterology 2015;148:10-3. the detection of advanced neoplasia. N Engl 39. Lieberman DA, Weiss DG, Harford
13. Crockett SD, Snover DC, Ahnen DJ, J Med 2007;357:1403-12. WV, et al. Five-year colon surveillance af-
Baron JA. Sessile serrated adenomas: an 27. Hassan C, Pooler BD, Kim DH, et al. ter screening colonoscopy. Gastroenterol-
evidence-based guide to management. Clin Computed tomographic colonography for ogy 2007;133:1077-85.
Gastroenterol Hepatol 2015;13(1):11-26.e1. colorectal cancer: risk factors for the de- 40. Imperiale TF, Glowinski EA, Lin-
14. Jass JR. Classification of colorectal tection of advanced neoplasia. Cancer 2013; Cooper C, Larkin GN, Rogge JD, Ranso-
cancer based on correlation of clinical, 119:2549-54. hoff DF. Five-year risk of colorectal neopla-
morphological and molecular features. 28. Pickhardt PJ, Kim DH, Pooler BD, et sia after negative screening colonoscopy.
Histopathology 2007;50:113-30. al. Assessment of volumetric growth rates N Engl J Med 2008;359:1218-24.
15. Stoffel EM, Boland CR. Genetics and of small colorectal polyps with CT colo- 41. Brenner H, Chang-Claude J, Jansen L,
1074 n engl j med 374;11 nejm.org March 17, 2016
The New England Journal of Medicine
Downloaded from nejm.org at CALIF INSTITUTE OF TECHNOLOGY on March 16, 2016. For personal use only. No other uses without permission.
Copyright 2016 Massachusetts Medical Society. All rights reserved.
Colorectal Adenomas
Knebel P, Stock C, Hoffmeister M. Reduced vices Task Force, September 2015 (http:// detected at CT colonographic screening:
risk of colorectal cancer up to 10 years after www.uspreventiveservicestaskforce.org/ implications for appropriate polyp size
screening, surveillance, or diagnostic Page/Document/draft-recommendation thresholds for polypectomy versus sur-
colonoscopy. Gastroenterology 2014;146: -statement/aspirin-to-prevent-cardiovascular veillance. AJR Am J Roentgenol 2007;188:
709-17. -disease-and-cancer). 940-4.
42. Bressler B, Paszat LF, Chen Z, Roth- 54. Chan AT, Ladabaum U. Where do we 68. Hur C, Chung DC, Schoen RE, Gazelle
well DM, Vinden C, Rabeneck L. Rates of stand with aspirin for the prevention of GS. The management of small polyps
new or missed colorectal cancers after colorectal cancer? The USPSTF recommen- found by virtual colonoscopy: results of
colonoscopy and their risk factors: a pop- dations.Gastroenterology 2016;150:14-8. a decision analysis. Clin Gastroenterol
ulation-based analysis. Gastroenterology 55. Baron JA, Barry EL, Mott LA, et al. Hepatol 2007;5:237-44.
2007;132:96-102. A trial of calcium and vitamin D for the 69. Zauber AG, Winawer SJ, OBrien MJ,
43. Corley DA, Jensen CD, Marks AR, et al. prevention of colorectal adenomas. N Engl et al. Colonoscopic polypectomy and
Variation of adenoma prevalence by age, J Med 2015;373:1519-30. long-term prevention of colorectal-cancer
sex, race, and colon location in a large 56. Manson JE, Mayne ST, Clinton SK. deaths. N Engl J Med 2012;366:687-96.
population: implications for screening Vitamin D and prevention of cancer 70. Lakoff J, Paszat LF, Saskin R, Rabeneck
and quality programs. Clin Gastroenterol ready for prime time? N Engl J Med 2011; L. Risk of developing proximal versus dis-
Hepatol 2013;11:172-80. 364:1385-7. tal colorectal cancer after a negative colo-
44. Brenner H, Altenhofen L, Kretschmann 57. Kahi CJ, Rex DK, Imperiale TF. Screen- noscopy: a population-based study. Clin
J, et al. Trends in adenoma detection rates ing, surveillance, and primary prevention Gastroenterol Hepatol 2008;6:1117-21.
during the first 10 years of the German for colorectal cancer: a review of the re- 71. Lieberman DA. Screening for colorec-
screening colonoscopy program. Gastro- cent literature. Gastroenterology 2008; tal cancer. N Engl J Med 2009;361:1179-
enterology 2015;149(2):356-66.e1. 135:380-99. 87.
