Das könnte Ihnen auch gefallen
- Polyvinylsulfonic Acid A Low Cost RNase Inhibitor For Enhanced RNA Preservation and Cell Free Protein TranslationDokument9 SeitenPolyvinylsulfonic Acid A Low Cost RNase Inhibitor For Enhanced RNA Preservation and Cell Free Protein Translationalessandro8265Noch keine Bewertungen
- G Tran Series Pirani Gauge Box UnitDokument2 SeitenG Tran Series Pirani Gauge Box Unitalessandro8265Noch keine Bewertungen
- How To Properly Clean Laboratory GlasswareDokument3 SeitenHow To Properly Clean Laboratory Glasswarealessandro8265Noch keine Bewertungen
- PatentDokument17 SeitenPatentalessandro8265Noch keine Bewertungen
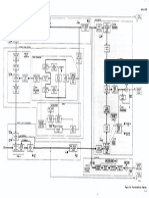
- HP 8405A Schematic Diagrams04Dokument1 SeiteHP 8405A Schematic Diagrams04alessandro8265Noch keine Bewertungen
- Instruction Manual: MillivoltmeterDokument51 SeitenInstruction Manual: Millivoltmeteralessandro8265100% (1)
- Building A Thermocouple Vacuum GaugeDokument8 SeitenBuilding A Thermocouple Vacuum Gaugealessandro8265Noch keine Bewertungen
- Experiment SetupDokument7 SeitenExperiment Setupalessandro8265Noch keine Bewertungen
- Pirani GaugeDokument4 SeitenPirani Gaugealessandro8265Noch keine Bewertungen
- Tektronix 475 Service ManualDokument222 SeitenTektronix 475 Service Manualkenkostan100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Nutrition in PlantsDokument33 SeitenNutrition in PlantsIqra HanifNoch keine Bewertungen
- Types of Nucleic Acids: Return To TOC 1Dokument95 SeitenTypes of Nucleic Acids: Return To TOC 1Hey itsJamNoch keine Bewertungen
- A Comparative Study of Various Oil ExtraDokument23 SeitenA Comparative Study of Various Oil ExtraAjay PurohitNoch keine Bewertungen
- Dake Chu: Cui WeiDokument61 SeitenDake Chu: Cui WeiDave UlanNoch keine Bewertungen
- Chemistry of Amino AcidDokument15 SeitenChemistry of Amino AcidWay FarerNoch keine Bewertungen
- Best Linear Unbiased Prediction of Genomic Breeding PDFDokument8 SeitenBest Linear Unbiased Prediction of Genomic Breeding PDFEdjane FreitasNoch keine Bewertungen
- PVP Form 1-Application FormDokument7 SeitenPVP Form 1-Application FormJoeluntalanNoch keine Bewertungen
- 0001DC012834 1 Yf1Dokument2 Seiten0001DC012834 1 Yf1Arun KumarNoch keine Bewertungen
- Erotic MassageDokument2 SeitenErotic MassageKarugu MartinNoch keine Bewertungen
- Progress in PD-1 - PD-L1 Pathway Inhibitors - From Biomacromolecules To Small MoleculesDokument30 SeitenProgress in PD-1 - PD-L1 Pathway Inhibitors - From Biomacromolecules To Small MoleculesMario Andres JuradoNoch keine Bewertungen
- Medical Biotechnology: A Resource Guide For Biotechnology Club SponsorsDokument39 SeitenMedical Biotechnology: A Resource Guide For Biotechnology Club Sponsorsim_mogerzNoch keine Bewertungen
- The Storage of Tropical Agricultural Products: Agrodok 31Dokument84 SeitenThe Storage of Tropical Agricultural Products: Agrodok 31Seyha L. AgriFoodNoch keine Bewertungen
- Form InspeksiDokument8 SeitenForm Inspeksiichsan syahputraNoch keine Bewertungen
- Treatment Knowledge Ramadhan SeriesDokument2 SeitenTreatment Knowledge Ramadhan SeriesAbrisha Agung WicaksonoNoch keine Bewertungen
- Douglas I. Johnson (Auth.) - Bacterial Pathogens and Their Virulence Factors (2018, Springer International Publishing)Dokument451 SeitenDouglas I. Johnson (Auth.) - Bacterial Pathogens and Their Virulence Factors (2018, Springer International Publishing)Alvaro EstupiñánNoch keine Bewertungen
- Behold The Mighty DinosaurDokument65 SeitenBehold The Mighty DinosaurLuis Fernandez100% (3)
- Warm Blooded Animals & ThermoregulationDokument33 SeitenWarm Blooded Animals & Thermoregulationlock stock and barrelNoch keine Bewertungen
- History of HLA PDFDokument17 SeitenHistory of HLA PDFeseNoch keine Bewertungen
- Jurnal KedokteranDokument6 SeitenJurnal Kedokteranusk.ppdsobgynganjil2022Noch keine Bewertungen
- Green Pesticides For Organic Farming Occurrence and Properties of Essential Oils For Use in Pest ControlDokument25 SeitenGreen Pesticides For Organic Farming Occurrence and Properties of Essential Oils For Use in Pest ControlteguhwidiartoNoch keine Bewertungen
- Cow/Calf Record Book: YearDokument64 SeitenCow/Calf Record Book: YearNikson Rafael AmosNoch keine Bewertungen
- Illustrated Pocket Dictionary of Chromatography PDFDokument222 SeitenIllustrated Pocket Dictionary of Chromatography PDFVohinh NgoNoch keine Bewertungen
- 1.1 and 1.3 NotesDokument3 Seiten1.1 and 1.3 NotesKalie ChanNoch keine Bewertungen
- RGKSU 1st Proff 10 YearsDokument115 SeitenRGKSU 1st Proff 10 YearsAranya BhandaryNoch keine Bewertungen
- Brock Biology of MicrooDokument6 SeitenBrock Biology of MicrooÇağla Koca100% (1)
- Sponge Bob Genetics PracticeDokument3 SeitenSponge Bob Genetics Practiceapi-293001217Noch keine Bewertungen
- Seminar 23 Feb 2013 Grand Zuri - ANTI AGING - Dr. Dr. Amarullah H. Siregar, PHDDokument49 SeitenSeminar 23 Feb 2013 Grand Zuri - ANTI AGING - Dr. Dr. Amarullah H. Siregar, PHDUmmuNoch keine Bewertungen
- Botany (Week 1-5) Merged PDFDokument287 SeitenBotany (Week 1-5) Merged PDFLisa MuthiniNoch keine Bewertungen
- Toxicity Research Paper On AntsDokument8 SeitenToxicity Research Paper On AntsMazhar FarNoch keine Bewertungen
- Synthetic Cannabinoid Receptor Agonists and Death Cases A Literature ReviewDokument14 SeitenSynthetic Cannabinoid Receptor Agonists and Death Cases A Literature ReviewTJPRC PublicationsNoch keine Bewertungen