Das könnte Ihnen auch gefallen
- Operation Ugly Truth Nurse Firsthand account of the NYC Pandemic 2020Von EverandOperation Ugly Truth Nurse Firsthand account of the NYC Pandemic 2020Noch keine Bewertungen
- Internal Medicine HISTORYDokument4 SeitenInternal Medicine HISTORYClaire FNoch keine Bewertungen
- Vomiting:: Internal Medicine HISTORY I. Patient'S Profile A. GENERAL DATA (Time: - )Dokument4 SeitenVomiting:: Internal Medicine HISTORY I. Patient'S Profile A. GENERAL DATA (Time: - )Peter GirasolNoch keine Bewertungen
- Neuropreceptorial ChecklistDokument33 SeitenNeuropreceptorial ChecklistAlloiBialba0% (1)
- History TakingDokument6 SeitenHistory Takingdharti daveNoch keine Bewertungen
- MayelinBenedictoRodriguez ClientForms 042922Dokument5 SeitenMayelinBenedictoRodriguez ClientForms 042922Cosmo Salón & SpaNoch keine Bewertungen
- Pediatric History OutlineDokument12 SeitenPediatric History OutlineDawn MarcoNoch keine Bewertungen
- PatienthistoryformenglishDokument4 SeitenPatienthistoryformenglishRuriko IkusawaNoch keine Bewertungen
- Pediatric AssessmentDokument6 SeitenPediatric AssessmentChu BagunuNoch keine Bewertungen
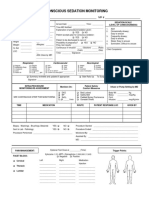
- 34 An Consious Sedation MonitoringDokument2 Seiten34 An Consious Sedation Monitoringabu alauon abed almohsenNoch keine Bewertungen
- Health Screening and Assessment Form - SampleDokument3 SeitenHealth Screening and Assessment Form - SampleRhu1 San Ildefonso100% (1)
- Pediatric History Taking Chart PDFDokument2 SeitenPediatric History Taking Chart PDFHerlene Lyneth ZalamedaNoch keine Bewertungen
- Assessment Tool On Neurological System: Baseline DataDokument21 SeitenAssessment Tool On Neurological System: Baseline DataK HepsibaNoch keine Bewertungen
- Live @,upbringing, Schooling, Marriage: When:, S/O:, Home SituationsDokument5 SeitenLive @,upbringing, Schooling, Marriage: When:, S/O:, Home SituationsJoy SalvadorNoch keine Bewertungen
- Annex A1: Print Legibly. Mark Appropriate Boxes C With " "Dokument21 SeitenAnnex A1: Print Legibly. Mark Appropriate Boxes C With " "allen zacariasNoch keine Bewertungen
- Health Survey FormDokument3 SeitenHealth Survey FormJazel SanchezNoch keine Bewertungen
- Paediatrics History + Examination Format-2Dokument4 SeitenPaediatrics History + Examination Format-2Salim KhaleelNoch keine Bewertungen
- Commed Template Family Report 2 1Dokument18 SeitenCommed Template Family Report 2 1Ge NavNoch keine Bewertungen
- OB Patho Assessment Tool EditedDokument6 SeitenOB Patho Assessment Tool EditedDarren RobertoNoch keine Bewertungen
- CRT 7Dokument8 SeitenCRT 7api-643868511Noch keine Bewertungen
- Annex A1: Print Legibly. Mark Appropriate Boxes C With " "Dokument6 SeitenAnnex A1: Print Legibly. Mark Appropriate Boxes C With " "Chum ChitaruNoch keine Bewertungen
- Form "D" Report of Practical Experience: Nursing Clinical Practice IDokument29 SeitenForm "D" Report of Practical Experience: Nursing Clinical Practice IAnderson RebaNoch keine Bewertungen
- Ateneo Higher Education Health Services Office Ateneo de Naga University Ateneo Avenue, Bagumbayan Sur, Naga CityDokument2 SeitenAteneo Higher Education Health Services Office Ateneo de Naga University Ateneo Avenue, Bagumbayan Sur, Naga CityKatherine VerceluzNoch keine Bewertungen
- Pediatric Assessment 1 12 PDFDokument11 SeitenPediatric Assessment 1 12 PDFJackieNate Ortiz100% (1)
- NCM 107 Rle: Indication of Use) : Name, Dose, Timing, Route Indication ObjectiveDokument5 SeitenNCM 107 Rle: Indication of Use) : Name, Dose, Timing, Route Indication ObjectiveDud AccNoch keine Bewertungen