45. Ahnen DJ, Wade SW, Jones WF, et al. 58. Levin B, Lieberman DA, McFarland B, 72. Kaminski MF, Regula J, Kraszewska E,
The increasing incidence of young-onset et al. Screening and surveillance for the et al. Quality indicators for colonoscopy
colorectal cancer: a call to action. Mayo early detection of colorectal cancer and and the risk of interval cancer. N Engl J
Clin Proc 2014;89:216-24. adenomatous polyps, 2008: a joint guide- Med 2010;362:1795-803.
46. Abdelsattar ZM, Wong SL, Regenbo- line from the American Cancer Society, the 73. Frenette CT, Strum WB. Relative rates
gen SE, Jomaa DM, Hardiman KM, Hen- US Multi-Society Task Force on Colorec- of missed diagnosis for colonoscopy,
dren S. Colorectal cancer outcomes and tal Cancer, and the American College of barium enema, and flexible sigmoidos-
treatment pattern in patients too young Radiology. Gastroenterology 2008;134: copy in 379 patients with colorectal can-
for average-risk screening. Cancer 2014 1570-95. cer. J Gastrointest Cancer 2007;38:148-53.
January 25 (Epub ahead of print). 59. Qaseem A, Denberg TD, Hopkins RH 74. ASGE Standards of Practice Commit-
47. Pendergrass CJ, Edelstein DL, Hylind Jr, et al. Screening for colorectal cancer: tee. Complications of colonoscopy. Gas-
LM, et al. Occurrence of colorectal adeno- a guidance statement from the American trointest Endosc 2011;74:745-52.
mas in younger adults: an epidemiologic College of Physicians. Ann Intern Med 75. Shaukat A, Rector TS, Church TR, et al.
necropsy study. Clin Gastroenterol Hepa- 2012;156:378-86. Longer withdrawal time is associated with
tol 2008;6:1011-5. 60. Robertson DJ, Imperiale TF. Stool test- a reduced incidence of interval cancer af-
48. Rundle AG, Lebwohl B, Vogel R, ing for colorectal cancer screening. Gas- ter screening colonoscopy. Gastroenterol-
Levine S, Neugut AI. Colonoscopic troenterology 2015;149:1286-93. ogy 2015;149:952-7.
screening in average-risk individuals ages 61. Quintero E, Castells A, Bujanda L, et al. 76. Rex DK, Schoenfeld PS, Cohen J, et al.
40 to 49 vs 50 to 59 years. Gastroenterol- Colonoscopy versus fecal immunochemi- Quality indicators for colonoscopy. Am J
ogy 2008;134:1311-5. cal testing in colorectal-cancer screening. Gastroenterol 2015;110:72-90.
49. Giardiello FM, Allen JI, Axilbund JE, N Engl J Med 2012;366:697-706. 77. U.S. Preventive Services Task Force.
et al. Guidelines on genetic evaluation 62. Shaukat A, Mongin SJ, Geisser MS, Screening for colorectal cancer: U.S. Pre-
and management of Lynch syndrome: et al. Long-term mortality after screening ventive Services Task Force recommenda-
a consensus statement by the US Multi- for colorectal cancer. N Engl J Med 2013; tion statement. Ann Intern Med 2008;149:
Society Task Force on colorectal cancer. 369:1106-14. 627-37.
Gastroenterology 2014;147:502-26. 63. Schoen RE, Pinsky PF, Weissfeld JL, 78. van Hees F, Habbema DJF, Meester
50. Tao S, Hoffmeister M, Brenner H. et al. Colorectal-cancer incidence and mor- RG, et al. Should colorectal cancer screen-
Development and validation of a scoring tality with screening flexible sigmoidos- ing be considered in elderly persons with-
system to identify individuals at high copy. N Engl J Med 2012;366:2345-57. out previous screening. Ann Intern Med
risk for advanced colorectal neoplasms 64. Atkin WS, Edwards R, Kralj-Hans I, 2014;160:750-9.
who should undergo colonoscopy screen- et al. Once-only flexible sigmoidoscopy 79. Mittal S, Lin Y-L, Tan A, Kuo YF, El-
ing. Clin Gastroenterol Hepatol 2014;12: screening in prevention of colorectal can- Serag HB, Goodwin JS. Limited life ex-
478-85. cer: a multicentre randomised controlled pectancy among a subgroup of Medicare
51. Imperiale TF, Monahan PO, Stump trial. Lancet 2010;375:1624-33. beneficiaries receiving screening colonos-
TE, Glowinski EA, Ransohoff DF. Deriva- 65. Johnson CD, Chen MH, Toledano AY, copies. Clin Gastroenterol Hepatol 2014;
tion and validation of a scoring system for et al. Accuracy of CT colonography for 12(3):443-50.e1.
