Das könnte Ihnen auch gefallen
- Pheochromocytomas, Paragangliomas and Disorders of the Sympathoadrenal System: Clinical Features, Diagnosis and ManagementVon EverandPheochromocytomas, Paragangliomas and Disorders of the Sympathoadrenal System: Clinical Features, Diagnosis and ManagementLewis LandsbergNoch keine Bewertungen
- Review: Diagnosis and Management of Antiphospholipid Syndrome in PregnancyDokument7 SeitenReview: Diagnosis and Management of Antiphospholipid Syndrome in PregnancyFebri Yudha Adhi KurniawanNoch keine Bewertungen
- Nephrotic Syndrome: Symposium: NephrologyDokument4 SeitenNephrotic Syndrome: Symposium: Nephrologypramuliansyah haqNoch keine Bewertungen
- SD Nefrotico en AdultosDokument6 SeitenSD Nefrotico en AdultosSebastian Ignacio Vega GonzalezNoch keine Bewertungen
- Nephrotic Syndrome Children PDFDokument11 SeitenNephrotic Syndrome Children PDFesdl86Noch keine Bewertungen
- Michels 2017Dokument12 SeitenMichels 2017Nisa TaslimNoch keine Bewertungen
- Recent Update in The Management of Childhood Nephr PDFDokument8 SeitenRecent Update in The Management of Childhood Nephr PDFREHNUMA URMINoch keine Bewertungen
- 05 - Sle, DMZ, PHSDokument157 Seiten05 - Sle, DMZ, PHSG SNoch keine Bewertungen
- AAFP Marzo 2016 Sindrome NefroticoDokument7 SeitenAAFP Marzo 2016 Sindrome NefroticoAntonio MoncadaNoch keine Bewertungen
- Afp 20180601 P 741Dokument9 SeitenAfp 20180601 P 741Deni IrwandiNoch keine Bewertungen
- Paper English 3 - DONEDokument21 SeitenPaper English 3 - DONESarita AmeliaNoch keine Bewertungen
- LimfadenopatiDokument8 SeitenLimfadenopatiZulkarnain PrakosoNoch keine Bewertungen
- Causes and Pathophysiology of Nephrotic Syndrome IDokument14 SeitenCauses and Pathophysiology of Nephrotic Syndrome ISundas EjazNoch keine Bewertungen
- HELLP SYNDROME - A Diagnostic Dilemma PDFDokument5 SeitenHELLP SYNDROME - A Diagnostic Dilemma PDFragil sekarNoch keine Bewertungen
- Systemic Lupus Erythematosus: Authors: Maliha F ShaikhDokument6 SeitenSystemic Lupus Erythematosus: Authors: Maliha F ShaikhAnonymous hF5zAdvwCCNoch keine Bewertungen
- Pediatrik LeukemiasDokument14 SeitenPediatrik LeukemiasLefrina GusrianiiNoch keine Bewertungen
- Ed Neutr 2022Dokument32 SeitenEd Neutr 2022Marga KouryNoch keine Bewertungen
- Wilm's TumorDokument4 SeitenWilm's TumorWilliam NewleafNoch keine Bewertungen
- Myelodysplastic Syndromes PDFDokument14 SeitenMyelodysplastic Syndromes PDFAdriian PortilloNoch keine Bewertungen
- Aplastic Anemia: Review of Etiology and TreatmentDokument7 SeitenAplastic Anemia: Review of Etiology and TreatmentCleber MaiaNoch keine Bewertungen
- Congenital Myopathies: BackgroundDokument34 SeitenCongenital Myopathies: BackgroundHerry GunawanNoch keine Bewertungen
- Pituitary Apoplexy Pathophysiology Diagnosis and MDokument6 SeitenPituitary Apoplexy Pathophysiology Diagnosis and MlathifatulNoch keine Bewertungen