- Health Examination RecordDokument4 SeitenHealth Examination Recordmary joy dela cruzNoch keine Bewertungen
- Gordons Functional Health Pattern Assessment Tool (Bano, R.)Dokument3 SeitenGordons Functional Health Pattern Assessment Tool (Bano, R.)ojay880% (1)
- Health History FormDokument1 SeiteHealth History Formapi-353679123Noch keine Bewertungen
- 11th REVISION HEALTH DECLARATION FORM 11 OCT 2020Dokument1 Seite11th REVISION HEALTH DECLARATION FORM 11 OCT 2020TIMMY BOYNoch keine Bewertungen
- Saint Louis University School of Medicine Department of Medicine General Data: Past Medical HistoryDokument3 SeitenSaint Louis University School of Medicine Department of Medicine General Data: Past Medical HistoryMarieCrisNoch keine Bewertungen
- Procedural Sedation RecordDokument2 SeitenProcedural Sedation RecordRosanne AguilarNoch keine Bewertungen
- GordonsDokument2 SeitenGordonsAngelica OctotNoch keine Bewertungen
- Tangalan Rural Health Unit Birthing Facility: Philippine Health Insurance CorporationDokument3 SeitenTangalan Rural Health Unit Birthing Facility: Philippine Health Insurance CorporationbenNoch keine Bewertungen
- P.A. Tool (Case Pres FINAL.)Dokument23 SeitenP.A. Tool (Case Pres FINAL.)Crystal Ann TadiamonNoch keine Bewertungen
- Hasil Pemeriksaan Kesehatan: I. General Data / Data PribadiDokument3 SeitenHasil Pemeriksaan Kesehatan: I. General Data / Data PribadiAoeliaZulkarneinNoch keine Bewertungen
- Cagayan de Oro City College of Nursing Assessment FormDokument12 SeitenCagayan de Oro City College of Nursing Assessment Formsticdo_nursing2011Noch keine Bewertungen
- Gordon S Functional Health Pattern Assessment ToolDokument17 SeitenGordon S Functional Health Pattern Assessment Toolmiss RN96% (45)
- Rle Worksheet: Labor Room and Delivery RoomDokument15 SeitenRle Worksheet: Labor Room and Delivery RoomLalisaM Activity100% (1)
- Night BeforeDokument3 SeitenNight BeforeChris MoffettNoch keine Bewertungen
- New Patient Paperwork (FINAL DRAFT)Dokument4 SeitenNew Patient Paperwork (FINAL DRAFT)andrew_sokolNoch keine Bewertungen
- Sedation Record: Patient Selection Criteria DateDokument2 SeitenSedation Record: Patient Selection Criteria Datenona aryanNoch keine Bewertungen
- Patients Profile RegaladoDokument5 SeitenPatients Profile RegaladoAngelo ArabejoNoch keine Bewertungen
- Student Health Record Form - FrontDokument1 SeiteStudent Health Record Form - FrontESPOS JEMS MYKELNoch keine Bewertungen
- FORMAT Pengkajian Bahasa InggrisDokument13 SeitenFORMAT Pengkajian Bahasa InggrisMadiinaaftNoch keine Bewertungen
- Apta Eval-Fax Version Asapt 2007Dokument4 SeitenApta Eval-Fax Version Asapt 2007Abdur RasyidNoch keine Bewertungen
- Nursing/Nursing Forms/Gordon's 11 Functional Health Patterns Aoih0718Dokument14 SeitenNursing/Nursing Forms/Gordon's 11 Functional Health Patterns Aoih0718jelaNoch keine Bewertungen
- Prenatal Nutrition and Immunization: Demographics OB HistoryDokument19 SeitenPrenatal Nutrition and Immunization: Demographics OB HistorynivraeNoch keine Bewertungen
- MRI WorksheetDokument2 SeitenMRI WorksheetDilini WijesinghNoch keine Bewertungen
- AUC Health ClearanceDokument2 SeitenAUC Health ClearanceNatasha ReddyNoch keine Bewertungen
- New P.E FormDokument5 SeitenNew P.E FormSt. John ClinicNoch keine Bewertungen
- Appendix 2: Evaluation Form For The Acquired Monocular Vision PatientDokument2 SeitenAppendix 2: Evaluation Form For The Acquired Monocular Vision PatientEvelyn SepulvedaNoch keine Bewertungen
