Das könnte Ihnen auch gefallen
- Asthma or Copd Case StudyDokument10 SeitenAsthma or Copd Case StudyMahendra ShrimaliNoch keine Bewertungen
- GERD (Gastroesophageal Reflux Disease)Dokument112 SeitenGERD (Gastroesophageal Reflux Disease)Mharj Alfelor Cecilio100% (7)
- Urine Dipstick Testing Everything You Need To.33Dokument4 SeitenUrine Dipstick Testing Everything You Need To.33Brad GreyNoch keine Bewertungen
- Pulmonary Function Testing1Dokument51 SeitenPulmonary Function Testing1kusaarNoch keine Bewertungen
- Algorithms For DyspneaDokument2 SeitenAlgorithms For DyspneaJE AsuncionNoch keine Bewertungen
- Pneumonia Case StudyDokument24 SeitenPneumonia Case StudyDharylle Cariño100% (1)
- Fact Sheet YaconDokument2 SeitenFact Sheet YaconTrilceNoch keine Bewertungen
- Cases and Doctrines On Legal MedicineDokument44 SeitenCases and Doctrines On Legal MedicineEliza MontemayorNoch keine Bewertungen
- Spirometry Step by StepDokument9 SeitenSpirometry Step by StepAndry Wahyudi AgusNoch keine Bewertungen
- Radiation Therapy For Breast Cancer 2016Dokument162 SeitenRadiation Therapy For Breast Cancer 2016Alexandra Nicoleta Teisi100% (1)
- Complete DentureDokument57 SeitenComplete Denturedr_ahmad_zuhdi100% (3)
- Pedia 3.1 Pediatric PulmoDokument8 SeitenPedia 3.1 Pediatric PulmoAswanth ThisaiveeranNoch keine Bewertungen
- RestorilDokument1 SeiteRestorilKatie McPeek100% (1)
- Nursing Care Plan: Lorma Colleges Con Template Related Learning ExperienceDokument6 SeitenNursing Care Plan: Lorma Colleges Con Template Related Learning ExperiencePauline GarciaNoch keine Bewertungen
- Assessment Diagnosis Planning Intervention Rationale Evaluation SubjectiveDokument4 SeitenAssessment Diagnosis Planning Intervention Rationale Evaluation Subjectivecammel ramos100% (1)
- Peak Flow MeterDokument4 SeitenPeak Flow Meterteti0% (1)
- Indrabasti Marma2Dokument4 SeitenIndrabasti Marma2Rajiv SharmaNoch keine Bewertungen
- NCP Ineffective Breathing PatternDokument3 SeitenNCP Ineffective Breathing PatternEds Sy50% (4)
- Respirology 2023 FinalDokument127 SeitenRespirology 2023 FinalBelinda ELISHANoch keine Bewertungen
- Case Presentation OF: Iron Deficiency AnemiaDokument33 SeitenCase Presentation OF: Iron Deficiency Anemiaitshurt_teardrops100% (1)
- Carcinoma Rectum - Janak - NEWDokument74 SeitenCarcinoma Rectum - Janak - NEWTowhidulIslamNoch keine Bewertungen
- Carcinoma Rectum - Janak - NEWDokument74 SeitenCarcinoma Rectum - Janak - NEWTowhidulIslamNoch keine Bewertungen
- Dhaka North City CorporatationDokument9 SeitenDhaka North City Corporatationathiqul100% (4)
- The Appropriate Amount of Oxygen Is Continuously Delivered So That The Patient Does Not DesiderateDokument4 SeitenThe Appropriate Amount of Oxygen Is Continuously Delivered So That The Patient Does Not DesideratezheeraNoch keine Bewertungen
- NCP - Or-Rotation 2Dokument12 SeitenNCP - Or-Rotation 2Vian RiveraNoch keine Bewertungen