- Calvin Damanik, DR, SPPD: Departement Penyakit Dalam Fak Kedokteran Umi MedDokument37 SeitenCalvin Damanik, DR, SPPD: Departement Penyakit Dalam Fak Kedokteran Umi MedMaria lestari harianjaNoch keine Bewertungen
- Hematology Topics 16-20Dokument20 SeitenHematology Topics 16-20Angelo Jude CobachaNoch keine Bewertungen
- Lupus ErythematosusDokument5 SeitenLupus ErythematosusAditya DarmawanNoch keine Bewertungen
- Acute Leukemia in ChildrenDokument15 SeitenAcute Leukemia in ChildrenSabrina JonesNoch keine Bewertungen
- Afp 20140501 P 731Dokument8 SeitenAfp 20140501 P 731metabolismeproteinNoch keine Bewertungen
- Anemia AplasticaDokument14 SeitenAnemia Aplasticajesus.alfonso.sanchez.herreraNoch keine Bewertungen
- MR 28 Agustus-1Dokument7 SeitenMR 28 Agustus-1BramaNoch keine Bewertungen
- IM Bone Marrow Failure Aplastic AnemiaDokument6 SeitenIM Bone Marrow Failure Aplastic AnemiaKrisha BalorioNoch keine Bewertungen
- Seminar: Lionel Adès, Raphael Itzykson, Pierre FenauxDokument14 SeitenSeminar: Lionel Adès, Raphael Itzykson, Pierre FenauxAchmad Teguh Fikri PratamaNoch keine Bewertungen
- 1476 1503 1 PB PDFDokument8 Seiten1476 1503 1 PB PDFArief GusmanNoch keine Bewertungen
- Hereditaryhemorrhagic TelangiectasiaDokument18 SeitenHereditaryhemorrhagic TelangiectasiaalecsaNoch keine Bewertungen
- Noonan Syndrome (Am Fam Physician. 2014 PDFDokument7 SeitenNoonan Syndrome (Am Fam Physician. 2014 PDFKhalila DiantiNoch keine Bewertungen
- Nephrotic SyndromeDokument37 SeitenNephrotic SyndromeJon Adonis GozunNoch keine Bewertungen
- 32 Saha EtalDokument3 Seiten32 Saha EtaleditorijmrhsNoch keine Bewertungen
- Nephrotic Syndrome: Department of Pediatrics The First Affiliated Hospital Sun Yat-Sen UniversityDokument67 SeitenNephrotic Syndrome: Department of Pediatrics The First Affiliated Hospital Sun Yat-Sen UniversityBuwaneka VidanageNoch keine Bewertungen
- Anesthesia For Systemic Lupus Erythematosus ReviewDokument12 SeitenAnesthesia For Systemic Lupus Erythematosus ReviewAnonymous x75qV3lGNoch keine Bewertungen
- A695 PDFDokument9 SeitenA695 PDFFauzi NoviaNoch keine Bewertungen
- Aplastic AnemiaDokument26 SeitenAplastic AnemiaIrina Moldovan100% (1)
- Systemic Lupus ErythematosusDokument12 SeitenSystemic Lupus ErythematosusEdwin WardhanaNoch keine Bewertungen
- SD Paraneoplasico NeurologicoDokument11 SeitenSD Paraneoplasico NeurologicoMidori OkaNoch keine Bewertungen
- Neurooncology of Familial Cancer SyndromesDokument10 SeitenNeurooncology of Familial Cancer SyndromesMădălina SimionNoch keine Bewertungen
- The Term Aplastic Anemia Indicates: Pancytopenia in The PresenceDokument34 SeitenThe Term Aplastic Anemia Indicates: Pancytopenia in The PresenceKhadar mohamedNoch keine Bewertungen
- Aplastic AnemiaDokument5 SeitenAplastic Anemiascremo_xtremeNoch keine Bewertungen
- Types of Anemia Part2Dokument6 SeitenTypes of Anemia Part2April Mae Magos LabradorNoch keine Bewertungen
- Lupus Full PDFDokument12 SeitenLupus Full PDFEzza noerNoch keine Bewertungen
- Aplastic Anemia, 2008Dokument10 SeitenAplastic Anemia, 2008j.doe.hex_87Noch keine Bewertungen
