Das könnte Ihnen auch gefallen
- Developmental MilestonesDokument4 SeitenDevelopmental Milestonesschxzerrydawn100% (2)
- Subjective History PediatricDokument4 SeitenSubjective History PediatricAbbyGael Fikri MNoch keine Bewertungen
- Pediatric Assessment&screening ToolsDokument7 SeitenPediatric Assessment&screening Toolsdariand100% (1)
- Physical Examination of The NewbornDokument11 SeitenPhysical Examination of The NewbornJenL100% (3)
- Infant ReflexesDokument41 SeitenInfant ReflexesamwriteaNoch keine Bewertungen
- (3F) Pediatrics - Pediatric HistoryDokument9 Seiten(3F) Pediatrics - Pediatric HistoryNomar Nonato100% (2)
- Pediatric History FormDokument5 SeitenPediatric History FormEssa Smj100% (1)
- Neurologic Examination of Newborn and InfantsDokument6 SeitenNeurologic Examination of Newborn and InfantsRem AlfelorNoch keine Bewertungen
- Ot Guidelines Child SpecificDokument34 SeitenOt Guidelines Child Specific健康生活園Healthy Life Garden100% (1)
- Occupational Therapy Initial EvaluationDokument10 SeitenOccupational Therapy Initial EvaluationNerissa BanguiNoch keine Bewertungen
- Pediatric EvaluationDokument7 SeitenPediatric Evaluationapi-420919156100% (2)
- Developmental MilestonesDokument22 SeitenDevelopmental MilestonesSillmark Bacason100% (3)
- OTR Example QuestionsDokument19 SeitenOTR Example QuestionsSonya100% (1)
- PEDIATRICS Medical History & PE Guide (With Appendix)Dokument34 SeitenPEDIATRICS Medical History & PE Guide (With Appendix)Kathleen Dy100% (2)
- Developmental MilestonesDokument3 SeitenDevelopmental MilestonesElibmasacNoch keine Bewertungen
- PT GoalsDokument13 SeitenPT Goalsnaomi harowNoch keine Bewertungen
- Occupational Therapy in Neonatal Services and Early Intervention PDFDokument152 SeitenOccupational Therapy in Neonatal Services and Early Intervention PDFLauren100% (1)
- Student Treatment Session Soap 8Dokument9 SeitenStudent Treatment Session Soap 8api-340625860100% (1)
- Pediatric Primitive ReflexesDokument2 SeitenPediatric Primitive ReflexesJonathanNoch keine Bewertungen
- Pediatric Growth and DevelopmentDokument9 SeitenPediatric Growth and DevelopmentPaula100% (4)
- Developmental AssessmentDokument13 SeitenDevelopmental AssessmentIsaac Tan100% (1)
- OTR NBCOT ReviewDokument167 SeitenOTR NBCOT ReviewDen Ise100% (1)
- 13 Assessment&screening Tools PDFDokument5 Seiten13 Assessment&screening Tools PDFQina Nugroho, pts.100% (1)
- Occupational Therapy: Skills For LivingDokument14 SeitenOccupational Therapy: Skills For Livingkalik67% (3)
- Principles and Practice of Child Neurology in Infancy, 2nd EditionVon EverandPrinciples and Practice of Child Neurology in Infancy, 2nd EditionColin KennedyNoch keine Bewertungen
- Bayley ScalesDokument7 SeitenBayley Scalesmrabhilekh100% (1)
- Newborn AssessmentDokument15 SeitenNewborn Assessmentmarie97% (35)
- DSC BookDokument52 SeitenDSC BookPriti Khemka60% (5)
- Pediatric AssessmentDokument5 SeitenPediatric AssessmentmitchNoch keine Bewertungen
- Pediatric Treatment PlanDokument11 SeitenPediatric Treatment PlanKayla Jensen100% (1)
- Study TipsDokument2 SeitenStudy Tipsapi-405162391Noch keine Bewertungen
- Occupational Therapy Toolbox Study GuideDokument44 SeitenOccupational Therapy Toolbox Study GuideKristian ShumateNoch keine Bewertungen
- Pediatric Evaluation of Disability Inventory SUMMARYDokument4 SeitenPediatric Evaluation of Disability Inventory SUMMARYFaye ValensoyNoch keine Bewertungen
- Physical Therapy Initial EvaluationDokument3 SeitenPhysical Therapy Initial EvaluationkhushmitNoch keine Bewertungen