- Case Conferences: The Expert ClinicianDokument5 SeitenCase Conferences: The Expert ClinicianMayNoch keine Bewertungen
- c64 Section3 Spirometry 2014Dokument19 Seitenc64 Section3 Spirometry 2014Mihai PetrescuNoch keine Bewertungen
- Spiro Me Try Cheat Sheet 09Dokument2 SeitenSpiro Me Try Cheat Sheet 09Yudha Perwira PutraNoch keine Bewertungen
- Alterations in OxygenationDokument6 SeitenAlterations in OxygenationAUBREY MARIE . GUERRERONoch keine Bewertungen
- Lectura 3Dokument13 SeitenLectura 3MB ValdiviaNoch keine Bewertungen
- 4 2020 Spirometry Quick Glance GuideDokument2 Seiten4 2020 Spirometry Quick Glance Guidepatrick_raj884545Noch keine Bewertungen
- Nursing Care Plan Impaired Gas ExchangeDokument1 SeiteNursing Care Plan Impaired Gas ExchangeKarylle PetilNoch keine Bewertungen
- Blouet 2018 SDokument10 SeitenBlouet 2018 SnarykNoch keine Bewertungen
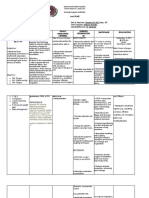
- Procedure/S Indication/S Result/S Normal Values Implications Nursing ResponsibilitiesDokument9 SeitenProcedure/S Indication/S Result/S Normal Values Implications Nursing Responsibilitiesmyer pasandalanNoch keine Bewertungen
- NCP and Drug StudyDokument7 SeitenNCP and Drug StudyKirsty Marie SupranesNoch keine Bewertungen
- 76 AcutePB840PAVPlusMgmtProtocolSS10VE5543 1316719265 PDFDokument2 Seiten76 AcutePB840PAVPlusMgmtProtocolSS10VE5543 1316719265 PDFNATHALIA MORENO PERILLANoch keine Bewertungen
- Spirometry Step by Step PDFDokument9 SeitenSpirometry Step by Step PDFwesdNoch keine Bewertungen
- Spirometry: Performance and Interpretation A Guide For General PractitionersDokument15 SeitenSpirometry: Performance and Interpretation A Guide For General PractitionersAgi AngloSaxonNoch keine Bewertungen
- Case PresentationDokument5 SeitenCase PresentationJARIETTA OCHOANoch keine Bewertungen
- Pulmonary Tuberculosis G3Dokument12 SeitenPulmonary Tuberculosis G3Cuttie Anne GalangNoch keine Bewertungen
- Polysom Finals.Dokument9 SeitenPolysom Finals.Guenevere DamasinNoch keine Bewertungen
- Case Study Respiratory DisorderDokument17 SeitenCase Study Respiratory DisorderJester GalayNoch keine Bewertungen
- 5.12.02 How To Interpret Pulmonary Function Tests 1Dokument10 Seiten5.12.02 How To Interpret Pulmonary Function Tests 1Thakoon TtsNoch keine Bewertungen
- Bahagian Iv: Ringkasan Penemuan Yang PentingDokument11 SeitenBahagian Iv: Ringkasan Penemuan Yang PentingBrandon MikeNoch keine Bewertungen
- Ruizo, NCPDokument3 SeitenRuizo, NCPJay Debby RuizoNoch keine Bewertungen
- Pepsi NaDokument11 SeitenPepsi NaOscar OsorioNoch keine Bewertungen
- Protocol and Procedure For Undertaking and Interpreting SpirometryDokument22 SeitenProtocol and Procedure For Undertaking and Interpreting Spirometryolaalsharif2Noch keine Bewertungen
- Labs - Case ConDokument7 SeitenLabs - Case ConDara Sophia EncarguezNoch keine Bewertungen
- Oks Na To Thank U Aubs!!: Okiii!!! Wuv U All!Dokument10 SeitenOks Na To Thank U Aubs!!: Okiii!!! Wuv U All!CiaraNoch keine Bewertungen