advanced colorectal neoplasia in asymp- detection of large adenomas and cancers. 80. Schoen RE, Pinsky PF, Weissfeld JL,
tomatic adults: a cross sectional study. N Engl J Med 2008;359:1207-17. et al. Utilization of surveillance colonos-
Ann Intern Med 2015;163:339-46. 66. Pickhardt PJ, Hain KS, Kim DH, Has- copy in community practice. Gastroenter-
52. Liao X, Lochhead P, Nishihara R, et al. san C. Low rates of cancer or high-grade ology 2010;138:73-81.
Aspirin use, tumor PIK3CA mutation, and dysplasia in colorectal polyps collected 81. Johnson MR, Grubber J, Grambow SC,
colorectal-cancer survival. N Engl J Med from computed tomography colonogra- et al. Physician non-adherence to colonos-
2012;367:1596-606. phy screening. Clin Gastroenterol Hepa- copy interval guidelines in the Veteran
53. Draft recommendation statement: as- tol 2010;8:610-5. Affairs healthcare system. Gastroenterol-
pirin to prevent cardiovascular disease and 67. Kim DH, Pickhardt PJ, Taylor AJ. ogy 2015;149:938-51.
cancer. Rockville, MD: U.S. Preventive Ser- Characteristics of advanced adenomas Copyright 2016 Massachusetts Medical Society.
n engl j med 374;11 nejm.org March 17, 2016 1075
The New England Journal of Medicine
Downloaded from nejm.org at CALIF INSTITUTE OF TECHNOLOGY on March 16, 2016. For personal use only. No other uses without permission.
Copyright 2016 Massachusetts Medical Society. All rights reserved.
Das könnte Ihnen auch gefallen
- Lynch Syndrome: Molecular Mechanism and Current Clinical PracticeVon EverandLynch Syndrome: Molecular Mechanism and Current Clinical PracticeNaohiro TomitaNoch keine Bewertungen
- Colorectal AdenomasDokument11 SeitenColorectal AdenomasMatias FlammNoch keine Bewertungen
- Adenomatous Polyps of The Colon 2006Dokument7 SeitenAdenomatous Polyps of The Colon 2006Anelise SchaedlerNoch keine Bewertungen
- Aisha Tabassum EtalDokument4 SeitenAisha Tabassum EtaleditorijmrhsNoch keine Bewertungen
- Pathophysiology of Colorectal CancerDokument2 SeitenPathophysiology of Colorectal CancerMp WhNoch keine Bewertungen
- Referat Bedah - QuwDokument14 SeitenReferat Bedah - QuwSaniaty TuankottaNoch keine Bewertungen
- 2009 0527 rs.1 PDFDokument5 Seiten2009 0527 rs.1 PDFpaolaNoch keine Bewertungen
- Git ArticleDokument6 SeitenGit ArticlePawan SapkotaNoch keine Bewertungen
- Practice Essentials: View Media GalleryDokument8 SeitenPractice Essentials: View Media GallerywzlNoch keine Bewertungen
- AmeloblastomaDokument4 SeitenAmeloblastomaMarïsa CastellonNoch keine Bewertungen
- Unusual Subtypes of Prostate CancerDokument12 SeitenUnusual Subtypes of Prostate CancerRonnie Alexander Reyes MartínezNoch keine Bewertungen
- Angiosacaaroma 1Dokument15 SeitenAngiosacaaroma 1Francisco ZurgaNoch keine Bewertungen
- JurnalDokument13 SeitenJurnalAnonymous OSTAJzYWDDNoch keine Bewertungen
- Polyp Genetics: Coen Laurens Klos, MD Sekhar Dharmarajan, MDDokument7 SeitenPolyp Genetics: Coen Laurens Klos, MD Sekhar Dharmarajan, MDMarjuani yusufNoch keine Bewertungen
- Near-Infrared Raman Spectroscopy For TheDokument12 SeitenNear-Infrared Raman Spectroscopy For TheAlberto Carlos Espinosa GaravitoNoch keine Bewertungen
- GB Cancer - Radiologic-Pathologic CorrelationDokument20 SeitenGB Cancer - Radiologic-Pathologic CorrelationSamuel WidjajaNoch keine Bewertungen
- Oral Malignant MelanomaDokument3 SeitenOral Malignant MelanomaKrisna AugustianNoch keine Bewertungen