- OT Theories (In A Nutshell)Dokument8 SeitenOT Theories (In A Nutshell)TaraJane House100% (1)
- Pediatric History TakingDokument7 SeitenPediatric History TakingBet Bagares100% (2)
- The Short Textbook of Pediatrics PDFDokument38 SeitenThe Short Textbook of Pediatrics PDFGolla manoharNoch keine Bewertungen
- Ot Goals NuevoDokument157 SeitenOt Goals NuevoElbania PerezNoch keine Bewertungen
- English in Paediatrics 1: Textbook for Mothers, Caregivers, Nurses and PaediatriciansVon EverandEnglish in Paediatrics 1: Textbook for Mothers, Caregivers, Nurses and PaediatriciansBewertung: 5 von 5 Sternen5/5 (1)
- Pediatric Evaluation ReportDokument3 SeitenPediatric Evaluation Reportapi-469965619Noch keine Bewertungen
- IEEDokument3 SeitenIEEMickaela PangilinanNoch keine Bewertungen
- Developmental Profile by AgeDokument3 SeitenDevelopmental Profile by AgeJc Saballegue100% (1)
- Bayley-III Clinical Use and InterpretationVon EverandBayley-III Clinical Use and InterpretationBewertung: 2 von 5 Sternen2/5 (1)
- Senior Occupational Therapist: Passbooks Study GuideVon EverandSenior Occupational Therapist: Passbooks Study GuideNoch keine Bewertungen
- GMFMscoresheetDokument6 SeitenGMFMscoresheetAbdur RasyidNoch keine Bewertungen
- PEDI CAT Manual 1 3 6 PDFDokument162 SeitenPEDI CAT Manual 1 3 6 PDFSari Nm100% (2)
- Occupational Therapy Manual For The EASA ModelDokument48 SeitenOccupational Therapy Manual For The EASA Modellolocy L100% (2)
- NBCOT Ques From Facebook 2012/2013Dokument52 SeitenNBCOT Ques From Facebook 2012/2013Magaloo Shmuloo100% (1)
- Developmental MilestonesDokument30 SeitenDevelopmental MilestonesSana Bushra100% (5)
- A Handbook of Pediatric Terms With Simple Non-technical Definitions: WordsRUs Pediatric Dictionaries, #1Von EverandA Handbook of Pediatric Terms With Simple Non-technical Definitions: WordsRUs Pediatric Dictionaries, #1Noch keine Bewertungen
- An Evidence Based Occupational Therapy Toolkit For Assessment and Treatment of The Upper Extremity Post StrokeDokument63 SeitenAn Evidence Based Occupational Therapy Toolkit For Assessment and Treatment of The Upper Extremity Post StrokeYaltiNoch keine Bewertungen
- OTR ReviewDokument64 SeitenOTR Reviewkjykiki1986100% (6)
- VMIpdfDokument6 SeitenVMIpdfRidwan HadiputraNoch keine Bewertungen
- Rheumatology Practice in Occupational Therapy: Promoting Lifestyle ManagementVon EverandRheumatology Practice in Occupational Therapy: Promoting Lifestyle ManagementLynne GoodacreNoch keine Bewertungen
- Newborn and Pediatrics History and PeDokument12 SeitenNewborn and Pediatrics History and PeShauneeNoch keine Bewertungen
- COTA NBCOT ReviewDokument128 SeitenCOTA NBCOT ReviewDen Ise100% (4)
- Category Ot Goals.Dokument11 SeitenCategory Ot Goals.adelitaperez100% (3)
- HemiplegiaDokument5 SeitenHemiplegiaRyan TOgzNoch keine Bewertungen
- Pediatric History & Physical ExamDokument5 SeitenPediatric History & Physical ExamLloyd Jay Lin100% (1)
- 6min English Kids at Home PDFDokument5 Seiten6min English Kids at Home PDFJim Jose AntonyNoch keine Bewertungen
- Common Cutaneous Infections and InfestationsDokument28 SeitenCommon Cutaneous Infections and InfestationsJim Jose AntonyNoch keine Bewertungen
- 6min English Electricity PDFDokument5 Seiten6min English Electricity PDFJim Jose AntonyNoch keine Bewertungen
- India Today 29 June 2020 PDFDokument76 SeitenIndia Today 29 June 2020 PDFJim Jose AntonyNoch keine Bewertungen
- Immunization in Children: Fahad Al ZamilDokument44 SeitenImmunization in Children: Fahad Al ZamilJim Jose AntonyNoch keine Bewertungen