- Gordon S Functional Health Pattern Assessment TooL: EdisonDokument13 SeitenGordon S Functional Health Pattern Assessment TooL: EdisonEdison Olad Dangkeo, RN,RM67% (3)
- WARDWORK TemplateDokument9 SeitenWARDWORK TemplateColeen NeyraNoch keine Bewertungen
- Governmental Traumatizing Investigations: An Application to Get a New Toilet, Part IVon EverandGovernmental Traumatizing Investigations: An Application to Get a New Toilet, Part INoch keine Bewertungen
- Pain: From Suffering to Feeling BetterVon EverandPain: From Suffering to Feeling BetterBewertung: 5 von 5 Sternen5/5 (1)
- A Pain Doctor’S Dilemma: Prescribing Opioids in an Era of OverdoseVon EverandA Pain Doctor’S Dilemma: Prescribing Opioids in an Era of OverdoseNoch keine Bewertungen
- ALLOW ME TO ADVOCATE FOR YOU ON YOUR NEXT DOCTORS APPOINTMENT.: Health QuestionsVon EverandALLOW ME TO ADVOCATE FOR YOU ON YOUR NEXT DOCTORS APPOINTMENT.: Health QuestionsNoch keine Bewertungen
- j.1 Emergencies 072012Dokument32 Seitenj.1 Emergencies 072012Norjetalexis CabreraNoch keine Bewertungen
- The Neurologic Examination-PDOUT-MHAMCMDokument31 SeitenThe Neurologic Examination-PDOUT-MHAMCMNorjetalexis CabreraNoch keine Bewertungen
- Drug ComputationDokument1 SeiteDrug ComputationNorjetalexis CabreraNoch keine Bewertungen
- Etiology Demographic S Clinical Manifestation S Disease Progressio N Pathophysiolog y Microscopic Appearanc e PrognosisDokument1 SeiteEtiology Demographic S Clinical Manifestation S Disease Progressio N Pathophysiolog y Microscopic Appearanc e PrognosisNorjetalexis CabreraNoch keine Bewertungen
- Compilation AnesthesiaDokument5 SeitenCompilation AnesthesiaNorjetalexis CabreraNoch keine Bewertungen
- Lonza BenchGuides Protocol For Performing A Trypan Blue Viability Test Technical Reference Guide PDFDokument2 SeitenLonza BenchGuides Protocol For Performing A Trypan Blue Viability Test Technical Reference Guide PDFNorjetalexis CabreraNoch keine Bewertungen
- HodgkinDokument2 SeitenHodgkinNorjetalexis CabreraNoch keine Bewertungen
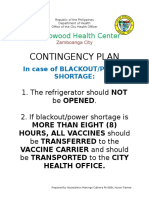
- Contingency Plan: Zambowood Health CenterDokument1 SeiteContingency Plan: Zambowood Health CenterNorjetalexis CabreraNoch keine Bewertungen
- 3.2 Peritoneal Cavity and The Esophagus (Banez)Dokument4 Seiten3.2 Peritoneal Cavity and The Esophagus (Banez)Norjetalexis CabreraNoch keine Bewertungen
- Drug ComputationDokument1 SeiteDrug ComputationNorjetalexis CabreraNoch keine Bewertungen
- Hersey Modern Violin MethodDokument53 SeitenHersey Modern Violin Methodovidiu4u2003100% (2)
- 3.1 Anterior Abdominal Wall (Bea)Dokument5 Seiten3.1 Anterior Abdominal Wall (Bea)Norjetalexis CabreraNoch keine Bewertungen
- Beriot Method Part 1Dokument78 SeitenBeriot Method Part 1Norjetalexis CabreraNoch keine Bewertungen
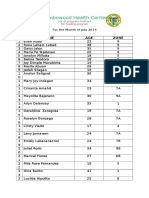
- Zambowood Health Center: Name AGE ZoneDokument2 SeitenZambowood Health Center: Name AGE ZoneNorjetalexis CabreraNoch keine Bewertungen
- Parasitology Slide Presentation SET BDokument28 SeitenParasitology Slide Presentation SET BNorjetalexis CabreraNoch keine Bewertungen
- Morning Report 5-7 JanDokument18 SeitenMorning Report 5-7 JanBudiNoch keine Bewertungen
- Desain GordingDokument17 SeitenDesain GordingIrfan Gơlden BơyNoch keine Bewertungen
- Cardiorespiratory Assessment ChartDokument3 SeitenCardiorespiratory Assessment Chartphysiovipin100% (3)
- Kuis Emesis 4-MergedDokument16 SeitenKuis Emesis 4-Mergedibnu an nafisNoch keine Bewertungen