- Systemic Lupus ErythematosusDokument28 SeitenSystemic Lupus ErythematosusLuiz Fernando Alves FerreiraNoch keine Bewertungen
- Sindrome NefroticoDokument8 SeitenSindrome NefroticoRudy Espejo del ArcaNoch keine Bewertungen
- Lupus Nephritis: Disease of The MonthDokument12 SeitenLupus Nephritis: Disease of The MonthHanik FiriaNoch keine Bewertungen
- Antiphospholipid Syndrome (Aps) and PregnancyDokument36 SeitenAntiphospholipid Syndrome (Aps) and Pregnancyskeisham11Noch keine Bewertungen
- 74 Year Old Woman With Fatigue, Anorexia, and AbdoDokument6 Seiten74 Year Old Woman With Fatigue, Anorexia, and AbdoRamiro Arraya MierNoch keine Bewertungen
- MEHU525 - U2 - T12 - Nephrotic SyndromeDokument13 SeitenMEHU525 - U2 - T12 - Nephrotic SyndromeJorge OtoyaNoch keine Bewertungen
- Anemi Aplastik Dan MielodisplasiaDokument34 SeitenAnemi Aplastik Dan MielodisplasiaRoby KieranNoch keine Bewertungen
- Naranjo 2017Dokument13 SeitenNaranjo 2017enriquegarciagalianaNoch keine Bewertungen
- 18 NephroticsyndromeDokument7 Seiten18 NephroticsyndromeKim's FamilyNoch keine Bewertungen
- Insulinoma: Tumores Neuroendocrinos GastroenteropancreáticosDokument6 SeitenInsulinoma: Tumores Neuroendocrinos GastroenteropancreáticosRafaella Valverde VilchrrezNoch keine Bewertungen
- Immune Hematology: Diagnosis and Management of Autoimmune CytopeniasVon EverandImmune Hematology: Diagnosis and Management of Autoimmune CytopeniasJenny M. DespotovicNoch keine Bewertungen
- p479 PDFDokument7 Seitenp479 PDFsDamnNoch keine Bewertungen
- Moderate Sedation 05Dokument39 SeitenModerate Sedation 05drkameshNoch keine Bewertungen
- Radiographic ViewsDokument9 SeitenRadiographic ViewssDamnNoch keine Bewertungen
- Lapjag 11-17 FADDokument12 SeitenLapjag 11-17 FADsDamnNoch keine Bewertungen
- Classification of Headache and Facial Pain PDFDokument8 SeitenClassification of Headache and Facial Pain PDFsDamnNoch keine Bewertungen
- Nephrotic Syndrome: BackgroundDokument25 SeitenNephrotic Syndrome: BackgroundsDamnNoch keine Bewertungen
- BMJ 336 7654 CR 01185 PDFDokument5 SeitenBMJ 336 7654 CR 01185 PDFsDamnNoch keine Bewertungen
- Herpes GuideDokument12 SeitenHerpes GuidesDamnNoch keine Bewertungen
- What Is Twin-To-Twin Transfusion Syndrome?Dokument8 SeitenWhat Is Twin-To-Twin Transfusion Syndrome?sDamnNoch keine Bewertungen
- Herpes Zoster Vaccine Fact SheetDokument8 SeitenHerpes Zoster Vaccine Fact SheetsDamnNoch keine Bewertungen
- Unud-228-1060756295-Daftar PustakaDokument4 SeitenUnud-228-1060756295-Daftar PustakaBertus AwNoch keine Bewertungen
- Valacyclovir Development Treatment and PharmacokineticsDokument8 SeitenValacyclovir Development Treatment and PharmacokineticssDamnNoch keine Bewertungen
- Approach To The Patient With Hematuria: Paul D. Simmons, MD St. Mary's Family Medicine Residency Grand JunctionDokument41 SeitenApproach To The Patient With Hematuria: Paul D. Simmons, MD St. Mary's Family Medicine Residency Grand JunctionMichael Spica RampangileiNoch keine Bewertungen
