Das könnte Ihnen auch gefallen
- Comparative Study of Various Brands in Atorvastatin TherapyDokument53 SeitenComparative Study of Various Brands in Atorvastatin TherapyUttam Kr PatraNoch keine Bewertungen
- Pharmacy Service PolicyDokument3 SeitenPharmacy Service PolicydmuscleNoch keine Bewertungen
- Daptomycin (Cubicin)Dokument1 SeiteDaptomycin (Cubicin)Adrianne BazoNoch keine Bewertungen
- Vancomycin Protocol RQHRDokument15 SeitenVancomycin Protocol RQHRl1o2stNoch keine Bewertungen
- Generic Name T Rade Name Classification Minitran Anti Angina NitroglycerinDokument1 SeiteGeneric Name T Rade Name Classification Minitran Anti Angina NitroglycerinChristopher LeeNoch keine Bewertungen
- Drugs To Watch With WARFARINDokument3 SeitenDrugs To Watch With WARFARINRajendra RaiNoch keine Bewertungen
- Drug InteractionsDokument21 SeitenDrug InteractionsPawan Deshmukh100% (1)
- Drug Study: ER DrugsDokument5 SeitenDrug Study: ER Drugsmaeca101Noch keine Bewertungen
- Diabetes Type 2 HassanDokument26 SeitenDiabetes Type 2 Hassanyash_acharya007100% (1)
- Generic Name FurosemideDokument1 SeiteGeneric Name FurosemideChristopher LeeNoch keine Bewertungen
- Challenges in Hypertension ManagementDokument86 SeitenChallenges in Hypertension ManagementAdel SALLAMNoch keine Bewertungen
- Therapeutic Hypothermia Niraj BharuchDokument31 SeitenTherapeutic Hypothermia Niraj BharuchNiraj GuptaNoch keine Bewertungen
- Midazolam FinalDokument2 SeitenMidazolam FinalAhmad AbqariNoch keine Bewertungen
- Antiviral DrugsDokument56 SeitenAntiviral DrugsciccianoNoch keine Bewertungen
- Pharmacology Antimycobacterial DrugsDokument9 SeitenPharmacology Antimycobacterial Drugsroyce charlieNoch keine Bewertungen
- Drug ListsDokument10 SeitenDrug ListsAmber Merritt100% (1)
- Emergency Medicine ListDokument1 SeiteEmergency Medicine ListmomnaNoch keine Bewertungen
- Opioid Analgesics: Just in Time Training September 2006Dokument16 SeitenOpioid Analgesics: Just in Time Training September 2006Yel CMNoch keine Bewertungen
- Medication Card LisinoprilDokument1 SeiteMedication Card LisinoprilTSPANNoch keine Bewertungen
- Patient Case - Vpa ToxicityDokument13 SeitenPatient Case - Vpa Toxicityapi-611386981Noch keine Bewertungen
- Levaquin Drug CardDokument1 SeiteLevaquin Drug CardSheri490100% (1)
- IV PO Conversion CAPDokument3 SeitenIV PO Conversion CAPdamondouglasNoch keine Bewertungen
- Generic Menu - Tgp3Dokument16 SeitenGeneric Menu - Tgp3Jan Clarise Geronimo MacalaladNoch keine Bewertungen
- A Guide On Intravenous Drug Compatibilities Based On Their PHDokument10 SeitenA Guide On Intravenous Drug Compatibilities Based On Their PHSergio M JuniorNoch keine Bewertungen
- IvabradineDokument33 SeitenIvabradinepashaNoch keine Bewertungen
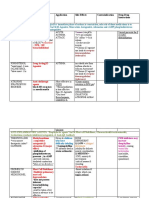
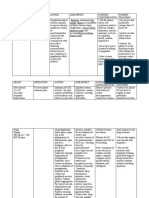
- Drug Name Mechanism Application Side Effects Contraindication Drug-Drug InteractionsDokument3 SeitenDrug Name Mechanism Application Side Effects Contraindication Drug-Drug Interactionsazhar hussinNoch keine Bewertungen
- Journal Reading EMPEROR-ReducedDokument21 SeitenJournal Reading EMPEROR-ReducedLolii Con Harhazyuku100% (1)
- LovenoxDokument1 SeiteLovenoxKatie McPeek100% (2)
- Aminophylline GuidelinesDokument2 SeitenAminophylline GuidelinesA. Shamshir A. MoktiNoch keine Bewertungen