- Pathophysiology, Clinical Presentation, and Management of CC (2008)Dokument24 SeitenPathophysiology, Clinical Presentation, and Management of CC (2008)Miguel RamírezNoch keine Bewertungen
- Adenocarcinoma Borderline OvarioDokument18 SeitenAdenocarcinoma Borderline OvarioIsaac MaderoNoch keine Bewertungen
- HHS Public Access: Author ManuscriptDokument26 SeitenHHS Public Access: Author ManuscriptCherryNoch keine Bewertungen
- Ovarian Cancer - StatPearls - NCBI BookshelfDokument13 SeitenOvarian Cancer - StatPearls - NCBI BookshelfeeeeeeNoch keine Bewertungen
- CA Cervicales Poco ComunesDokument13 SeitenCA Cervicales Poco Comunesangelo marinoNoch keine Bewertungen
- Genetics and Bowel CancerDokument5 SeitenGenetics and Bowel Canceri can always make u smile :DNoch keine Bewertungen
- CR Pa 2 PDFDokument4 SeitenCR Pa 2 PDFmitaNoch keine Bewertungen
- J Omsc 2020 100166Dokument5 SeitenJ Omsc 2020 100166Gisela LalitaNoch keine Bewertungen
- Molecular Genetics of Colorectal CancerDokument6 SeitenMolecular Genetics of Colorectal Cancermuhammad rizqi romadlonNoch keine Bewertungen
- 6 Neck DissectionDokument9 Seiten6 Neck DissectionAnne MarieNoch keine Bewertungen
- ACC Overview From UVADokument2 SeitenACC Overview From UVALuciaTrinovenaLaseNoch keine Bewertungen
- 1 s2.0 S0002939419300625 Main PDFDokument9 Seiten1 s2.0 S0002939419300625 Main PDFAsti DwiningsihNoch keine Bewertungen
- The Small Fatal Choroidal Melanoma Study. A Survey by The European Ophthalmic Oncology GroupDokument9 SeitenThe Small Fatal Choroidal Melanoma Study. A Survey by The European Ophthalmic Oncology GroupAsti DwiningsihNoch keine Bewertungen
- Current Diagnosis and Management of Retroperitoneal SarcomaDokument11 SeitenCurrent Diagnosis and Management of Retroperitoneal SarcomaMaximiliano TorresNoch keine Bewertungen
- 45657Dokument28 Seiten45657zoxpop1980Noch keine Bewertungen
- NEJMhereditarycolorectalcancer PDFDokument14 SeitenNEJMhereditarycolorectalcancer PDF송란다Noch keine Bewertungen
- Polymorphous Low Grade Adenocarcinoma of The Parotid in A TeenagerDokument4 SeitenPolymorphous Low Grade Adenocarcinoma of The Parotid in A Teenagersara luciaNoch keine Bewertungen
- Articulo 1Dokument17 SeitenArticulo 1Andrea NeriaNoch keine Bewertungen
- Current Controversies in The Management of Malignant Parotid TumorsDokument8 SeitenCurrent Controversies in The Management of Malignant Parotid TumorsDirga Rasyidin LNoch keine Bewertungen
- ZLJ 209Dokument11 SeitenZLJ 209afg_19Noch keine Bewertungen
- Review: Colorectal Polyps and Polyposis SyndromesDokument15 SeitenReview: Colorectal Polyps and Polyposis SyndromesSilvana María Espinoza CuadrosNoch keine Bewertungen
- CCarcinoma Ex Adenoma Pleomorfo - Una Revisión Integral de Clínicas, Patológicas y Molecular de DatosDokument9 SeitenCCarcinoma Ex Adenoma Pleomorfo - Una Revisión Integral de Clínicas, Patológicas y Molecular de Datoswilson nicolasNoch keine Bewertungen
- Leiomyosarcoma PenisDokument4 SeitenLeiomyosarcoma PenisMuneer KhalamNoch keine Bewertungen
- Department of Ophthalmology Faculty of Medicine Andalas University / DR. M. Djamil Hospital - PADANGDokument10 SeitenDepartment of Ophthalmology Faculty of Medicine Andalas University / DR. M. Djamil Hospital - PADANGFaimmatul SyuhadaNoch keine Bewertungen
- Ovarian Malignant Germ Cell Tumors PDFDokument26 SeitenOvarian Malignant Germ Cell Tumors PDFFernanda RiveraNoch keine Bewertungen
- Jadp 09 321Dokument8 SeitenJadp 09 321Diornald MogiNoch keine Bewertungen
