Das könnte Ihnen auch gefallen
- Adult Advanced Life Support Algorithm 2021 Aug 2023Dokument1 SeiteAdult Advanced Life Support Algorithm 2021 Aug 2023cknihilnewNoch keine Bewertungen
- PalsDokument1 SeitePalslordroentgenNoch keine Bewertungen
- Adult advanced life support guidelinesDokument1 SeiteAdult advanced life support guidelineskhaledNoch keine Bewertungen
- Presenting Problems in Cardiovascular Disease - 457: Abnormal Heart SoundsDokument19 SeitenPresenting Problems in Cardiovascular Disease - 457: Abnormal Heart SoundsDarawan MirzaNoch keine Bewertungen
- Poster 10 PALS 01 01 ENG V20100927 PDFDokument1 SeitePoster 10 PALS 01 01 ENG V20100927 PDFAndy XiaoNoch keine Bewertungen
- ALS Cardiac Arrest GuideDokument1 SeiteALS Cardiac Arrest GuideLucian Alin DinuNoch keine Bewertungen
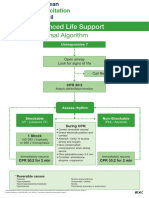
- Advanced Life Support - A0 PDFDokument1 SeiteAdvanced Life Support - A0 PDFiulia-uroNoch keine Bewertungen
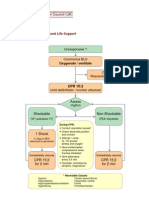
- Advanced Paediatric Life Support - A0 PDFDokument1 SeiteAdvanced Paediatric Life Support - A0 PDFiulia-uroNoch keine Bewertungen
- Advanced Life Support Algorithm: Learning OutcomesDokument8 SeitenAdvanced Life Support Algorithm: Learning OutcomesParvathy R NairNoch keine Bewertungen
- Cardiac Arrest Advanced Life SupportDokument1 SeiteCardiac Arrest Advanced Life SupportCristina TrofimovNoch keine Bewertungen
- Cardiac Arrest Advanced Life Support PDFDokument1 SeiteCardiac Arrest Advanced Life Support PDFCristina TrofimovNoch keine Bewertungen
- CPR for Asystole or PEADokument1 SeiteCPR for Asystole or PEAmayNoch keine Bewertungen
- Adult Advanced Life SupportDokument23 SeitenAdult Advanced Life SupportbigpriapNoch keine Bewertungen
- Paediatric ALS A3Dokument1 SeitePaediatric ALS A3Ali HusseinNoch keine Bewertungen
- Alsalgo PDFDokument1 SeiteAlsalgo PDFDelvanny Alfikri Rekaputri WicaksonoNoch keine Bewertungen
- AlsalgoDokument1 SeiteAlsalgozacklim_2000Noch keine Bewertungen
- PalsalgoDokument1 SeitePalsalgozacklim_2000Noch keine Bewertungen
- Advanced Life Support AlgorithmDokument34 SeitenAdvanced Life Support AlgorithmmariamNoch keine Bewertungen
- Reanimacion CardiopulmonarDokument15 SeitenReanimacion CardiopulmonarVictoriano ValienteNoch keine Bewertungen
- ACLS ReportDokument58 SeitenACLS ReportCamille Honeyleith FernandoNoch keine Bewertungen
- 44 CPR PDFDokument14 Seiten44 CPR PDFBramantyo NugrosNoch keine Bewertungen
- In Hospital AlgoDokument1 SeiteIn Hospital Algozacklim_2000Noch keine Bewertungen
- ACLSDokument275 SeitenACLSShajahan SideequeNoch keine Bewertungen
- Presentasi Code Blue IGDDokument16 SeitenPresentasi Code Blue IGDIgd Pondok TjandraNoch keine Bewertungen
- Cardiac Arrest Circular AlgorithmDokument2 SeitenCardiac Arrest Circular AlgorithmJunius SimarmataNoch keine Bewertungen
- Poster SpecCircs Traumatic Cardiac Arrest Algorithm ENG V20151005 HRES SiteDokument1 SeitePoster SpecCircs Traumatic Cardiac Arrest Algorithm ENG V20151005 HRES SiteangelologrilloNoch keine Bewertungen
- Immediate life supportDokument63 SeitenImmediate life supportmatrixkhalifa9955Noch keine Bewertungen
