Das könnte Ihnen auch gefallen
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsVon EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNoch keine Bewertungen
- Pre-Hospital Assessment Sheet: Triage ScoreDokument2 SeitenPre-Hospital Assessment Sheet: Triage Scoreratna purwitasariNoch keine Bewertungen
- Atls MedscapeDokument5 SeitenAtls MedscapeCastay GuerraNoch keine Bewertungen
- (Bioethics 2) 3.01.01 - Case - Joyce Brown (Pat G)Dokument2 Seiten(Bioethics 2) 3.01.01 - Case - Joyce Brown (Pat G)MarianneTee-ruh100% (1)
- Intensive Care Trauma SheetDokument2 SeitenIntensive Care Trauma SheetalexipsNoch keine Bewertungen
- Infection Control Questions For StaffDokument3 SeitenInfection Control Questions For StaffManisha maharaNoch keine Bewertungen
- 107 Rle Virtual Duty - Opd: Internal MedicineDokument6 Seiten107 Rle Virtual Duty - Opd: Internal MedicineGiel Margareth LindoNoch keine Bewertungen
- OPD Adolescent History FormDokument5 SeitenOPD Adolescent History FormNehemiah FranciscoNoch keine Bewertungen
- EMS Mass Casualty TriageDokument3 SeitenEMS Mass Casualty TriageRony NurhidayatNoch keine Bewertungen
- Pre Authorization FormDokument1 SeitePre Authorization FormMurugan RamalingamNoch keine Bewertungen
- Emergency Medical TechnicianDokument46 SeitenEmergency Medical TechnicianBill Alfred LaporeNoch keine Bewertungen
- Geriatric Emt QuizDokument6 SeitenGeriatric Emt QuizRebecca Lau0% (1)
- 2 - Airway and Ventilatory ManagementDokument5 Seiten2 - Airway and Ventilatory ManagementJessie E. GeeNoch keine Bewertungen
- BFR 06 - Scene Assessment and SafetyDokument18 SeitenBFR 06 - Scene Assessment and SafetyDex Valdez100% (1)
- Atls Important Notes Triage: Ali M. Ahmad Consultant Pediatric SurgeryDokument55 SeitenAtls Important Notes Triage: Ali M. Ahmad Consultant Pediatric SurgeryAndris TapaNoch keine Bewertungen
- Mental Health Powerpoint Eng Comp 2Dokument8 SeitenMental Health Powerpoint Eng Comp 2api-549191753Noch keine Bewertungen
- Trauma SheetDokument1 SeiteTrauma SheetbrownehsNoch keine Bewertungen
- Soap Note Template 03Dokument5 SeitenSoap Note Template 03Razan HaimounyNoch keine Bewertungen
- Characteristics of Family MedicineDokument3 SeitenCharacteristics of Family MedicineAn TonNoch keine Bewertungen
- Outline Perioperative NursingDokument8 SeitenOutline Perioperative NursingMM VNoch keine Bewertungen
- Patient History Taking TemplateDokument2 SeitenPatient History Taking TemplateVarshini Tamil SelvanNoch keine Bewertungen
- OEC Chapter 4Dokument10 SeitenOEC Chapter 4Phil McLeanNoch keine Bewertungen
- Acute Lymphoblastic LeukemiaDokument25 SeitenAcute Lymphoblastic Leukemiaapi-396564080Noch keine Bewertungen
- Stemi ChecklistDokument1 SeiteStemi ChecklistDanu SusantoNoch keine Bewertungen
- Pain: Onset: Provocation: Mental Status Airway Skin Moisture Pulse Color TempDokument4 SeitenPain: Onset: Provocation: Mental Status Airway Skin Moisture Pulse Color TempAlvarez StevenNoch keine Bewertungen
- Abdominal Pain History TakingDokument8 SeitenAbdominal Pain History TakingParth PatelNoch keine Bewertungen
- Vital Signs Reference Chart 1.2 - 1 PDFDokument1 SeiteVital Signs Reference Chart 1.2 - 1 PDFSerious Leo100% (1)
- ECG Brief NotesDokument5 SeitenECG Brief NotesKalpani Malsha UdawelagedaraNoch keine Bewertungen
- ACLS Study GuideDokument30 SeitenACLS Study GuidemmmmzNoch keine Bewertungen
- Acute Burns Case StudyDokument6 SeitenAcute Burns Case StudyErica MeyersNoch keine Bewertungen
- Prophylactic ETT 6yr Fail IV 2: Primary Survey 1.airway 3.circulationDokument17 SeitenProphylactic ETT 6yr Fail IV 2: Primary Survey 1.airway 3.circulationURo KkuNoch keine Bewertungen