- Dr. Elham Bukhari: Aediatri Nfectious IseaseDokument56 SeitenDr. Elham Bukhari: Aediatri Nfectious IseaseJim Jose AntonyNoch keine Bewertungen
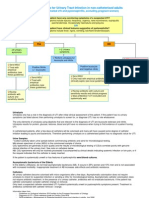
- Urinary Tract Infection in Children: Dr. Alia Al-Ibrahim Consultant Pediatric Nephrology Clinical Assistant ProfessorDokument11 SeitenUrinary Tract Infection in Children: Dr. Alia Al-Ibrahim Consultant Pediatric Nephrology Clinical Assistant ProfessorJim Jose AntonyNoch keine Bewertungen
- Acne Vulgaris and Acne Related DisordersDokument12 SeitenAcne Vulgaris and Acne Related DisordersJim Jose AntonyNoch keine Bewertungen
- Refractive ErrorsDokument7 SeitenRefractive ErrorsJim Jose AntonyNoch keine Bewertungen
- Strabismus, Amblyopia Management and LeukocoriaDokument19 SeitenStrabismus, Amblyopia Management and LeukocoriaJim Jose AntonyNoch keine Bewertungen
- Optha: NeuroDokument13 SeitenOptha: NeuroJim Jose AntonyNoch keine Bewertungen
- Ortho Team FinalDokument221 SeitenOrtho Team FinalJim Jose AntonyNoch keine Bewertungen
- Chronic Visual LossDokument7 SeitenChronic Visual LossJim Jose AntonyNoch keine Bewertungen
- Ocular EmergenciesDokument4 SeitenOcular EmergenciesJim Jose AntonyNoch keine Bewertungen
- Investigations of Lung DiseasesDokument14 SeitenInvestigations of Lung DiseasesJim Jose AntonyNoch keine Bewertungen
- GoutDokument1 SeiteGoutJim Jose AntonyNoch keine Bewertungen
- COPD and BronchiectasisDokument20 SeitenCOPD and BronchiectasisJim Jose AntonyNoch keine Bewertungen
- Acute Visual LossDokument10 SeitenAcute Visual LossJim Jose AntonyNoch keine Bewertungen
- Pleural EffusionDokument10 SeitenPleural EffusionJim Jose Antony100% (1)
- Hair Disorders and Pigmented Disorders of The SkinDokument8 SeitenHair Disorders and Pigmented Disorders of The SkinJim Jose AntonyNoch keine Bewertungen
- SampleH&P PDFDokument6 SeitenSampleH&P PDFJim Jose AntonyNoch keine Bewertungen
- Diagnostic Criteria For Urinary Tract InfectionDokument2 SeitenDiagnostic Criteria For Urinary Tract InfectioncandyslibioNoch keine Bewertungen
- Cardiology Disease List PDFDokument139 SeitenCardiology Disease List PDFJim Jose AntonyNoch keine Bewertungen
- Medicine Annotated Multiple ChoiceDokument20 SeitenMedicine Annotated Multiple ChoiceJim Jose AntonyNoch keine Bewertungen
- Motor and Sensory Examination: Dr. Bandar Al Jafen, MD Consultant NeurologistDokument36 SeitenMotor and Sensory Examination: Dr. Bandar Al Jafen, MD Consultant NeurologistJim Jose Antony100% (1)
- Orthopedic History Taking: DR - Kholoud Al-ZainDokument30 SeitenOrthopedic History Taking: DR - Kholoud Al-ZainJim Jose AntonyNoch keine Bewertungen
- MCQ Questions May 2006Dokument10 SeitenMCQ Questions May 2006Jim Jose AntonyNoch keine Bewertungen
- Anatomy of The Nose Nasopharynx and Paranasal Sinuses PDFDokument7 SeitenAnatomy of The Nose Nasopharynx and Paranasal Sinuses PDFJim Jose AntonyNoch keine Bewertungen
- Paranasal SinusesDokument7 SeitenParanasal SinusesJim Jose AntonyNoch keine Bewertungen
- Hypertrophic ScarsDokument13 SeitenHypertrophic ScarsNovita NingtyasNoch keine Bewertungen
- Measles Case FormDokument3 SeitenMeasles Case FormVlad BăhneanuNoch keine Bewertungen
- Healing Parvo PuppiesDokument11 SeitenHealing Parvo PuppiesAshen WillowsNoch keine Bewertungen
- Asbestos Awareness Quiz #1: AnswersDokument2 SeitenAsbestos Awareness Quiz #1: AnswersMichael NcubeNoch keine Bewertungen
- DR Upul Pathirana: Endo-Bronchial Ultrasound & Trans-Bronchial Needle AspirationDokument26 SeitenDR Upul Pathirana: Endo-Bronchial Ultrasound & Trans-Bronchial Needle AspirationUpul PathiranaNoch keine Bewertungen