- Aerovent, Apovent Atronase, Ipraxa, Ipvent Rhinovent, Rinatecrinovagos, Atrovent, Atrovent HfaDokument4 SeitenAerovent, Apovent Atronase, Ipraxa, Ipvent Rhinovent, Rinatecrinovagos, Atrovent, Atrovent HfaGwyn RosalesNoch keine Bewertungen
- OsteoporosisDokument19 SeitenOsteoporosisLasa SiahaanNoch keine Bewertungen
- C. Anti-Hypertensive Drugs.Dokument10 SeitenC. Anti-Hypertensive Drugs.Nabeel AsifNoch keine Bewertungen
- With Dr. Susan Lipsett: Community Acquired PneumoniaDokument1 SeiteWith Dr. Susan Lipsett: Community Acquired PneumoniaJayantiNoch keine Bewertungen
- Generic Name T Rade Name Classification Diltiazem Cardizem Antianginals, AntiarrhythmicsDokument1 SeiteGeneric Name T Rade Name Classification Diltiazem Cardizem Antianginals, AntiarrhythmicsChristopher LeeNoch keine Bewertungen
- CV 12-29-19Dokument7 SeitenCV 12-29-19api-507198061Noch keine Bewertungen
- Drug-Resistant TB TreatmentDokument120 SeitenDrug-Resistant TB TreatmentNadzhin15Noch keine Bewertungen
- Antihyperglycemic Agents Comparison ChartDokument9 SeitenAntihyperglycemic Agents Comparison ChartBonnieNoch keine Bewertungen
- ZoloftDokument26 SeitenZoloftgofastjayNoch keine Bewertungen
- Side Effects of Pregabalin DrugDokument20 SeitenSide Effects of Pregabalin DrugtulipcatcherNoch keine Bewertungen
- Antihyperglycemic Agents Comparison Chart PDFDokument9 SeitenAntihyperglycemic Agents Comparison Chart PDFconcoz100% (1)
- H-Southend Critical Medicines ListDokument7 SeitenH-Southend Critical Medicines ListWidya ChalluphytaOzha BiyandNoch keine Bewertungen
- Hypertension Drugs Cheat Sheet: by ViaDokument3 SeitenHypertension Drugs Cheat Sheet: by ViaGulzaib KhokharNoch keine Bewertungen
- Prozac (Fluoxetine) 40mgDokument1 SeiteProzac (Fluoxetine) 40mgENoch keine Bewertungen
- Obese Patients - Medication Dosing RQHR - 3Dokument8 SeitenObese Patients - Medication Dosing RQHR - 3Sarah Zielda NajibNoch keine Bewertungen
- Nstemi: How To Risk Stratify?Dokument32 SeitenNstemi: How To Risk Stratify?dhannibernadetNoch keine Bewertungen
- Ancef Drug CardDokument1 SeiteAncef Drug CardSheri490Noch keine Bewertungen
- Anticholinergics Study Drug ListDokument1 SeiteAnticholinergics Study Drug ListDrima Edi100% (1)
- Drug Study (Pe)Dokument15 SeitenDrug Study (Pe)Jobelle AcenaNoch keine Bewertungen
- (CV2) Pharmacology of AnticoagulantsDokument6 Seiten(CV2) Pharmacology of AnticoagulantsHanifa Shereen B. AliNoch keine Bewertungen
- All Other ClassificationsDokument6 SeitenAll Other ClassificationsCorey100% (1)
- DRUGSDokument5 SeitenDRUGSDanica EspejoNoch keine Bewertungen
- FinasterideDokument2 SeitenFinasterideSyokoyolanting DondonNoch keine Bewertungen
- State Board of PharmacyDokument66 SeitenState Board of PharmacyAnonymous hF5zAdvwCC100% (1)
- Quick Reference DMARDsDokument12 SeitenQuick Reference DMARDsEman MohamedNoch keine Bewertungen
- Soal EthicalDokument12 SeitenSoal EthicalAdelina AfrianiNoch keine Bewertungen
- Obat High Alert Dan LasaDokument2 SeitenObat High Alert Dan LasaAsri MNoch keine Bewertungen
- Gastrointestinal Tract Drugs: Pharmacist Marwan QasimDokument20 SeitenGastrointestinal Tract Drugs: Pharmacist Marwan QasimWaliNoch keine Bewertungen
- جرعات الاطفالDokument50 Seitenجرعات الاطفالWael Hamdy100% (1)
- Drug MenuDokument17 SeitenDrug MenukathlynmangasiNoch keine Bewertungen
- Quick Reference Guide April 2019 PDFDokument2 SeitenQuick Reference Guide April 2019 PDFAaron ShokarNoch keine Bewertungen