- Chronic-Cholecystitis-and-Metastatic-Breast-CA FinalDokument3 SeitenChronic-Cholecystitis-and-Metastatic-Breast-CA FinalRishi Du AgbugayNoch keine Bewertungen
- Adverse Events Associated With Therapeutic Dry NeedlingDokument11 SeitenAdverse Events Associated With Therapeutic Dry NeedlingPatricia MashabaNoch keine Bewertungen
- Cholecystectomy Nursing Care Plan: Intraoperative Problem: Risk For AspirationDokument1 SeiteCholecystectomy Nursing Care Plan: Intraoperative Problem: Risk For AspirationJess GoNoch keine Bewertungen
- BASH Guidelines 2007Dokument52 SeitenBASH Guidelines 2007markspencerwhitingNoch keine Bewertungen
- Epidural Information CardDokument2 SeitenEpidural Information Cardheba abuhelwaNoch keine Bewertungen
- Causes of Abdominal Pain in AdultsDokument41 SeitenCauses of Abdominal Pain in AdultsAmjaSaud100% (1)
- Schizophrenia Case Study File For ProjectDokument20 SeitenSchizophrenia Case Study File For ProjectNiharika SharmaNoch keine Bewertungen
- Sign & Symptoms: Disusun Oleh: Izri Miftahul AudryDokument12 SeitenSign & Symptoms: Disusun Oleh: Izri Miftahul AudryIzri Miftahul AudryNoch keine Bewertungen
- NR 17 - Excessive Fatigue Symptom InventoryDokument2 SeitenNR 17 - Excessive Fatigue Symptom InventoryCPSSTNoch keine Bewertungen
- The Therapeutics of Acupuncture and Moxibustion (Otitis Media, Tinnitusdeafness, Toothache, Sore Throat)Dokument22 SeitenThe Therapeutics of Acupuncture and Moxibustion (Otitis Media, Tinnitusdeafness, Toothache, Sore Throat)clerise3Noch keine Bewertungen
- Connexus SigcodesDokument8 SeitenConnexus SigcodesAhmed Mashaly100% (1)
- Chest Pain - Investigation, Diagnosis and TreatmentDokument5 SeitenChest Pain - Investigation, Diagnosis and Treatmentsoumabho paruiNoch keine Bewertungen
- Allen S Clinical Hints (Seror)Dokument479 SeitenAllen S Clinical Hints (Seror)aldodiasNoch keine Bewertungen
- Mnemonic CsDokument9 SeitenMnemonic CsJavier PresserNoch keine Bewertungen
- Abdominal PainDokument12 SeitenAbdominal PainGeeza Gem VicencioNoch keine Bewertungen
- CMCSS Return To Work/School FlowchartDokument1 SeiteCMCSS Return To Work/School FlowchartFOX 17 NewsNoch keine Bewertungen
- Establish of Vetigo. The Practitioner September 2010 - 254 (1732) : 19-23. 2010Dokument2 SeitenEstablish of Vetigo. The Practitioner September 2010 - 254 (1732) : 19-23. 2010Langlang BawonoNoch keine Bewertungen
- Acute Exacerbation Bronchial AsthmaDokument21 SeitenAcute Exacerbation Bronchial AsthmaChekNatrahNoch keine Bewertungen
- IBS ResearchDokument5 SeitenIBS ResearchDrHassan Ahmed ShaikhNoch keine Bewertungen
- PE and Health 12 - Module 5Dokument19 SeitenPE and Health 12 - Module 5Stephen Lorenzo A. Doria100% (2)
- 2A - Zahirah Rahmadian Budiman - PROBLEMS WITH PAINDokument5 Seiten2A - Zahirah Rahmadian Budiman - PROBLEMS WITH PAINZahirah BudimanNoch keine Bewertungen
- Migraine - Symptoms, Causes, Treatment, Triggers, and MoreDokument35 SeitenMigraine - Symptoms, Causes, Treatment, Triggers, and MoreKarlla SuarezNoch keine Bewertungen
- Medical History TakingDokument9 SeitenMedical History Takingbadreanimator100% (2)
- Skoring Osas AmirahDokument11 SeitenSkoring Osas AmirahthtklNoch keine Bewertungen
- Vocabulary Unit 3Dokument4 SeitenVocabulary Unit 3MARI CARMEN SANCHEZ RUBIONoch keine Bewertungen
- Análisis Clínico y Radiográfico de Las Técnicas ART y Remoción Químico-Mecánica de Caries - Estudio PilotoDokument7 SeitenAnálisis Clínico y Radiográfico de Las Técnicas ART y Remoción Químico-Mecánica de Caries - Estudio PilotoValeria RodriguezNoch keine Bewertungen