- Respiratory High-Flow Therapy Device (H-80A)Dokument4 SeitenRespiratory High-Flow Therapy Device (H-80A)hendranatjNoch keine Bewertungen
- NCP Week 6 Nrg301 ValenzonaDokument3 SeitenNCP Week 6 Nrg301 ValenzonaJoshennaNoch keine Bewertungen
- Final NCPDokument13 SeitenFinal NCPBAGUIO CATSNoch keine Bewertungen
- Vital Signs Taken As FollowsDokument10 SeitenVital Signs Taken As FollowsKyle AndrewNoch keine Bewertungen
- Respiratory PasTest MRCP II 2021Dokument1.050 SeitenRespiratory PasTest MRCP II 2021kathi raja sekharNoch keine Bewertungen
- Group 2B: A Pulmonary Histoplasmosis CaseDokument58 SeitenGroup 2B: A Pulmonary Histoplasmosis CaseAngela NeriNoch keine Bewertungen
- NCP On Ineffective Airway Clearance Nursing Diagnosi S Planning Nursing Interventions Implementatio N Evaluation Subjective: IndependentDokument10 SeitenNCP On Ineffective Airway Clearance Nursing Diagnosi S Planning Nursing Interventions Implementatio N Evaluation Subjective: IndependentSheryhan Tahir BayleNoch keine Bewertungen
- SpirometryDokument29 SeitenSpirometrydrnasir31Noch keine Bewertungen
- A Case Study On AsthmaDokument38 SeitenA Case Study On AsthmaMark Tristan AsuncionNoch keine Bewertungen
- MODULE2Dokument12 SeitenMODULE2Macasieb Renz Jian BalcitaNoch keine Bewertungen
- Directorate General of Health Services, Mohfw, Goi Comprehensive Guidelines For Management of Covid-19 Patients Asymptomatic Mild Moderate SevereDokument2 SeitenDirectorate General of Health Services, Mohfw, Goi Comprehensive Guidelines For Management of Covid-19 Patients Asymptomatic Mild Moderate SevereSpecial OPD SVMCHRCNoch keine Bewertungen
- Sakit Akon Tiyan Kada Mag Ubo-Ubo Ko.": Predisposing Factors: Precipitating FactorsDokument4 SeitenSakit Akon Tiyan Kada Mag Ubo-Ubo Ko.": Predisposing Factors: Precipitating FactorsAl TheóNoch keine Bewertungen
- Respiratory MRCP II Pastest 2023Dokument979 SeitenRespiratory MRCP II Pastest 2023Tanzir Islam BrittoNoch keine Bewertungen
- Smith IOS BasicsDokument37 SeitenSmith IOS Basicssstefan888Noch keine Bewertungen
- Diagnostic Test: Material Needed Management of Time Task Type Notes For TeacherDokument6 SeitenDiagnostic Test: Material Needed Management of Time Task Type Notes For TeacherYuni NatasyaNoch keine Bewertungen
- Comprehensive Life Support Tutorial Case 1: Question/Action Information Note/Reference TipsDokument3 SeitenComprehensive Life Support Tutorial Case 1: Question/Action Information Note/Reference Tipshyukkie minnieNoch keine Bewertungen
- Drugs For COPD: PharmacologyDokument8 SeitenDrugs For COPD: Pharmacologybo gum parkNoch keine Bewertungen
- Minimum Standards of Anorectal Manometry: PurposeDokument7 SeitenMinimum Standards of Anorectal Manometry: PurposesoudrackNoch keine Bewertungen
- Week 7 NCP CHFDokument3 SeitenWeek 7 NCP CHFSeth Michael Daniel BenauroNoch keine Bewertungen
- Faal Paru Dinamis: Jurnal RespirasiDokument8 SeitenFaal Paru Dinamis: Jurnal RespirasiHafis HerdimanNoch keine Bewertungen
