Das könnte Ihnen auch gefallen
- Health Insurance StudyDokument9 SeitenHealth Insurance StudyKiran BathiniNoch keine Bewertungen
- Roduct BookletDokument11 SeitenRoduct BookletDeepak MoreNoch keine Bewertungen
- Application For Accreditation of Hospital: National Accreditation Board For Hospitals and Healthcare ProvidersDokument16 SeitenApplication For Accreditation of Hospital: National Accreditation Board For Hospitals and Healthcare ProvidersAbdul BasitNoch keine Bewertungen
- Nursing Recruitment Skills Checklist: Guidance or DirectionDokument4 SeitenNursing Recruitment Skills Checklist: Guidance or DirectionKRIZZEL CATAMINNoch keine Bewertungen
- Star Family Health Optima 2020 PDFDokument1 SeiteStar Family Health Optima 2020 PDFRajat GuptaNoch keine Bewertungen
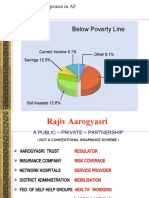
- Hospitalization Expenses in APDokument10 SeitenHospitalization Expenses in APSantosh GunduNoch keine Bewertungen
- Checklist For Esic/Esis HospitalsDokument6 SeitenChecklist For Esic/Esis HospitalssureesicNoch keine Bewertungen
- Star Out Patient Care Insurance PolicyV 1.0may2023Dokument37 SeitenStar Out Patient Care Insurance PolicyV 1.0may2023ठाकुर सूरज राणाNoch keine Bewertungen
- Rishi Valley Rural Health Centre Annual Report 2009-10Dokument4 SeitenRishi Valley Rural Health Centre Annual Report 2009-10Tk RamkumarNoch keine Bewertungen
- 2015-01-01 Norms For The Health Cadre - Sri LankaDokument83 Seiten2015-01-01 Norms For The Health Cadre - Sri LankaDoctors News86% (7)
- GMC Policy Benefits For StudentsDokument5 SeitenGMC Policy Benefits For StudentstrijtkaNoch keine Bewertungen
- CTS APE Endorsement LetterDokument3 SeitenCTS APE Endorsement LetterJoyce AnnNoch keine Bewertungen
- Welcome: National Level Meeting of Project Directors of Rural DevelopmentDokument115 SeitenWelcome: National Level Meeting of Project Directors of Rural DevelopmentAshwani PalNoch keine Bewertungen
- Medical Cover Guide-2Dokument5 SeitenMedical Cover Guide-2Temitope AdelowoNoch keine Bewertungen
- Final PSL Healthpolicy Wording PERSISTANT 2021-22Dokument38 SeitenFinal PSL Healthpolicy Wording PERSISTANT 2021-22AsifNoch keine Bewertungen
- Hospital Bill FormatDokument2 SeitenHospital Bill Formatsandee1910100% (1)
- Standards For Diagnostic RadiologyDokument25 SeitenStandards For Diagnostic Radiologymohadese EstajiNoch keine Bewertungen
- Nabh Application Dental ClinicDokument13 SeitenNabh Application Dental ClinicPriya HariNoch keine Bewertungen
- Dr. NTR Vaidya Seva: Quality Medicare For AllDokument48 SeitenDr. NTR Vaidya Seva: Quality Medicare For AllKiran Kumar BulikondaNoch keine Bewertungen
- Total Hip Replacement v4.1 Jan20Dokument3 SeitenTotal Hip Replacement v4.1 Jan20DindaNoch keine Bewertungen
- MCI One Pager Version 1.0 Oct 2020Dokument1 SeiteMCI One Pager Version 1.0 Oct 2020naval730107Noch keine Bewertungen
- Star Health Premier - Version 1.0 - Mar - 22Dokument33 SeitenStar Health Premier - Version 1.0 - Mar - 22Anoop AravindNoch keine Bewertungen
- CHI - One Pager - Version 1.3 - September 2021Dokument1 SeiteCHI - One Pager - Version 1.3 - September 2021ShihbNoch keine Bewertungen
- Senior Citizens Red Carpet Health Insurance Policy PDFDokument8 SeitenSenior Citizens Red Carpet Health Insurance Policy PDFrohit22221Noch keine Bewertungen
- Prudent Religare Employee Benefit ManualDokument24 SeitenPrudent Religare Employee Benefit ManualSheikh AtifNoch keine Bewertungen
- Form Medi-1Dokument4 SeitenForm Medi-1Abu Basir MandalNoch keine Bewertungen
- Admissions 2020 - General Category FeesDokument19 SeitenAdmissions 2020 - General Category FeesalishNoch keine Bewertungen