- Wet Mount Proficiency 2008A Critique2Dokument4 SeitenWet Mount Proficiency 2008A Critique2Anonymous bq4KY0mcWGNoch keine Bewertungen
- King & Pinger, Pearls of Midwifery PDFDokument14 SeitenKing & Pinger, Pearls of Midwifery PDFAnonymous bq4KY0mcWGNoch keine Bewertungen
- Wet Mount Proficiency 2007A CritiqueDokument6 SeitenWet Mount Proficiency 2007A CritiqueAnonymous bq4KY0mcWGNoch keine Bewertungen
- 1990-Fleming Suturing Method and PainDokument7 Seiten1990-Fleming Suturing Method and PainAnonymous bq4KY0mcWG0% (1)
- Kennedy-Model of Exemplary Midwifery PracticeDokument16 SeitenKennedy-Model of Exemplary Midwifery PracticeAnonymous bq4KY0mcWGNoch keine Bewertungen
- LOC Certificate For 'Assessing COPD in Primary Care - 0.5 Credit PDFDokument1 SeiteLOC Certificate For 'Assessing COPD in Primary Care - 0.5 Credit PDFAnonymous bq4KY0mcWGNoch keine Bewertungen
- Erwin-Demystifying The Nurse-Midwifery MGMT Process 1987Dokument7 SeitenErwin-Demystifying The Nurse-Midwifery MGMT Process 1987Anonymous bq4KY0mcWGNoch keine Bewertungen
- National Diabetes Fact Sheet, 2011: Diabetes Affects 25.8 Million People 8.3% of The U.S. PopulationDokument12 SeitenNational Diabetes Fact Sheet, 2011: Diabetes Affects 25.8 Million People 8.3% of The U.S. PopulationAnonymous bq4KY0mcWGNoch keine Bewertungen
- A Healthy Menopause: Diet, Nutrition and Lifestyle GuidanceDokument8 SeitenA Healthy Menopause: Diet, Nutrition and Lifestyle GuidanceAnonymous bq4KY0mcWGNoch keine Bewertungen
- Fetal DevelopmentDokument4 SeitenFetal DevelopmentAnonymous bq4KY0mcWGNoch keine Bewertungen
- Clinical Pearl TalkDokument26 SeitenClinical Pearl TalkAnonymous bq4KY0mcWGNoch keine Bewertungen
- JNC8 HTNDokument2 SeitenJNC8 HTNTaradifaNurInsi0% (1)
- 2017 JNC 8 Lipid and HTN GuidelinesDokument28 Seiten2017 JNC 8 Lipid and HTN GuidelinesAnonymous bq4KY0mcWGNoch keine Bewertungen
- 1APHA2012HVNAslide2012 10 23handoutDokument34 Seiten1APHA2012HVNAslide2012 10 23handoutAnonymous bq4KY0mcWGNoch keine Bewertungen
- Commonly Prescribed Insulin ProductsDokument1 SeiteCommonly Prescribed Insulin ProductsAnonymous bq4KY0mcWGNoch keine Bewertungen
- Nonhospital SettingDokument17 SeitenNonhospital SettingAnonymous bq4KY0mcWGNoch keine Bewertungen
- Kidney TransplantDokument6 SeitenKidney TransplantAnonymous bq4KY0mcWGNoch keine Bewertungen
- U G I D M: Sing The Lycemic Ndex IN Iabetes AnagementDokument2 SeitenU G I D M: Sing The Lycemic Ndex IN Iabetes AnagementAnonymous bq4KY0mcWGNoch keine Bewertungen
- Finding The BalanceDokument8 SeitenFinding The BalanceAnonymous bq4KY0mcWGNoch keine Bewertungen
- List Obat Obatan LCT PERINTIS UTAMADokument3 SeitenList Obat Obatan LCT PERINTIS UTAMANers SultanNoch keine Bewertungen
- Drugs Used For Treatment of Hypertension: 4/6/2023 DBU, Pharmacology 1Dokument113 SeitenDrugs Used For Treatment of Hypertension: 4/6/2023 DBU, Pharmacology 1BeimnetNoch keine Bewertungen
- 11 Antihypertensive AgentsDokument43 Seiten11 Antihypertensive AgentsAnonymous pmMHrWHdNoch keine Bewertungen
- Nuclear Stress Test Instructions 1Dokument2 SeitenNuclear Stress Test Instructions 1Maria EdelNoch keine Bewertungen
- Review Jurnal Interaksi Obat Antihipertensi - Radhwa Fauztina (20190350050)Dokument13 SeitenReview Jurnal Interaksi Obat Antihipertensi - Radhwa Fauztina (20190350050)Radhwa FauztinaNoch keine Bewertungen
- Masterlist of HPN & DM PT - MHCDokument5 SeitenMasterlist of HPN & DM PT - MHCRannel AragonNoch keine Bewertungen