- ACLS 2015 Algorithm and Anesthesia ACLS PDFDokument14 SeitenACLS 2015 Algorithm and Anesthesia ACLS PDFTaufiqurrahman RizkiNoch keine Bewertungen
- Algo ArrestDokument2 SeitenAlgo ArrestLocomotorica FK UkiNoch keine Bewertungen
- Basic Emergency Life Support ProceduresDokument26 SeitenBasic Emergency Life Support Proceduresabee80Noch keine Bewertungen
- Advance Life Support MaterialDokument2 SeitenAdvance Life Support MaterialmayNoch keine Bewertungen
- (Pre-Hospital) Adult Basic Life Support: UnresponsiveDokument24 Seiten(Pre-Hospital) Adult Basic Life Support: Unresponsiveae3770945Noch keine Bewertungen
- RECOVER_CPR_ALGORITHMDokument1 SeiteRECOVER_CPR_ALGORITHMkt496Noch keine Bewertungen
- Pulseless Ventricular Tachycardia/Ventricular Fibrillation Algorithm (Figure 8-5)Dokument1 SeitePulseless Ventricular Tachycardia/Ventricular Fibrillation Algorithm (Figure 8-5)Dyan IslamiNoch keine Bewertungen
- Poster ALS Algorithm ENG V20151005 HRES SiteDokument1 SeitePoster ALS Algorithm ENG V20151005 HRES SiteCosmina Alina MoscuNoch keine Bewertungen
- The ACM v2.0 International PDFDokument76 SeitenThe ACM v2.0 International PDFTiago SilvaNoch keine Bewertungen
- Start CPR Shout For Help/Activate Emergency Response: Give Oxygen Attach Monitor/DefibrillatorDokument2 SeitenStart CPR Shout For Help/Activate Emergency Response: Give Oxygen Attach Monitor/DefibrillatorFelicia ErikaNoch keine Bewertungen
- Critical Care Skills Check ListDokument3 SeitenCritical Care Skills Check Listhemarani60605582Noch keine Bewertungen
- Bls & Acls & DC ShockDokument70 SeitenBls & Acls & DC Shockpop lopNoch keine Bewertungen
- Resusitasi Kardio PulmonerDokument34 SeitenResusitasi Kardio PulmonerpuskngaliyanNoch keine Bewertungen
- CPR 2015Dokument55 SeitenCPR 2015Alisya NadhilahNoch keine Bewertungen
- Pediatric Bradycardia With A Pulse and Poor Perfusion AlgorithmDokument1 SeitePediatric Bradycardia With A Pulse and Poor Perfusion AlgorithmRadhiatul MardhiahNoch keine Bewertungen
- Acute Coronary Syndromes Algorithm: Patient Has Signs Suggestive of Ischemia or InfarctionDokument1 SeiteAcute Coronary Syndromes Algorithm: Patient Has Signs Suggestive of Ischemia or Infarctionjohndoe1995Noch keine Bewertungen
- Resuscitation Council (UK)Dokument18 SeitenResuscitation Council (UK)Abdelfattah RashwanNoch keine Bewertungen
- Tatalaksana KegawatdaruratanDokument9 SeitenTatalaksana KegawatdaruratanBennyNoch keine Bewertungen
- CPR PosterDokument1 SeiteCPR PosterHemantNoch keine Bewertungen
- Adult Advanced Life Support: Birmingham Children's Hospital ED Handbook Version 1 (2011)Dokument2 SeitenAdult Advanced Life Support: Birmingham Children's Hospital ED Handbook Version 1 (2011)madimadi11Noch keine Bewertungen
- STAGES of AnesthesiaDokument4 SeitenSTAGES of AnesthesiaMabz Posadas BisnarNoch keine Bewertungen
- Dvanced Cardiac Life SupportDokument72 SeitenDvanced Cardiac Life Supportolivia100% (1)
- Advanced Life Support Algorithm: Learning OutcomesDokument12 SeitenAdvanced Life Support Algorithm: Learning OutcomesAljeirou AlcachupasNoch keine Bewertungen