- Lung Carcinoma: Radiotherapy PlanningDokument9 SeitenLung Carcinoma: Radiotherapy PlanningTowhidulIslamNoch keine Bewertungen
- Sindrome Mielo DisplásicoDokument28 SeitenSindrome Mielo Displásicolisina293Noch keine Bewertungen
- Gastric Carcinoma: Radiation Planning: Ebrt Assessment of Disease 1. Examinations: 2. Investigations: A. Non-InvasiveDokument33 SeitenGastric Carcinoma: Radiation Planning: Ebrt Assessment of Disease 1. Examinations: 2. Investigations: A. Non-InvasiveTowhidulIslamNoch keine Bewertungen
- COVID Guideline V4.30.3.2020Dokument29 SeitenCOVID Guideline V4.30.3.2020gourabNoch keine Bewertungen
- 0529 Protocol Update 6.2.09 PDFDokument57 Seiten0529 Protocol Update 6.2.09 PDFTowhidulIslamNoch keine Bewertungen
- Adult Body Mass Index (BMI) Chart: WeightDokument2 SeitenAdult Body Mass Index (BMI) Chart: WeightTowhidulIslamNoch keine Bewertungen
- WedgeDokument9 SeitenWedgeTowhidulIslamNoch keine Bewertungen
- How To Detect Bad RAM With The Windows Memory Diagnostic Tool - TechRepublic PDFDokument1 SeiteHow To Detect Bad RAM With The Windows Memory Diagnostic Tool - TechRepublic PDFTowhidulIslamNoch keine Bewertungen
- Youtube by ClickDokument1 SeiteYoutube by ClickTowhidulIslamNoch keine Bewertungen
- Read MeDokument1 SeiteRead MeTowhidulIslamNoch keine Bewertungen
- Horton 2018Dokument15 SeitenHorton 2018TowhidulIslamNoch keine Bewertungen
- Dr. Towhidul Islam: MBBS, BCS (Health) CCD Bangabandhu Sheikh Mujib Medical University Cell Phone: 01725271380Dokument1 SeiteDr. Towhidul Islam: MBBS, BCS (Health) CCD Bangabandhu Sheikh Mujib Medical University Cell Phone: 01725271380TowhidulIslamNoch keine Bewertungen
- Items: No Items For Type NumberDokument1 SeiteItems: No Items For Type NumberTowhidulIslamNoch keine Bewertungen
- The Blockade of Immune Checkpoints Pardoll2012 PDFDokument13 SeitenThe Blockade of Immune Checkpoints Pardoll2012 PDFTowhidulIslamNoch keine Bewertungen
- Horton 2018Dokument5 SeitenHorton 2018TowhidulIslamNoch keine Bewertungen
- Pregnancy Fact SheetDokument3 SeitenPregnancy Fact SheetTowhidulIslamNoch keine Bewertungen
- Horton 2018Dokument15 SeitenHorton 2018TowhidulIslamNoch keine Bewertungen
- WHO and RECIST CriteriaDokument2 SeitenWHO and RECIST CriteriaTowhidulIslamNoch keine Bewertungen
- Diagnstico Diferencial de Vmitos PDFDokument9 SeitenDiagnstico Diferencial de Vmitos PDFLeoberto Batista Pereira SobrinhoNoch keine Bewertungen
- Bronchiolitis Peds.2014 2742.fullDokument32 SeitenBronchiolitis Peds.2014 2742.fullTowhidulIslamNoch keine Bewertungen
- Febrile NeutropeniaDokument7 SeitenFebrile NeutropeniaTowhidulIslamNoch keine Bewertungen
- 2008 RA Recommendations PDFDokument23 Seiten2008 RA Recommendations PDFTowhidulIslamNoch keine Bewertungen
- Analcancer 0617 7908Dokument1 SeiteAnalcancer 0617 7908TowhidulIslamNoch keine Bewertungen
- Abvd Hem HLDokument6 SeitenAbvd Hem HLTowhidulIslamNoch keine Bewertungen