- Stok Opname Rawat JalanDokument18 SeitenStok Opname Rawat JalandonicrusoeNoch keine Bewertungen
- 1criza Hipertensiva 2018Dokument47 Seiten1criza Hipertensiva 2018NicoletaStanNoch keine Bewertungen
- Atrial Flutter Medication: Drugs DoseDokument8 SeitenAtrial Flutter Medication: Drugs DoseVictoria Castillo TamayoNoch keine Bewertungen
- Free Drug Bank GUIDE 1 PDFDokument76 SeitenFree Drug Bank GUIDE 1 PDFRaouf Ra'fat Soliman100% (11)
- Identification and Determination of Antihypertonics From The Group of Angiotensin Ñ Convertase Inhibitors by Densitometric Method in Comparition With HPLC MethodDokument7 SeitenIdentification and Determination of Antihypertonics From The Group of Angiotensin Ñ Convertase Inhibitors by Densitometric Method in Comparition With HPLC MethodRoberta BotezNoch keine Bewertungen
- Data Expired DateDokument8 SeitenData Expired DateFARMASI PRIMA HUSADA SUKOREJONoch keine Bewertungen
- Hipertensi 2021Dokument121 SeitenHipertensi 2021puskesmas kasihan 1Noch keine Bewertungen
- Asociere Medicamente Si Clasa FarmacoterapeuticaDokument2 SeitenAsociere Medicamente Si Clasa FarmacoterapeuticaEduard MilitaruNoch keine Bewertungen
- Drugs Affecting Cardiac and Renal Systems LecDokument10 SeitenDrugs Affecting Cardiac and Renal Systems LecMichelle ErikaNoch keine Bewertungen
- DiureticsDokument4 SeitenDiureticsNazmul Islam AbirNoch keine Bewertungen
- Bisoprolol in Heart Failure PDFDokument37 SeitenBisoprolol in Heart Failure PDFMega AlmiraNoch keine Bewertungen
- Pencegahan Dan Pengobatan Hipertensi Pada Penderita Usia DewasaDokument7 SeitenPencegahan Dan Pengobatan Hipertensi Pada Penderita Usia DewasaGladys SariowanNoch keine Bewertungen
- CVS MCQsDokument36 SeitenCVS MCQsskNoch keine Bewertungen
- Soha ProtocolDokument5 SeitenSoha ProtocolKantilal NarkhedeNoch keine Bewertungen
- Generic Name Dosage Price: For CoughDokument6 SeitenGeneric Name Dosage Price: For CoughRaffy PangilinanNoch keine Bewertungen
- Pharmacology OF Anti-Hypertensive: Siti SyarifahDokument38 SeitenPharmacology OF Anti-Hypertensive: Siti SyarifahAnnurul Badry IINoch keine Bewertungen
- Código Descripción Costo Unita. Existencia Unidades Costo Existencia Precio 1 %utilDokument24 SeitenCódigo Descripción Costo Unita. Existencia Unidades Costo Existencia Precio 1 %utilNiky Dos SantosNoch keine Bewertungen
- E Cart DrugsDokument2 SeitenE Cart DrugsxmitchxNoch keine Bewertungen
- Stok Opname Obat DetailDokument1 SeiteStok Opname Obat DetailfatihNoch keine Bewertungen
- The JNC 8 Hypertension Guidelines: An In-Depth Guide: Michael R. Page, Pharmd, RPHDokument5 SeitenThe JNC 8 Hypertension Guidelines: An In-Depth Guide: Michael R. Page, Pharmd, RPHdicksonNoch keine Bewertungen
- Lasante CopiDokument12 SeitenLasante Copiluis alberto silva caicedoNoch keine Bewertungen
- Anesthetics: Local Topical: Name Indications Peak Effect (Min) Duration (Min) AmidesDokument3 SeitenAnesthetics: Local Topical: Name Indications Peak Effect (Min) Duration (Min) Amidesammar amerNoch keine Bewertungen
- "Respiratory System" يسفنتلا زاهجلا ةيودأ: 1. Bronchodilator (B2 - selective agonist)Dokument35 Seiten"Respiratory System" يسفنتلا زاهجلا ةيودأ: 1. Bronchodilator (B2 - selective agonist)Ahmed AbdrabouNoch keine Bewertungen
- Logistik Harga Obat (MUTIARA)Dokument3 SeitenLogistik Harga Obat (MUTIARA)EryanaCitaNoch keine Bewertungen