- Lia-Pre-Authorisation-Form - 20220117 2Dokument3 SeitenLia-Pre-Authorisation-Form - 20220117 2starspigotNoch keine Bewertungen
- Medical Aid Cover Guide 2018-FinalDokument5 SeitenMedical Aid Cover Guide 2018-FinalmakjnrNoch keine Bewertungen
- CHI One PagerDokument1 SeiteCHI One PagerPOS-ADSR TrackingNoch keine Bewertungen
- Top College FeesDokument227 SeitenTop College Feesarvindchopra3kNoch keine Bewertungen
- 2020 r2tmc Arta HandbookDokument140 Seiten2020 r2tmc Arta Handbookroblox accNoch keine Bewertungen
- AAC-Entry Level SeriesDokument48 SeitenAAC-Entry Level SeriesChandu PanditNoch keine Bewertungen
- Medical Report TemplateDokument1 SeiteMedical Report TemplateKimny PerezNoch keine Bewertungen
- I-Great Medi Care: Your Hassle-Free Personal Medical CareDokument24 SeitenI-Great Medi Care: Your Hassle-Free Personal Medical Carenrlyn_mduNoch keine Bewertungen
- Ms-001 (2) Clinical Priv Form Dental 2019Dokument4 SeitenMs-001 (2) Clinical Priv Form Dental 2019Athira RajanNoch keine Bewertungen
- Product Summary FOR Enhanced Hospital & Surgical Insurance AND Group Major Medical InsuranceDokument8 SeitenProduct Summary FOR Enhanced Hospital & Surgical Insurance AND Group Major Medical InsuranceAxel KruseNoch keine Bewertungen
- VBA-21-0960J-3-ARE Prostate Cancer PDFDokument3 SeitenVBA-21-0960J-3-ARE Prostate Cancer PDFCombat CraigNoch keine Bewertungen
- I-Medik RIDER Suite: Your One Stop Medical Protection SolutionDokument83 SeitenI-Medik RIDER Suite: Your One Stop Medical Protection SolutionainafaqeeraNoch keine Bewertungen
- Final - HOSPITAL BILL FORMAT PDFDokument2 SeitenFinal - HOSPITAL BILL FORMAT PDFH C85% (13)
- Final - Hospital Bill FormatDokument2 SeitenFinal - Hospital Bill FormatH C50% (2)
- Benefits Guide Colombia 2021Dokument10 SeitenBenefits Guide Colombia 2021Luis Carlos Gutierrez PedrazaNoch keine Bewertungen
- Income FlexCareDokument22 SeitenIncome FlexCareDarren ChenNoch keine Bewertungen
- Unnameed BroDokument29 SeitenUnnameed BroNanda RobbyNoch keine Bewertungen
- Family Health Optima Insurance PlanDokument1 SeiteFamily Health Optima Insurance PlanChetan tripathiNoch keine Bewertungen
- Singlife - Pre-Hospitalisation Form (PHF) - 2023Dokument1 SeiteSinglife - Pre-Hospitalisation Form (PHF) - 2023shemanth123Noch keine Bewertungen
- 2021 PPMP - Projects-HSFESP-FINALDokument20 Seiten2021 PPMP - Projects-HSFESP-FINALKimscey Yvan DZ SulitNoch keine Bewertungen
- Assistant Nurse Comp Check 2018Dokument3 SeitenAssistant Nurse Comp Check 2018pmnh nqps0% (1)
- Outpatient ClaimDokument1 SeiteOutpatient Claimtajuddin8Noch keine Bewertungen
- Star Health and Allied Insurance Company LimitedDokument6 SeitenStar Health and Allied Insurance Company LimitedPurna CharyNoch keine Bewertungen
- FHO - Revised - One PagerDokument1 SeiteFHO - Revised - One Pagersurya100% (1)
- Closed Medical Record ReviewDokument6 SeitenClosed Medical Record ReviewMuzna Iqbal50% (2)
- Benefits ManualDokument12 SeitenBenefits ManualPramod ApugolNoch keine Bewertungen
- Project - Vetecon 2 TermDokument18 SeitenProject - Vetecon 2 Termmathieulaid1Noch keine Bewertungen
- AXA-HOPEMedic2 XtraBrochure (Agency) (Sep2018)Dokument60 SeitenAXA-HOPEMedic2 XtraBrochure (Agency) (Sep2018)E-Qie BalNoch keine Bewertungen
- December 2019: Chemistry and Microscopy Results in One Report Question or Question Is Not ApplicableDokument4 SeitenDecember 2019: Chemistry and Microscopy Results in One Report Question or Question Is Not ApplicableImam Al-DoaibesNoch keine Bewertungen
- Business Model FINAL - Sahil VermaDokument43 SeitenBusiness Model FINAL - Sahil VermaParamjeet SinghNoch keine Bewertungen
- Annexure Panchkarma - 1st EditionDokument228 SeitenAnnexure Panchkarma - 1st EditionSmita SaxenaNoch keine Bewertungen
