Das könnte Ihnen auch gefallen
- Fenotipos Sepsis 5 PDFDokument16 SeitenFenotipos Sepsis 5 PDFGerardo LermaNoch keine Bewertungen
- Treatment Implications of Novel Clinical Phenotypes For Sepsis PDFDokument2 SeitenTreatment Implications of Novel Clinical Phenotypes For Sepsis PDFGerardo LermaNoch keine Bewertungen
- Fenotipos Sepsis 3Dokument5 SeitenFenotipos Sepsis 3Gerardo LermaNoch keine Bewertungen
- Gibson 2018Dokument10 SeitenGibson 2018Gerardo LermaNoch keine Bewertungen
- s13054 019 2655 7 PDFDokument9 Seitens13054 019 2655 7 PDFjenaro heli Ardila CortesNoch keine Bewertungen
- Sepsis and ShockDokument13 SeitenSepsis and ShockUther Pendragon100% (2)
- Fenotipos Sepsis 1 PDFDokument2 SeitenFenotipos Sepsis 1 PDFGerardo LermaNoch keine Bewertungen
- 10 1001@jama 2019Dokument15 Seiten10 1001@jama 2019Liliam GonzalezNoch keine Bewertungen
- Fenotipos Sepsis 3Dokument5 SeitenFenotipos Sepsis 3Gerardo LermaNoch keine Bewertungen
- AOAStudy 2018Dokument26 SeitenAOAStudy 2018Gerardo Lerma100% (1)
- Acute Respiratory Distress Syndrome NEJM 2018Dokument11 SeitenAcute Respiratory Distress Syndrome NEJM 2018darlingcarvajalduqueNoch keine Bewertungen
- Anxiety LancetDokument12 SeitenAnxiety LancetAnonymous B9zv0Y100% (1)
- 13958054684195Dokument13 Seiten13958054684195Chairul Nurdin AzaliNoch keine Bewertungen
- ARDSnet Ventilation Protocol SummaryDokument2 SeitenARDSnet Ventilation Protocol SummaryvbfisioNoch keine Bewertungen
- Enfermedades de Transmision SexualDokument45 SeitenEnfermedades de Transmision SexualGerardo LermaNoch keine Bewertungen
- Pas PDFDokument8 SeitenPas PDFRoxi_137Noch keine Bewertungen
- Artritis ReumatoideDokument9 SeitenArtritis ReumatoideGerardo Lerma BurciagaNoch keine Bewertungen
- Trombotic MicroangyopathyDokument13 SeitenTrombotic MicroangyopathyGerardo LermaNoch keine Bewertungen
- Study Guide PlannerDokument6 SeitenStudy Guide PlannerGerardo LermaNoch keine Bewertungen
- ABIM DetalladoDokument52 SeitenABIM DetalladoGerardo LermaNoch keine Bewertungen
- Abim Certificacion Examination BlueprintDokument28 SeitenAbim Certificacion Examination BlueprintGerardo LermaNoch keine Bewertungen
- Picmonic Step 1 Study Guide 2016Dokument32 SeitenPicmonic Step 1 Study Guide 2016bisharat50% (2)
- FIGO Clasificación HUA 2011Dokument11 SeitenFIGO Clasificación HUA 2011dickenskevinNoch keine Bewertungen
- UnderstandingPathophysiology2E 9780729541602 CraftGordon Samplechapter Web PDFDokument38 SeitenUnderstandingPathophysiology2E 9780729541602 CraftGordon Samplechapter Web PDFGerardo Lerma0% (4)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- HL Topic 11.4 ReproductionDokument6 SeitenHL Topic 11.4 ReproductionAnonymous iIj7YGNoch keine Bewertungen
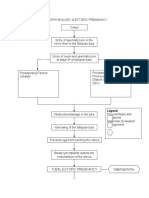
- PATHOPHYSIOLOGY of ECTOPIC PREGNANCYDokument2 SeitenPATHOPHYSIOLOGY of ECTOPIC PREGNANCYrye100% (1)
- The Occult Forces of Sexual UnionDokument6 SeitenThe Occult Forces of Sexual Unionimmortality2045_841960% (5)
- Plant Propagation Lab ActivityDokument2 SeitenPlant Propagation Lab ActivityClint Jhun TabugocNoch keine Bewertungen
- Characteristics of Living Things Guided NotesDokument3 SeitenCharacteristics of Living Things Guided NotesErica HartNoch keine Bewertungen