- Adrenal Cortical TumorsDokument8 SeitenAdrenal Cortical TumorsSabrina whtNoch keine Bewertungen
- Review Article: Cancers of The Appendix: Review of The LiteraturesDokument7 SeitenReview Article: Cancers of The Appendix: Review of The LiteraturesMaman AhmadNoch keine Bewertungen
- Medsci 06 00031 PDFDokument113 SeitenMedsci 06 00031 PDFCarolina VillalobosNoch keine Bewertungen
- W de WenisimoDokument18 SeitenW de WenisimoBJ CarminatorNoch keine Bewertungen
- Pi Is 1555415518300035Dokument7 SeitenPi Is 1555415518300035Kawai MaharaniNoch keine Bewertungen
- Salivary Gland MalignanciesDokument69 SeitenSalivary Gland MalignanciesKessi VikaneswariNoch keine Bewertungen
- Invasive Squamous Cell Carcinoma: Comparison of Differentiation Grade and Tumour Depth by Anatomical Site in 1666 TumoursDokument8 SeitenInvasive Squamous Cell Carcinoma: Comparison of Differentiation Grade and Tumour Depth by Anatomical Site in 1666 TumoursEstefy Cerda MoscosoNoch keine Bewertungen
- J Amjoto 2019 102279Dokument5 SeitenJ Amjoto 2019 102279Gisela LalitaNoch keine Bewertungen
- Zebra FishDokument552 SeitenZebra FishmcvalledorNoch keine Bewertungen
- Testicular CancerDokument12 SeitenTesticular Cancerghost_724Noch keine Bewertungen
- Cancer y Celulas Madre 2022Dokument11 SeitenCancer y Celulas Madre 2022Jose EdgarNoch keine Bewertungen
- Ca de Colon y Polipos PDFDokument24 SeitenCa de Colon y Polipos PDFGabriela Zavaleta CamachoNoch keine Bewertungen
- Esophageal Cancer: Diagnosis and Management: Ai Zheng Aizheng Chinese Journal of Cancer October 2010Dokument13 SeitenEsophageal Cancer: Diagnosis and Management: Ai Zheng Aizheng Chinese Journal of Cancer October 2010Al VlaovicNoch keine Bewertungen
- Perfusion CT Imaging of Colorectal Cancer: Review ArticleDokument9 SeitenPerfusion CT Imaging of Colorectal Cancer: Review ArticleBambangSetiawanNoch keine Bewertungen
- Jurnal Kanker TestisDokument9 SeitenJurnal Kanker TestisDiatni FibriNoch keine Bewertungen
- Testis CancerDokument9 SeitenTestis CancerMuhammad Tawfiq ZamriNoch keine Bewertungen
- 624 PDFDokument9 Seiten624 PDFTri AryantiNoch keine Bewertungen
- Articulo 2 PDFDokument12 SeitenArticulo 2 PDFLucero BallesterosNoch keine Bewertungen
- Articulo 1Dokument13 SeitenArticulo 1Lucero BallesterosNoch keine Bewertungen
- Apoptosis Necrosis and OncosisDokument13 SeitenApoptosis Necrosis and OncosisLucero BallesterosNoch keine Bewertungen
- Golgi WoundDokument6 SeitenGolgi WoundLucero BallesterosNoch keine Bewertungen
- Golgi WoundDokument6 SeitenGolgi WoundLucero BallesterosNoch keine Bewertungen
- Articulo de DivulgacionDokument5 SeitenArticulo de DivulgacionLucero BallesterosNoch keine Bewertungen
- Lista de Verbos Irregulares en InglésDokument5 SeitenLista de Verbos Irregulares en Inglésaleslo8100% (3)
- Clinical Presentation, Diagnosis, and Staging of Colorectal CancerDokument20 SeitenClinical Presentation, Diagnosis, and Staging of Colorectal CancerJose Luis Marin CatacoraNoch keine Bewertungen
- ColonosDokument20 SeitenColonosshaneatateNoch keine Bewertungen
- PELAGIO-Cancer Module-NCM 112Dokument12 SeitenPELAGIO-Cancer Module-NCM 112Shiena Mae PelagioNoch keine Bewertungen
- Virtual Colonoscopy: in Colorectal Cancer ScreeningDokument27 SeitenVirtual Colonoscopy: in Colorectal Cancer ScreeningEwhied RuslamNoch keine Bewertungen
- Clinical Presentation, Diagnosis, and Staging of Colorectal CancerDokument36 SeitenClinical Presentation, Diagnosis, and Staging of Colorectal CancerjjjkkNoch keine Bewertungen