- AbbreviationDokument19 SeitenAbbreviationJayson NatividadNoch keine Bewertungen
- Revise ELECTROCARDIOGRAM MONITORINGDokument2 SeitenRevise ELECTROCARDIOGRAM MONITORINGsenyorakath100% (1)
- Blunt Trauma AbdomenDokument41 SeitenBlunt Trauma AbdomenSanthanu SukumaranNoch keine Bewertungen
- Cardiac ArrestDokument10 SeitenCardiac ArrestFebby Aulia AriefNoch keine Bewertungen
- Case Study: Exercise 2: Triage 1Dokument26 SeitenCase Study: Exercise 2: Triage 1Chandra DewiNoch keine Bewertungen
- Blood Pressure ChartDokument9 SeitenBlood Pressure Chartver_at_workNoch keine Bewertungen
- Health HistoryDokument12 SeitenHealth HistoryGreta D RNNoch keine Bewertungen
- Elderly AbuseDokument6 SeitenElderly AbuseKyte100% (1)
- Pathophysiology of Shock Sepsis and Organ Failure PDFDokument1.179 SeitenPathophysiology of Shock Sepsis and Organ Failure PDFNotInterested100% (1)
- Preoperative Preparation of The Surgical PatientDokument33 SeitenPreoperative Preparation of The Surgical PatientPrincewill SeiyefaNoch keine Bewertungen
- StrokeDokument6 SeitenStrokebrendavenegasNoch keine Bewertungen
- Philippine Pediatric Society in Cooperation With The Society of Pediatric Critical Care Medicine, PhilippinesDokument32 SeitenPhilippine Pediatric Society in Cooperation With The Society of Pediatric Critical Care Medicine, PhilippinesShari TernolaNoch keine Bewertungen
- Appendix B-Acceptable AcronymsDokument11 SeitenAppendix B-Acceptable AcronymsKimberly SolisNoch keine Bewertungen
- Taking Blood Pressure ManuallyDokument2 SeitenTaking Blood Pressure ManuallyManoj Kumar GNoch keine Bewertungen
- Chest Trauma: Prepared By: Bill Milan Nremt-P, Ccemt-PDokument79 SeitenChest Trauma: Prepared By: Bill Milan Nremt-P, Ccemt-PEryanda DinataNoch keine Bewertungen
- ASA ClassificationDokument20 SeitenASA ClassificationDeepak SolankiNoch keine Bewertungen
- MCI Drill Sample ScenariosDokument8 SeitenMCI Drill Sample ScenariosDarylNoch keine Bewertungen
- Communicable Disease ChartDokument4 SeitenCommunicable Disease ChartSanjeev Kumar0% (1)
- International Recruitment Application Form (New)Dokument5 SeitenInternational Recruitment Application Form (New)EL SHITANoch keine Bewertungen
- Bites and Stings PPT Fix DR IsyaDokument61 SeitenBites and Stings PPT Fix DR IsyamadeNoch keine Bewertungen
- Pediatric Cardiovascular DiseasesDokument4 SeitenPediatric Cardiovascular DiseasesWendy EscalanteNoch keine Bewertungen
- Responding To A Code BlueDokument33 SeitenResponding To A Code Blueamanrup randhawaNoch keine Bewertungen
- Health History Documentation Form ChristinaDokument6 SeitenHealth History Documentation Form Christinaapi-545542584Noch keine Bewertungen
- Iii. Physical Assessment and Review of SystemDokument7 SeitenIii. Physical Assessment and Review of SystemBiya MacunteNoch keine Bewertungen
- Ketikkan Emergency HostDokument2 SeitenKetikkan Emergency HostBella ApNoch keine Bewertungen
- Nursing Head To Toe Assessment Checklist Revised SP 2013Dokument3 SeitenNursing Head To Toe Assessment Checklist Revised SP 2013clarimer100% (3)
- Related Learning Experience Requirements For Medical and Surgical Ward AreasDokument14 SeitenRelated Learning Experience Requirements For Medical and Surgical Ward AreasDummy AccountNoch keine Bewertungen
- RevisedDokument16 SeitenRevisedZymer Lee AbasoloNoch keine Bewertungen
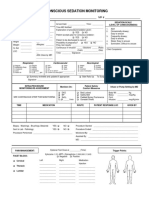
- 34 An Consious Sedation MonitoringDokument2 Seiten34 An Consious Sedation Monitoringabu alauon abed almohsenNoch keine Bewertungen