- Cardiovascular Examination: Preparation of The PatientDokument4 SeitenCardiovascular Examination: Preparation of The PatientLolla SinwarNoch keine Bewertungen
- Comparison - of - ABAcard - p30 - and RSID - Semen - Test - Kits - For - Forensic - Semen - Identification PDFDokument5 SeitenComparison - of - ABAcard - p30 - and RSID - Semen - Test - Kits - For - Forensic - Semen - Identification PDFEdward Arthur IskandarNoch keine Bewertungen
- Drug Study Magnesium SulfateDokument3 SeitenDrug Study Magnesium SulfateSchyna Marielle VitaleNoch keine Bewertungen
- Screenshot 2022-10-21 at 19.56.24Dokument3 SeitenScreenshot 2022-10-21 at 19.56.24Zafira AkramNoch keine Bewertungen
- 10 Jurnal Tentang Judul Penerapan Nafas Dalam Post Op Apendisitis Sulhan Wira DutaDokument98 Seiten10 Jurnal Tentang Judul Penerapan Nafas Dalam Post Op Apendisitis Sulhan Wira DutaSultan Wira DutaNoch keine Bewertungen
- Cardiovascular Dynamics PhysiolabDokument55 SeitenCardiovascular Dynamics PhysiolabJaninepacia100% (1)
- ASTHMADokument48 SeitenASTHMAifcrstarsNoch keine Bewertungen
- Immobilization and Death of Bacteria by Flora Seal Microbial SealantDokument6 SeitenImmobilization and Death of Bacteria by Flora Seal Microbial SealantinventionjournalsNoch keine Bewertungen
- I. Objectives: GeneralDokument36 SeitenI. Objectives: GeneralSharlaine CabanayanNoch keine Bewertungen
- Obstetrics by Ten Teachers, 20th Edition 2017Dokument33 SeitenObstetrics by Ten Teachers, 20th Edition 2017salah subbah100% (1)
- Dsfasdfsadf PDFDokument246 SeitenDsfasdfsadf PDFrpascua123Noch keine Bewertungen
- AW32150 - 30 - Surgical Guideline SYNCHRONY PIN - EN English - WebDokument64 SeitenAW32150 - 30 - Surgical Guideline SYNCHRONY PIN - EN English - WebLong An DoNoch keine Bewertungen
- The Adhesive Bridge Inlay Retained in The TherapyDokument3 SeitenThe Adhesive Bridge Inlay Retained in The TherapyLekic JelenaNoch keine Bewertungen
- Assessment Cover Sheet: Student To Complete Please Read The Below CarefullyDokument25 SeitenAssessment Cover Sheet: Student To Complete Please Read The Below CarefullyNoreen Punjwani100% (1)
- Quality Form Oplan Kalusugan Sa Deped Accomplishment Report FormDokument11 SeitenQuality Form Oplan Kalusugan Sa Deped Accomplishment Report Formchris orlanNoch keine Bewertungen
- English For HealthDokument97 SeitenEnglish For HealthRahmat Bagus Setya BudiNoch keine Bewertungen
- KERATOSIS AND RELATED DISORDERS OF ORAL MUCOSA (2) Edited JsmuDokument126 SeitenKERATOSIS AND RELATED DISORDERS OF ORAL MUCOSA (2) Edited JsmuMINI DHABANoch keine Bewertungen
- Management of Chest TubeDokument22 SeitenManagement of Chest TubeFatima Hafza SahiddinNoch keine Bewertungen
- Full Download Book Medical Epigenetics PDFDokument41 SeitenFull Download Book Medical Epigenetics PDFandrew.lindsey981100% (14)
- Fracture of The Upper HumerusDokument22 SeitenFracture of The Upper HumerusOlasinde AnthonyNoch keine Bewertungen
- Hemato OnologyDokument60 SeitenHemato OnologyGousayAlkhazmariNoch keine Bewertungen
- Endocrine DisordersDokument106 SeitenEndocrine DisordersMansur MuhammadNoch keine Bewertungen
- 1 CervixDokument12 Seiten1 Cervixzianab aliNoch keine Bewertungen
- Blood and Marrow Transplant Quality Management PlanDokument47 SeitenBlood and Marrow Transplant Quality Management PlansumathiNoch keine Bewertungen
- FULL Download Ebook PDF International Trauma Life Support For Emergency Care Providers 9th Edition PDF EbookDokument51 SeitenFULL Download Ebook PDF International Trauma Life Support For Emergency Care Providers 9th Edition PDF Ebookcarl.helbling11893% (42)