- Emergency Care Algorithms 2018 PDFDokument77 SeitenEmergency Care Algorithms 2018 PDFFranklin Correa100% (2)
- Code Blue Simulation TrainingDokument26 SeitenCode Blue Simulation TrainingJenny CandraNoch keine Bewertungen
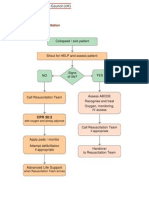
- G2015 in Hospital ResuscitationDokument1 SeiteG2015 in Hospital ResuscitationLily hestiNoch keine Bewertungen
- PALSposterDokument1 SeitePALSposterJose SesmeroNoch keine Bewertungen
- Modern Anaesthesia:: A Concise Guide to the Study and Practice of Anaesthesia.Von EverandModern Anaesthesia:: A Concise Guide to the Study and Practice of Anaesthesia.Noch keine Bewertungen
- Questions and Answers in Small Animal AnesthesiaVon EverandQuestions and Answers in Small Animal AnesthesiaLesley J. SmithNoch keine Bewertungen
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideVon EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuideNoch keine Bewertungen
- Monitoring Mechanical Ventilation Using Ventilator WaveformsVon EverandMonitoring Mechanical Ventilation Using Ventilator WaveformsNoch keine Bewertungen
- Advanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesVon EverandAdvanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesBewertung: 4 von 5 Sternen4/5 (6)
- American Journal of Emergency Medicine: SciencedirectDokument4 SeitenAmerican Journal of Emergency Medicine: SciencedirectRenzo Iván Marín DávalosNoch keine Bewertungen
- Emergency Medicine Resident Efficiency and Emergency Department CrowdingDokument9 SeitenEmergency Medicine Resident Efficiency and Emergency Department CrowdingRenzo Iván Marín DávalosNoch keine Bewertungen
- Medical and Undergraduate Student Perceptions On Scribing in An Emergency DepartmentDokument14 SeitenMedical and Undergraduate Student Perceptions On Scribing in An Emergency DepartmentRenzo Iván Marín DávalosNoch keine Bewertungen
- African Journal of Emergency MedicineDokument11 SeitenAfrican Journal of Emergency MedicineRenzo Iván Marín DávalosNoch keine Bewertungen
- Emergency Medicine Residents On Electronic Medical Records: Perspectives and AdviceDokument7 SeitenEmergency Medicine Residents On Electronic Medical Records: Perspectives and AdviceRenzo Iván Marín DávalosNoch keine Bewertungen
- African Journal of Emergency Medicine: CommentaryDokument7 SeitenAfrican Journal of Emergency Medicine: CommentaryRenzo Iván Marín DávalosNoch keine Bewertungen
- Assessing Medical Student Documentation Using Simulated Charts in Emergency MedicineDokument6 SeitenAssessing Medical Student Documentation Using Simulated Charts in Emergency MedicineRenzo Iván Marín DávalosNoch keine Bewertungen
- Survey of Continuing Education Needs For Nonemergency Physicians in Emergency MedicineDokument4 SeitenSurvey of Continuing Education Needs For Nonemergency Physicians in Emergency MedicineRenzo Iván Marín DávalosNoch keine Bewertungen
- 2019 Hypertensive Disorders of PregnancyDokument16 Seiten2019 Hypertensive Disorders of PregnancyMaria del Pilar Devis MoralesNoch keine Bewertungen
- Stroke 2019 Klavuzu1Dokument75 SeitenStroke 2019 Klavuzu1MuNoch keine Bewertungen
- 10 1016@j Jacc 2019 01 011Dokument52 Seiten10 1016@j Jacc 2019 01 011Gaby AlboresNoch keine Bewertungen