- 1 Relative Maxima, Relative Minima and Saddle PointsDokument3 Seiten1 Relative Maxima, Relative Minima and Saddle PointsRoy VeseyNoch keine Bewertungen
- Why I Want To Be An Army OfficerDokument1 SeiteWhy I Want To Be An Army OfficercmphalanNoch keine Bewertungen
- X2ho LteDokument7 SeitenX2ho LtePrasoon PuthuvattilNoch keine Bewertungen
- Press ReleaseDokument1 SeitePress Releaseapi-303080489Noch keine Bewertungen
- Perception On The Impact of New Learning Tools in Humss StudentDokument6 SeitenPerception On The Impact of New Learning Tools in Humss StudentElyza Marielle BiasonNoch keine Bewertungen
- 1.Gdpr - Preparation Planning GanttDokument6 Seiten1.Gdpr - Preparation Planning GanttbeskiNoch keine Bewertungen
- Blind Chinese SoldiersDokument2 SeitenBlind Chinese SoldiersSampolNoch keine Bewertungen
- Uttar Pradesh Universities Act 1973Dokument73 SeitenUttar Pradesh Universities Act 1973ifjosofNoch keine Bewertungen
- AIW Unit Plan - Ind. Tech ExampleDokument4 SeitenAIW Unit Plan - Ind. Tech ExampleMary McDonnellNoch keine Bewertungen
- Unit 1session 2 Performance MGMTDokument38 SeitenUnit 1session 2 Performance MGMTMayank TrivediNoch keine Bewertungen
- Info Cad Engb FestoDokument14 SeitenInfo Cad Engb FestoBayu RahmansyahNoch keine Bewertungen
- PG 19 - 20 GROUP 5Dokument2 SeitenPG 19 - 20 GROUP 5Kevin Luis Pacheco ZarateNoch keine Bewertungen
- The Use of Images by Claudius ClaudianusDokument66 SeitenThe Use of Images by Claudius ClaudianusDracostinarumNoch keine Bewertungen
- Cns Spectrums: The Clinical Challenges of Akathisia CME Review ArticleDokument16 SeitenCns Spectrums: The Clinical Challenges of Akathisia CME Review Articledzakiyah nurul israNoch keine Bewertungen
- An Objective of Dress Code PolicyDokument4 SeitenAn Objective of Dress Code PolicySiddhraj Singh KushwahaNoch keine Bewertungen
- The First Quality Books To ReadDokument2 SeitenThe First Quality Books To ReadMarvin I. NoronaNoch keine Bewertungen
- Gullivers TravelDokument3 SeitenGullivers TravelRanen Das MishukNoch keine Bewertungen
- Scholarly Article: Ritam Mukherjee: Post-Tagore Bengali Poetry: Image of God' and SecularismDokument6 SeitenScholarly Article: Ritam Mukherjee: Post-Tagore Bengali Poetry: Image of God' and SecularismbankansNoch keine Bewertungen
- Speakout Language BankDokument7 SeitenSpeakout Language BankСаша БулуєвNoch keine Bewertungen
- Management of Breast CancerDokument53 SeitenManagement of Breast CancerGaoudam NatarajanNoch keine Bewertungen
- Low Intermediate Korean Vocabulary and GrammarDokument10 SeitenLow Intermediate Korean Vocabulary and GrammarTuong Van Nguyen100% (3)
- Overpressure Prediction From PS Seismic DataDokument10 SeitenOverpressure Prediction From PS Seismic DataSevinj HumbatovaNoch keine Bewertungen
- Sec 25 HmaDokument3 SeitenSec 25 HmaMukul BajajNoch keine Bewertungen
- Beginner Levels of EnglishDokument4 SeitenBeginner Levels of EnglishEduardoDiazNoch keine Bewertungen
- 4 Problem GamblingDokument14 Seiten4 Problem GamblingLee Jia HuiNoch keine Bewertungen
- Rousseau NotesDokument4 SeitenRousseau NotesAkhilesh IssurNoch keine Bewertungen
- G.R. No. 205307 PEOPLE Vs EDUARDO GOLIDAN y COTO-ONGDokument24 SeitenG.R. No. 205307 PEOPLE Vs EDUARDO GOLIDAN y COTO-ONGRuel FernandezNoch keine Bewertungen
- DB2 UsefullcommandDokument8 SeitenDB2 Usefullcommandganeshreddy_dspxNoch keine Bewertungen
- Brent Berlin-Covert Categories and Folk TaxonomyDokument10 SeitenBrent Berlin-Covert Categories and Folk TaxonomyKawita ChuachengNoch keine Bewertungen
- Impulsive Buying PDFDokument146 SeitenImpulsive Buying PDFrukwavuNoch keine Bewertungen