- CPG - Presentation 26.04.2018 - EnglishDokument46 SeitenCPG - Presentation 26.04.2018 - EnglishChuộtĐẻTrứngNoch keine Bewertungen
- Textbook of Urgent Care Management: Chapter 11, Urgent Care AccreditationVon EverandTextbook of Urgent Care Management: Chapter 11, Urgent Care AccreditationNoch keine Bewertungen
- 2 CGMP Meeting d1s3 Production Shah v3.0Dokument58 Seiten2 CGMP Meeting d1s3 Production Shah v3.0vsvsuresh2099100% (1)
- What's NanofiltrationDokument1 SeiteWhat's NanofiltrationdesNoch keine Bewertungen
- FILMTEC Membranes Water Chemistry and Pretreatment: Silica Scale PreventionDokument4 SeitenFILMTEC Membranes Water Chemistry and Pretreatment: Silica Scale PreventionMuthu KumarNoch keine Bewertungen
- SBR in Plant TechnologyDokument27 SeitenSBR in Plant TechnologydesNoch keine Bewertungen
- Certificate of FitnessDokument1 SeiteCertificate of FitnessdesNoch keine Bewertungen
- Rubia CordifoliaDokument7 SeitenRubia CordifoliadesNoch keine Bewertungen
- Chennai MTC Bus SheduleDokument13 SeitenChennai MTC Bus SheduledesNoch keine Bewertungen
- Pump & PressureDokument4 SeitenPump & PressuredesNoch keine Bewertungen
- Medical Certificate SampleDokument1 SeiteMedical Certificate Sampletacharya1Noch keine Bewertungen
- Bio. Growth On MemDokument2 SeitenBio. Growth On MemdesNoch keine Bewertungen
- Fouling SolutionsDokument3 SeitenFouling SolutionsdesNoch keine Bewertungen
- Asme Bpe PDFDokument17 SeitenAsme Bpe PDFJuan González LozanoNoch keine Bewertungen
- Membrane Rejection LevelsDokument2 SeitenMembrane Rejection LevelsdesNoch keine Bewertungen
- Electrodeionization (EDI) : Fact SheetDokument7 SeitenElectrodeionization (EDI) : Fact Sheetald3ano100% (1)
- Activated Carbon FiltrationDokument4 SeitenActivated Carbon FiltrationdesNoch keine Bewertungen
- Membrane Fouling - Corrective Actions: By: Gil K. Dhawan Ph.D. P.E., Applied Membranes, IncDokument2 SeitenMembrane Fouling - Corrective Actions: By: Gil K. Dhawan Ph.D. P.E., Applied Membranes, IncdesNoch keine Bewertungen
- Electrodeionization (EDI) : Fact SheetDokument7 SeitenElectrodeionization (EDI) : Fact Sheetald3ano100% (1)
- Membranes ProtectionDokument6 SeitenMembranes ProtectionsirmatuNoch keine Bewertungen
- Test For Determining Silt Density Index: EquipmentDokument2 SeitenTest For Determining Silt Density Index: EquipmentdesNoch keine Bewertungen
- Activated Carbon FiltrationDokument4 SeitenActivated Carbon FiltrationdesNoch keine Bewertungen
- ONE Compliance GLO 2016Dokument3 SeitenONE Compliance GLO 2016desNoch keine Bewertungen
- Apec WaterDokument3 SeitenApec WaterdesNoch keine Bewertungen
- Oxford English For Infomation Technology4Dokument1 SeiteOxford English For Infomation Technology4desNoch keine Bewertungen
- Oxford English For Infomation Technology5Dokument4 SeitenOxford English For Infomation Technology5desNoch keine Bewertungen
- KratavoveDokument1 SeiteKratavovedesNoch keine Bewertungen
- Oxford English For Infomation Technology 3Dokument5 SeitenOxford English For Infomation Technology 3desNoch keine Bewertungen
- Amar Chitra Katha-Panchatantra-Crows and Owls PDFDokument32 SeitenAmar Chitra Katha-Panchatantra-Crows and Owls PDFdes67% (3)
- Cryogenics and SpaceDokument1 SeiteCryogenics and SpacedesNoch keine Bewertungen
- Robots Are The Future For Mankind Due To Lack of ResourcesDokument1 SeiteRobots Are The Future For Mankind Due To Lack of ResourcesdesNoch keine Bewertungen
- NCP Loss of AppetiteDokument2 SeitenNCP Loss of AppetiteIris Balino100% (1)
- Fissured TongueDokument31 SeitenFissured Tonguenuratiqah_jasmiadNoch keine Bewertungen
