Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- AS Unit 1 Revision Note Physics IAL EdexcelDokument9 SeitenAS Unit 1 Revision Note Physics IAL EdexcelMahbub Khan100% (1)
- List - of - Members As On 6 3 18 PDFDokument8 SeitenList - of - Members As On 6 3 18 PDFashish jaiswal100% (1)
- Fig. 6.14 Circular WaveguideDokument16 SeitenFig. 6.14 Circular WaveguideThiagu RajivNoch keine Bewertungen
- OsteomyelitisDokument10 SeitenOsteomyelitismustafaNoch keine Bewertungen
- A Freudian Look Into Roger Waters' True Expressions in "The Wall."Dokument5 SeitenA Freudian Look Into Roger Waters' True Expressions in "The Wall."Jacob Ritteman100% (1)
- HTTP WWW - Aphref.aph - Gov.au House Committee Haa Overseasdoctors Subs Sub133Dokument3 SeitenHTTP WWW - Aphref.aph - Gov.au House Committee Haa Overseasdoctors Subs Sub133hadia duraniNoch keine Bewertungen
- Agricultural LocationDokument26 SeitenAgricultural LocationPrince MpofuNoch keine Bewertungen
- 2019 - List of Equipment, Tools & MaterialsDokument3 Seiten2019 - List of Equipment, Tools & Materialsreynald manzanoNoch keine Bewertungen
- A Plan of Life - Scepter BookletDokument10 SeitenA Plan of Life - Scepter Bookletpeteatkinson@gmail.comNoch keine Bewertungen
- PolygonsDokument23 SeitenPolygonsPietrelle Liana PuruggananNoch keine Bewertungen
- Mobile DevGuide 13 - Gulde For Mobile DeveloperDokument258 SeitenMobile DevGuide 13 - Gulde For Mobile DevelopersmaliscribdNoch keine Bewertungen
- Estudio - Women Who Suffered Emotionally From Abortion - A Qualitative Synthesis of Their ExperiencesDokument6 SeitenEstudio - Women Who Suffered Emotionally From Abortion - A Qualitative Synthesis of Their ExperiencesSharmely CárdenasNoch keine Bewertungen
- PHMSA Amended Corrective Action Order For Plains All American Pipeline Regarding Refugio Oil Spill in Santa Barbara CountyDokument7 SeitenPHMSA Amended Corrective Action Order For Plains All American Pipeline Regarding Refugio Oil Spill in Santa Barbara Countygiana_magnoliNoch keine Bewertungen
- Hermle C42 ENDokument72 SeitenHermle C42 ENKiril AngelovNoch keine Bewertungen
- Italian Companies Eastern China - JAN 2014Dokument139 SeitenItalian Companies Eastern China - JAN 2014AndresNoch keine Bewertungen
- MMDA v. Viron Transportation CoDokument3 SeitenMMDA v. Viron Transportation CoTtlrpqNoch keine Bewertungen
- Flore Bridoux CV Sep 2016 Short VersionDokument10 SeitenFlore Bridoux CV Sep 2016 Short Versionbayu_pancaNoch keine Bewertungen
- 9701 w19 QP 21 PDFDokument12 Seiten9701 w19 QP 21 PDFFaiza KhalidNoch keine Bewertungen
- El Poder de La Disciplina El Hábito Que Cambiará Tu Vida (Raimon Samsó)Dokument4 SeitenEl Poder de La Disciplina El Hábito Que Cambiará Tu Vida (Raimon Samsó)ER CaballeroNoch keine Bewertungen
- Guide Item Dota 2Dokument11 SeitenGuide Item Dota 2YogaWijayaNoch keine Bewertungen
- Tribebook Wendigo Revised Edition 6244638Dokument109 SeitenTribebook Wendigo Revised Edition 6244638PedroNoch keine Bewertungen
- d301244x012 PDFDokument330 Seitend301244x012 PDFFIRMANSYAH100% (1)
- Soal Dan Pembahasan Grammar Lat TOEP 1Dokument6 SeitenSoal Dan Pembahasan Grammar Lat TOEP 1Abdur100% (2)
- AIPT 2021 GuidelineDokument4 SeitenAIPT 2021 GuidelineThsavi WijayasingheNoch keine Bewertungen
- TV Studio ChainDokument38 SeitenTV Studio ChainKalpesh Katara100% (1)
- Medical and Health Care DocumentDokument6 SeitenMedical and Health Care Document786waqar786Noch keine Bewertungen
- Edu602 Ubd TemplateDokument2 SeitenEdu602 Ubd Templateapi-481192424Noch keine Bewertungen
- Feature Fusion Based On Convolutional Neural Netwo PDFDokument8 SeitenFeature Fusion Based On Convolutional Neural Netwo PDFNguyễn Thành TânNoch keine Bewertungen
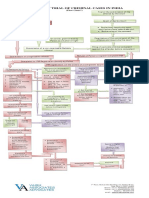
- Process of Trial of Criminal Cases in India (Flow Chart)Dokument1 SeiteProcess of Trial of Criminal Cases in India (Flow Chart)Arun Hiro100% (1)
- 6.marketing ManagementDokument11 Seiten6.marketing ManagementadararaNoch keine Bewertungen