- Is A Traditional Colonoscopy or A Virtual Colonoscopy BetterDokument1 SeiteIs A Traditional Colonoscopy or A Virtual Colonoscopy BetterPaul JensenNoch keine Bewertungen
- American Cancer SocietyDokument41 SeitenAmerican Cancer SocietyEvi UtariNoch keine Bewertungen
- All Your Advanced Analysis Needs One Comprehensive Solution: StartDokument185 SeitenAll Your Advanced Analysis Needs One Comprehensive Solution: StartMitra MedistraNoch keine Bewertungen
- Assignment On Investigations-OncologyDokument12 SeitenAssignment On Investigations-OncologyAxsa AlexNoch keine Bewertungen
- Colonoscopy For DummiesDokument79 SeitenColonoscopy For Dummiesmike.krawulski9224100% (3)
- Colorectal Cancer OverviewDokument23 SeitenColorectal Cancer OverviewAlina AldeaNoch keine Bewertungen
- Clinical Presentation, Diagnosis, and Staging of Colorectal Cancer - UpToDate PDFDokument41 SeitenClinical Presentation, Diagnosis, and Staging of Colorectal Cancer - UpToDate PDFVali MocanuNoch keine Bewertungen
- Abdomen X RayDokument4 SeitenAbdomen X RaytimvrghsNoch keine Bewertungen
- Somatom Sessions 16-00079282-00270173 PDFDokument42 SeitenSomatom Sessions 16-00079282-00270173 PDF2vjNoch keine Bewertungen
- Colorectal Cancer Prevention and Early DetectionDokument33 SeitenColorectal Cancer Prevention and Early DetectionNesyah AyuNoch keine Bewertungen
- Group 4 - CT ScannerDokument29 SeitenGroup 4 - CT ScannerAnh TrầnNoch keine Bewertungen
- Colon CancerDokument7 SeitenColon CancerAdrian Paulo CastivaNoch keine Bewertungen
- Colon Polyps: Types, Diagnosis, and Treatment Options - Kaizen Gastro CareDokument2 SeitenColon Polyps: Types, Diagnosis, and Treatment Options - Kaizen Gastro CareKaizen Gastro CareNoch keine Bewertungen
- IFOBT For CRC ScreeningDokument91 SeitenIFOBT For CRC Screeningkillua0707Noch keine Bewertungen
- Clinical Presentation Diagnosis and Staging of Colorectal Cancer UpToDateDokument39 SeitenClinical Presentation Diagnosis and Staging of Colorectal Cancer UpToDateSean SialanaNoch keine Bewertungen
- Ohtas 15 1Dokument39 SeitenOhtas 15 1indahNoch keine Bewertungen
- Colonoscopi IndicationDokument26 SeitenColonoscopi IndicationTony HardianNoch keine Bewertungen
- Gastrointestinal Oncology.2011 PDFDokument469 SeitenGastrointestinal Oncology.2011 PDFpzlatin100% (1)
- Virtual Colonoscopy (VC, Also Called CT ColonographyDokument4 SeitenVirtual Colonoscopy (VC, Also Called CT ColonographyAbhay KumarNoch keine Bewertungen
- Medical Surgical NotesDokument17 SeitenMedical Surgical NotesNP YarebNoch keine Bewertungen
- Virtual ColonosDokument200 SeitenVirtual ColonosDiana VershyninaNoch keine Bewertungen
- Virtual Colonoscopy Vs Conventional Colonoscopy in Patients at High Risk of Colorectal Cancer - A Prospective Trial of 150 PatientsDokument8 SeitenVirtual Colonoscopy Vs Conventional Colonoscopy in Patients at High Risk of Colorectal Cancer - A Prospective Trial of 150 PatientsPari Pengda BaliNoch keine Bewertungen
- Colon CancerDokument5 SeitenColon Cancernicwil_wilnicNoch keine Bewertungen
- The Press Pa 022912Dokument20 SeitenThe Press Pa 022912Bangor PressNoch keine Bewertungen
- Role of CT Virtual Colonoscopy Versus Conventional Colonoscopy in The Evaluation of Colonic PolypsDokument8 SeitenRole of CT Virtual Colonoscopy Versus Conventional Colonoscopy in The Evaluation of Colonic PolypsPari Pengda BaliNoch keine Bewertungen