- Judul Jurnal2Dokument1 SeiteJudul Jurnal2sDamnNoch keine Bewertungen
- HematuriaDokument24 SeitenHematuriaHawania IINoch keine Bewertungen
- Lumbar Disc HerniationDokument19 SeitenLumbar Disc HerniationsDamnNoch keine Bewertungen
- Differential Diagnosis of HematuriaDokument5 SeitenDifferential Diagnosis of HematuriasDamnNoch keine Bewertungen
- JudulDokument1 SeiteJudulsDamnNoch keine Bewertungen
- HematuriaDokument4 SeitenHematuriasDamnNoch keine Bewertungen
- Lumbar Disc HerniationDokument19 SeitenLumbar Disc HerniationRabie'ahBahananNoch keine Bewertungen
- Streptococcal Tonsillitis As A Cause of Urticaria Tonsillitis and UrticariaDokument5 SeitenStreptococcal Tonsillitis As A Cause of Urticaria Tonsillitis and UrticariasDamnNoch keine Bewertungen
- Contraindications To Air TravelDokument15 SeitenContraindications To Air TravelsDamnNoch keine Bewertungen
- Antimicrob. Agents Chemother. 2004 Gosling 3642 3Dokument2 SeitenAntimicrob. Agents Chemother. 2004 Gosling 3642 3sDamnNoch keine Bewertungen
- Blood Pressure LevelsDokument4 SeitenBlood Pressure LevelsHeart of the Valley, Pediatric CardiologyNoch keine Bewertungen
- The Merapi's Eruption Refugees Emergency Care. Prevalence of Refugees Reported at UPN "Veteran"Dokument2 SeitenThe Merapi's Eruption Refugees Emergency Care. Prevalence of Refugees Reported at UPN "Veteran"sDamnNoch keine Bewertungen
- BP Limits Chart 0112Dokument4 SeitenBP Limits Chart 0112sDamnNoch keine Bewertungen
- Allergy, Asthma & Clinical Immunology: Urticaria and InfectionsDokument12 SeitenAllergy, Asthma & Clinical Immunology: Urticaria and InfectionssDamnNoch keine Bewertungen
- JurnalDokument2 SeitenJurnalsDamnNoch keine Bewertungen
- Format Follow UP BangsalDokument1 SeiteFormat Follow UP BangsalsDamnNoch keine Bewertungen
- Anatomic Therapy PDFDokument364 SeitenAnatomic Therapy PDFrahul_choubey_9Noch keine Bewertungen
- Nursing Diagnosis Nursing Intervention Rationale Exchange: Prioritized Nursing Problem For Choanal AtresiaDokument9 SeitenNursing Diagnosis Nursing Intervention Rationale Exchange: Prioritized Nursing Problem For Choanal AtresiaJinaan MahmudNoch keine Bewertungen
- Iron Deficiency AnemiaDokument4 SeitenIron Deficiency AnemiaWiljohn de la CruzNoch keine Bewertungen
- Cerebral Salt Wasting SyndromeDokument6 SeitenCerebral Salt Wasting SyndromeAbi ArifiNoch keine Bewertungen
- Learning Area Grade Level Quarter Date: English 9 4Dokument4 SeitenLearning Area Grade Level Quarter Date: English 9 4Kim So-Hyun100% (1)
- TB in Special SituationsDokument49 SeitenTB in Special SituationsVipul KumarNoch keine Bewertungen
- Eduskills Listening Mock Test Day 3 QNDokument15 SeitenEduskills Listening Mock Test Day 3 QNselvarajmarithai1432Noch keine Bewertungen
- PediatricsDokument21 SeitenPediatricsManoj KumarNoch keine Bewertungen
- Assignment 1 Part 1 A1Dokument10 SeitenAssignment 1 Part 1 A1garrenaNoch keine Bewertungen