- NCERT Biology Reproductive Health FactsDokument5 SeitenNCERT Biology Reproductive Health FactsNishtha Jain100% (1)
- Assessing Male Genitalia and InguinalDokument51 SeitenAssessing Male Genitalia and InguinalJellaiza QuiozonNoch keine Bewertungen
- Introduction To Life ScienceDokument24 SeitenIntroduction To Life ScienceCharlize Marie Dula-ogonNoch keine Bewertungen
- R1 Symptoms and Diagnosis of PregnancyDokument49 SeitenR1 Symptoms and Diagnosis of PregnancyMoges desaleNoch keine Bewertungen
- Sexual Reproduction in Flowering Plants QuestionsDokument11 SeitenSexual Reproduction in Flowering Plants QuestionsAjayNoch keine Bewertungen
- 9700 m16 QP 42 PDFDokument28 Seiten9700 m16 QP 42 PDFAtef Ibrahim KhalifaNoch keine Bewertungen
- Veterinaria Medika Vol 7, No. 2, Juli 2014Dokument8 SeitenVeterinaria Medika Vol 7, No. 2, Juli 2014Ergha TriadyNoch keine Bewertungen
- Floral Formula: BotanyDokument7 SeitenFloral Formula: BotanyzedoksNoch keine Bewertungen
- 57-1-1 BiologyDokument15 Seiten57-1-1 BiologyRavneet KaurNoch keine Bewertungen
- BIO 3:plant ClassificationDokument5 SeitenBIO 3:plant ClassificationTers MedinaNoch keine Bewertungen
- Reproductive Character of The Ricefield EelDokument14 SeitenReproductive Character of The Ricefield EelnesaNoch keine Bewertungen
- Mode of ReproductionDokument33 SeitenMode of ReproductionMd. Rayhan Ali RejviNoch keine Bewertungen
- National Public School: SUBJECT-Science (10 (Pre Board Examination)Dokument2 SeitenNational Public School: SUBJECT-Science (10 (Pre Board Examination)amit kumarNoch keine Bewertungen
- J5-6 Lesson 10 - Meiosis StudentDokument3 SeitenJ5-6 Lesson 10 - Meiosis Studentkristhel ann caringal reyes0% (1)
- Week 5 Worksheet AnswersDokument5 SeitenWeek 5 Worksheet AnswersaskldhfdasjkNoch keine Bewertungen
- Question Paper Unit A161 02 Modules b1 b2 b3 Higher TierDokument16 SeitenQuestion Paper Unit A161 02 Modules b1 b2 b3 Higher TierAnonymous QFkCS837bNoch keine Bewertungen
- Teaching and Learning Module KSSR (Semakan 2017) Science Year 6Dokument116 SeitenTeaching and Learning Module KSSR (Semakan 2017) Science Year 6LING KUOK LIMNoch keine Bewertungen
- 1-Embryonic-Stem-Cells 1ST LECDokument31 Seiten1-Embryonic-Stem-Cells 1ST LECrihamazim2018Noch keine Bewertungen
- Bio 10th - How Do Organism Reproduce - Revision WorksheetDokument10 SeitenBio 10th - How Do Organism Reproduce - Revision WorksheetDharmendra SinghNoch keine Bewertungen
- A Quick Overview of Genetic Engineering and EctoDokument1 SeiteA Quick Overview of Genetic Engineering and EctoHannah Grace AquinoNoch keine Bewertungen
- Contoh PDFDokument12 SeitenContoh PDFGratiano TelaumbanuaNoch keine Bewertungen
- Lesson Plan For Final DemoDokument9 SeitenLesson Plan For Final DemoJunjun Caoli50% (2)
- Hydatidiform MoleDokument2 SeitenHydatidiform MoleIrfan HardiNoch keine Bewertungen
- Revision Notes Class 8 Science Chapter 10 - Reaching The Age of AdolescenceDokument2 SeitenRevision Notes Class 8 Science Chapter 10 - Reaching The Age of AdolescenceArpit SharmaNoch keine Bewertungen
- Pregnancy - Anatomy and PhysiologyDokument5 SeitenPregnancy - Anatomy and PhysiologyNiSCHENoch keine Bewertungen