- Orthopedic Clinics Na 2007 Vol 38 ScoliosisDokument102 SeitenOrthopedic Clinics Na 2007 Vol 38 ScoliosisChanina BlacksteinNoch keine Bewertungen
- Guillian-Barr e Syndrome - A Case StudyDokument11 SeitenGuillian-Barr e Syndrome - A Case StudyHecan ComeNoch keine Bewertungen
- Inservice Education Bio Medical Waste ManagementDokument56 SeitenInservice Education Bio Medical Waste ManagementPraveen John Edward William100% (1)
- 1 s2.0 S0377123714001750 MainDokument7 Seiten1 s2.0 S0377123714001750 MainMarlon Cespedes AlccaNoch keine Bewertungen
- Regulatory Requirements For Clinical Trials in IndiDokument8 SeitenRegulatory Requirements For Clinical Trials in IndiMahendran NNoch keine Bewertungen
- Review Notes 2000 - CardiologyDokument58 SeitenReview Notes 2000 - Cardiologyeliaszavaleta100% (1)
- Personalitati in MedicinaDokument10 SeitenPersonalitati in MedicinaIvanka MedescuNoch keine Bewertungen
- Drug Fridge - Cleaning Procedure: WCDHB-PN-0061Dokument2 SeitenDrug Fridge - Cleaning Procedure: WCDHB-PN-0061Rika VerdikaNoch keine Bewertungen
- Head Injury: Tahun Dua Sem. Satu M.S.GanesanDokument32 SeitenHead Injury: Tahun Dua Sem. Satu M.S.GanesanThines Noloc'zNoch keine Bewertungen
- NCM 105 Notes 5 StudentsDokument11 SeitenNCM 105 Notes 5 StudentsRI NANoch keine Bewertungen
- Advanced Mechanical VentilationDokument96 SeitenAdvanced Mechanical VentilationMukhtar KhanNoch keine Bewertungen
- Procedural Verification ProtocolDokument4 SeitenProcedural Verification ProtocolPops IcunaNoch keine Bewertungen
- Restraint Soctrative With AnswersDokument5 SeitenRestraint Soctrative With AnswersKarren FernandezNoch keine Bewertungen
- Intranasal Steroids in PediatricsDokument39 SeitenIntranasal Steroids in PediatricsKishore ChandkiNoch keine Bewertungen
- Alcohol Treatment CenterDokument54 SeitenAlcohol Treatment CenterAnonymous ntDYikdyNoch keine Bewertungen
- 24 Hour Urine CollectionDokument3 Seiten24 Hour Urine CollectionFatima Neshreen SarahadilNoch keine Bewertungen
- Classification and Management of Subcutaneous EmphysemaDokument5 SeitenClassification and Management of Subcutaneous EmphysemaTaufik Gumilar WahyudinNoch keine Bewertungen
- Rights and Obligations of PatientsDokument10 SeitenRights and Obligations of PatientsRey BenítezNoch keine Bewertungen
- Junard M. Lu Hap, RN: #51 Champaca Lapu-Lapu Street Brgy. Dadiangas East, General Santos City Contact Number 050-310-9586Dokument6 SeitenJunard M. Lu Hap, RN: #51 Champaca Lapu-Lapu Street Brgy. Dadiangas East, General Santos City Contact Number 050-310-9586Junard M. Lu HapNoch keine Bewertungen
- Beyond Schizophrenia (2016) PDFDokument251 SeitenBeyond Schizophrenia (2016) PDFRicardo HungriaNoch keine Bewertungen
- Nursing Care Plan: CirrhosisDokument11 SeitenNursing Care Plan: CirrhosisneuronurseNoch keine Bewertungen
- Nursing Assessment 1Dokument70 SeitenNursing Assessment 1Amira AttyaNoch keine Bewertungen
- 01 - Activity 01Dokument2 Seiten01 - Activity 01Denice VicenteNoch keine Bewertungen
- Meningitis: Laguitao, Ayra B. LLANETA, Marissa Angeline BDokument12 SeitenMeningitis: Laguitao, Ayra B. LLANETA, Marissa Angeline BAyra Batore Laguitao100% (1)
- Category 17 Best AD Content Entire Publication-Aug 7 Issue-St Joseph News PressDokument36 SeitenCategory 17 Best AD Content Entire Publication-Aug 7 Issue-St Joseph News Pressamy.brantNoch keine Bewertungen
- Health Information Management Technology: An Applied ApproachDokument104 SeitenHealth Information Management Technology: An Applied ApproachJenniferNoch keine Bewertungen
- Celecoxib (Drug Study)Dokument3 SeitenCelecoxib (Drug Study)Franz.thenurse6888100% (1)
- Anadrol PIDokument8 SeitenAnadrol PIAnabolmasteRNoch keine Bewertungen