- Delayed Sequence Intubation: A Prospective Observational StudyDokument8 SeitenDelayed Sequence Intubation: A Prospective Observational StudyRenzo Iván Marín DávalosNoch keine Bewertungen
- ASCIA Guidelines Acute Management Anaphylaxis 2019Dokument8 SeitenASCIA Guidelines Acute Management Anaphylaxis 2019Asadulla KhanNoch keine Bewertungen
- JurnalDokument14 SeitenJurnalCendekiaNoch keine Bewertungen
- ) Ptqjubmfwbdvbujpoqmboojoh Bttfttnfou QfsgpsnbodfboefwbmvbujpoDokument7 Seiten) Ptqjubmfwbdvbujpoqmboojoh Bttfttnfou QfsgpsnbodfboefwbmvbujpoRenzo Iván Marín DávalosNoch keine Bewertungen
- Diagnostic Accuracy of A New High-Sensitivity Troponin I Assay and Five Accelerated Diagnostic Pathways For Ruling Out Acute Myocardial Infarction and Acute Coronary SyndromeDokument16 SeitenDiagnostic Accuracy of A New High-Sensitivity Troponin I Assay and Five Accelerated Diagnostic Pathways For Ruling Out Acute Myocardial Infarction and Acute Coronary SyndromeRenzo Iván Marín DávalosNoch keine Bewertungen
- 2019 Hypertensive Disorders of PregnancyDokument16 Seiten2019 Hypertensive Disorders of PregnancyMaria del Pilar Devis MoralesNoch keine Bewertungen
- 10 1016@j Jacc 2019 01 011Dokument52 Seiten10 1016@j Jacc 2019 01 011Gaby AlboresNoch keine Bewertungen
- Covid19treatmentguidelines PDFDokument124 SeitenCovid19treatmentguidelines PDFMaria Bolivia Rothe CabaNoch keine Bewertungen
- Sd. Guillain Barré PDFDokument15 SeitenSd. Guillain Barré PDFHabib G. Moutran BarrosoNoch keine Bewertungen
- Covid19treatmentguidelines PDFDokument124 SeitenCovid19treatmentguidelines PDFMaria Bolivia Rothe CabaNoch keine Bewertungen
- To Intubate or Not To Intubate: Emergency Medicine Physicians' Perspective On Intubating Critically Ill, Terminal Cancer PatientsDokument8 SeitenTo Intubate or Not To Intubate: Emergency Medicine Physicians' Perspective On Intubating Critically Ill, Terminal Cancer PatientsRenzo Iván Marín DávalosNoch keine Bewertungen
- ) Ptqjubmfwbdvbujpoqmboojoh Bttfttnfou QfsgpsnbodfboefwbmvbujpoDokument7 Seiten) Ptqjubmfwbdvbujpoqmboojoh Bttfttnfou QfsgpsnbodfboefwbmvbujpoRenzo Iván Marín DávalosNoch keine Bewertungen
- Coronavirus-COVID-19 2 PDFDokument22 SeitenCoronavirus-COVID-19 2 PDFByron Reyes Saà100% (1)
- To Intubate or Not To Intubate: Emergency Medicine Physicians' Perspective On Intubating Critically Ill, Terminal Cancer PatientsDokument8 SeitenTo Intubate or Not To Intubate: Emergency Medicine Physicians' Perspective On Intubating Critically Ill, Terminal Cancer PatientsRenzo Iván Marín DávalosNoch keine Bewertungen
- ) Ptqjubmfwbdvbujpoqmboojoh Bttfttnfou QfsgpsnbodfboefwbmvbujpoDokument7 Seiten) Ptqjubmfwbdvbujpoqmboojoh Bttfttnfou QfsgpsnbodfboefwbmvbujpoRenzo Iván Marín DávalosNoch keine Bewertungen
- The Bougie and First-Pass Success in The Emergency DepartmentDokument7 SeitenThe Bougie and First-Pass Success in The Emergency DepartmentRenzo Iván Marín DávalosNoch keine Bewertungen
- Ten Laws of BoundariesDokument17 SeitenTen Laws of Boundariesstjohn30067% (3)
- 1 s2.0 S0149763418301957 MainDokument24 Seiten1 s2.0 S0149763418301957 MainjackNoch keine Bewertungen