- Normal Tissue Responses To RadiationDokument56 SeitenNormal Tissue Responses To RadiationTowhidulIslamNoch keine Bewertungen
- Ratio: Number Rate of Events, Items, Persons, Etc One Group Number Rate of Events, Items, Persons, Etc Another GroupDokument11 SeitenRatio: Number Rate of Events, Items, Persons, Etc One Group Number Rate of Events, Items, Persons, Etc Another GroupdayafterNoch keine Bewertungen
- GAF 2021 BrochureDokument16 SeitenGAF 2021 BrochureAtulSanapNoch keine Bewertungen
- Principles of Inheritance and Variations MCQs IDokument13 SeitenPrinciples of Inheritance and Variations MCQs IMahendhiran MariappanNoch keine Bewertungen
- Principles of Routine Exodontia 2Dokument55 SeitenPrinciples of Routine Exodontia 2رضوان سهم الموايدNoch keine Bewertungen
- Modified MLKNN AlgorithmDokument11 SeitenModified MLKNN AlgorithmsaurabhNoch keine Bewertungen
- REKAPITULASI PASIEN CA PENIS NewDokument51 SeitenREKAPITULASI PASIEN CA PENIS Newagus sukarnaNoch keine Bewertungen
- Additional Notes On ShockDokument3 SeitenAdditional Notes On ShockSheniqua GreavesNoch keine Bewertungen
- Fon by SatarDokument40 SeitenFon by SatarAqib SatarNoch keine Bewertungen
- Antisocial BehaviorDokument12 SeitenAntisocial BehaviorEdward Ian BelmesNoch keine Bewertungen
- Laporan Kasus Per Gol Umur Feb 2023Dokument7 SeitenLaporan Kasus Per Gol Umur Feb 2023Akreditasi UKPNoch keine Bewertungen
- Datasheet Reagent SansureDokument3 SeitenDatasheet Reagent Sansuredanang setiawanNoch keine Bewertungen
- Vensim Model IndexDokument4 SeitenVensim Model Indexkaren dejoNoch keine Bewertungen
- Molecules - 1 (Carbs & Lipids) V2Dokument13 SeitenMolecules - 1 (Carbs & Lipids) V2ormattNoch keine Bewertungen
- Urtica Urens William Boericke Cyrus Maxwell Bogar Adolf Zur Lippe John Henry ClarkeDokument9 SeitenUrtica Urens William Boericke Cyrus Maxwell Bogar Adolf Zur Lippe John Henry ClarkeShah FaisalNoch keine Bewertungen
- Orthopedic InstrumentsDokument7 SeitenOrthopedic InstrumentsRonnie CanteroNoch keine Bewertungen
- Patient Education: Colic (Excessive Crying) in Infants (Beyond The Basics)Dokument15 SeitenPatient Education: Colic (Excessive Crying) in Infants (Beyond The Basics)krh5fnjnprNoch keine Bewertungen
- LAB 4 - StreptococcusDokument31 SeitenLAB 4 - Streptococcussajad abasNoch keine Bewertungen
- Bharat India: Extremely Bad Status of Testing & VaccinationDokument308 SeitenBharat India: Extremely Bad Status of Testing & VaccinationP Eng Suraj SinghNoch keine Bewertungen
- Opalescence Boost Whitening PDFDokument2 SeitenOpalescence Boost Whitening PDFVikas AggarwalNoch keine Bewertungen
- S 0140525 X 00003368 ADokument59 SeitenS 0140525 X 00003368 AEnver OruroNoch keine Bewertungen
- ElectrocardiogramDokument17 SeitenElectrocardiogramvinnu kalyanNoch keine Bewertungen
- 150 Years of PharmacovigilanceDokument2 Seiten150 Years of PharmacovigilanceCarlos José Lacava Fernández100% (1)
- MenopauseDokument21 SeitenMenopauseDr K AmbareeshaNoch keine Bewertungen