- CH 071 Acute Kidney Injury in ChildrenDokument9 SeitenCH 071 Acute Kidney Injury in Childrenarun babuNoch keine Bewertungen
- Nursing Care Plan Placenta PreviaDokument2 SeitenNursing Care Plan Placenta PreviaApril Ann HortilanoNoch keine Bewertungen
- Drug Study FINALDokument32 SeitenDrug Study FINALhomeworkping1Noch keine Bewertungen
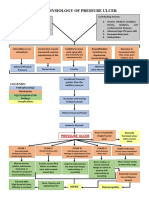
- Pathophysiology of Pressure UlcerDokument1 SeitePathophysiology of Pressure UlcerSTORAGE FILENoch keine Bewertungen
- Dilated CardiomyopathyDokument23 SeitenDilated CardiomyopathyYanna Habib-MangotaraNoch keine Bewertungen
- Histological Features of Candidiasis: By:Mamdouh Dagsh Alshrifi ID:321103259Dokument14 SeitenHistological Features of Candidiasis: By:Mamdouh Dagsh Alshrifi ID:321103259Mamdouh D AlrwailiNoch keine Bewertungen
- Normal Digestion / Absorption of FatDokument5 SeitenNormal Digestion / Absorption of FatMarc Michael Dela CruzNoch keine Bewertungen
- Garssen, 2004 - Physical Training and Fatigue, Fitness, and Quality of Life in Guillain-Barre Syndrome and CIDPDokument3 SeitenGarssen, 2004 - Physical Training and Fatigue, Fitness, and Quality of Life in Guillain-Barre Syndrome and CIDPkarinaNoch keine Bewertungen
- Paedia - Dr. RehabDokument173 SeitenPaedia - Dr. RehabMohammed Saad NabhanNoch keine Bewertungen
- Life Is A Continous Process of AdjustmentDokument78 SeitenLife Is A Continous Process of AdjustmentGulmoharNoch keine Bewertungen
- CarmelliDokument5 SeitenCarmellinana PrimasantiNoch keine Bewertungen
- CHN Epidemiology QUIZDokument1 SeiteCHN Epidemiology QUIZJammeNoch keine Bewertungen
- Presented by DR Muhammad Usman Senior Lecturer BUCPT: Introduction To Screening For Referral in Physical TherapyDokument27 SeitenPresented by DR Muhammad Usman Senior Lecturer BUCPT: Introduction To Screening For Referral in Physical Therapysaba ramzanNoch keine Bewertungen
- Lapp Jan2020Dokument88 SeitenLapp Jan2020Siti RojanahNoch keine Bewertungen
- "COVID Is Fake Sick Actually Have Influenza A or B", by Dr. Derek KnaussDokument2 Seiten"COVID Is Fake Sick Actually Have Influenza A or B", by Dr. Derek KnaussSANDRA BAGGNoch keine Bewertungen
- Limping Child: Department of Orthopaedics Afmc, PuneDokument101 SeitenLimping Child: Department of Orthopaedics Afmc, Punerithesh ramachandranNoch keine Bewertungen
- 1 InfectionDokument41 Seiten1 InfectionIMA MSN TNNoch keine Bewertungen
- Physical Examination FormDokument4 SeitenPhysical Examination FormDawit KumsaNoch keine Bewertungen
- Prevenção Secundária Avc Isquêmico - Guideline 2022Dokument41 SeitenPrevenção Secundária Avc Isquêmico - Guideline 2022Felipe Stoquetti de AbreuNoch keine Bewertungen
- Digital Covid Questionnaire For Revival Approval FormatDokument2 SeitenDigital Covid Questionnaire For Revival Approval Formatsouravdey3Noch keine Bewertungen
- Cleansing and DetoxificationDokument1 SeiteCleansing and DetoxificationerosNoch keine Bewertungen