- Rtaa SB 4 - 10011991Dokument6 SeitenRtaa SB 4 - 10011991alcomech100% (3)
- Nigeria Trainers ManualDokument131 SeitenNigeria Trainers ManualVivi ALNoch keine Bewertungen
- ADA Concept GuideDokument10 SeitenADA Concept GuidemoalpohoNoch keine Bewertungen
- Butonal NS 175 TDSDokument2 SeitenButonal NS 175 TDSPT. PITAGORAS KONSULTANNoch keine Bewertungen
- Ciso Workshop 2 Security Management PDFDokument37 SeitenCiso Workshop 2 Security Management PDFHigino Domingos de Almeida JoãoNoch keine Bewertungen
- 1 s2.0 S0016706105000467 MainDokument12 Seiten1 s2.0 S0016706105000467 MainLeonardo JaimesNoch keine Bewertungen
- Elements (Industrial Plant)Dokument5 SeitenElements (Industrial Plant)Veralyn Mae BondadNoch keine Bewertungen
- Antihyperlipidemic AgentsDokument71 SeitenAntihyperlipidemic AgentsFirda100% (1)
- Simonson 20033wDokument15 SeitenSimonson 20033wbahrul.hidayah@yahoo.comNoch keine Bewertungen
- 02AdvancedThinkAhead1 Term3 TL2Dokument4 Seiten02AdvancedThinkAhead1 Term3 TL2marina dominguez sanchezNoch keine Bewertungen
- Genie Z45.25 J Internal Combustion - Service Manual - Part No. 219418Dokument331 SeitenGenie Z45.25 J Internal Combustion - Service Manual - Part No. 219418marciogianottiNoch keine Bewertungen
- FOCAL DYSTONIA-A NEUROLOGICAL CONDITION-TREATED WITH CAUSTICUM - Karl Robinson MDDokument2 SeitenFOCAL DYSTONIA-A NEUROLOGICAL CONDITION-TREATED WITH CAUSTICUM - Karl Robinson MDFaker FockerNoch keine Bewertungen
- Climate and Cultural IdentityDokument2 SeitenClimate and Cultural IdentityCha AbolucionNoch keine Bewertungen
- 02-Plant Morphology (Exercise)Dokument5 Seiten02-Plant Morphology (Exercise)varshavishuNoch keine Bewertungen
- TLE Pre-Assessment Most & Least Learned SkillsDokument7 SeitenTLE Pre-Assessment Most & Least Learned SkillsRd DavidNoch keine Bewertungen
- Higuey, Dom Rep Mdpc/Puj: .Eff.23.MayDokument5 SeitenHiguey, Dom Rep Mdpc/Puj: .Eff.23.MayVanessa Yumayusa0% (1)
- Cognitive and Psychopathological Aspects of Ehlers DanlosDokument5 SeitenCognitive and Psychopathological Aspects of Ehlers DanlosKarel GuevaraNoch keine Bewertungen
- Guerra, Germae Joyce - Media JournalDokument2 SeitenGuerra, Germae Joyce - Media JournalGERMAE JOYCE GUERRANoch keine Bewertungen
- Res Ipsa LoquiturDokument6 SeitenRes Ipsa LoquiturZydalgLadyz NeadNoch keine Bewertungen
- CoWIN Portal StepsDokument23 SeitenCoWIN Portal StepsU VenkateshNoch keine Bewertungen
- Sara Salon and SpaDokument4 SeitenSara Salon and Spasania zehraNoch keine Bewertungen
- Boiler BlowdownDokument2 SeitenBoiler BlowdownbaratheonNoch keine Bewertungen
- Bed MakingDokument14 SeitenBed MakingHarold Haze Cortez100% (1)
- EN Project LogisticsDokument2 SeitenEN Project Logisticsdevie shyntiaNoch keine Bewertungen
- Duty Resume ReportDokument1 SeiteDuty Resume ReportaleemuddinNoch keine Bewertungen
- Effects of Climate ChangeDokument10 SeitenEffects of Climate ChangeJan100% (1)
- O-Rings & SealsDokument10 SeitenO-Rings & SealsPartsGopher.comNoch keine Bewertungen
- Design and PlanningDokument15 SeitenDesign and PlanningZeljkoSipcicNoch keine Bewertungen