Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Slides - Issues and Perspectives Health Policy - Master HealthDokument42 SeitenSlides - Issues and Perspectives Health Policy - Master HealthSourav SarkarNoch keine Bewertungen
- Konnichi Yawa Sa Mock Review Ictmpart1Dokument8 SeitenKonnichi Yawa Sa Mock Review Ictmpart1Wansun MaglangitNoch keine Bewertungen
- The Cardiac & Vascular Institute Recognized For Quality Laboratory ServicesDokument2 SeitenThe Cardiac & Vascular Institute Recognized For Quality Laboratory ServicesPR.comNoch keine Bewertungen
- Mortality and Morbidity CHNDokument19 SeitenMortality and Morbidity CHNPamela Ria HensonNoch keine Bewertungen
- 8030-Article Text-18786-1-10-20191106Dokument9 Seiten8030-Article Text-18786-1-10-20191106Bernadina AlfionitaNoch keine Bewertungen
- Lab Med Quality IndicatorsDokument15 SeitenLab Med Quality IndicatorsMelani Sinasri RenagupitaNoch keine Bewertungen
- 5th Topic Future Direction For Client Education 1Dokument31 Seiten5th Topic Future Direction For Client Education 1lykajoypangilinan14Noch keine Bewertungen
- Advantages and Disadvantages of Free HealthcareDokument1 SeiteAdvantages and Disadvantages of Free HealthcareJames DayritNoch keine Bewertungen
- 2019-20 Osh Training CalenderDokument2 Seiten2019-20 Osh Training Calenderchapisha incNoch keine Bewertungen
- Care Supreme - BrochureDokument4 SeitenCare Supreme - BrochureVivek HamseNoch keine Bewertungen
- Final-Bdnc - Peran Tenaga Gizi Dalam Era TransformasiDokument43 SeitenFinal-Bdnc - Peran Tenaga Gizi Dalam Era TransformasiLisa FarhatusNoch keine Bewertungen
- Dimensi Budaya Keselamatan Pasien: Dimension of Patient Safety CultureDokument9 SeitenDimensi Budaya Keselamatan Pasien: Dimension of Patient Safety CultureBendito KedatiNoch keine Bewertungen
- Antenatal CareDokument14 SeitenAntenatal CareJustine NyangaresiNoch keine Bewertungen
- Chapter-PSQ PSQ 1Dokument6 SeitenChapter-PSQ PSQ 1balaji srinivasanNoch keine Bewertungen
- PhilHealth Circular No. 011-2015 OHAT PackageDokument12 SeitenPhilHealth Circular No. 011-2015 OHAT Packagerommel mendozaNoch keine Bewertungen
- Virtual Care Discussion PaperDokument24 SeitenVirtual Care Discussion Papere.K.e.kNoch keine Bewertungen
- A Problem of Display Codes Case StudyDokument7 SeitenA Problem of Display Codes Case StudyJam EsNoch keine Bewertungen
- 2003 Davies Primary Care Award Cooper Pediatrics Matt MabalotDokument10 Seiten2003 Davies Primary Care Award Cooper Pediatrics Matt Mabalotapi-237901402Noch keine Bewertungen
- IntroductionDokument2 SeitenIntroductionlaoy aolNoch keine Bewertungen
- ANC Guidelines - 18 July 2022 - Final-3 (6942)Dokument238 SeitenANC Guidelines - 18 July 2022 - Final-3 (6942)Sara YehiaNoch keine Bewertungen
- Bahasa Inggris (Community Mental Health Nursing)Dokument16 SeitenBahasa Inggris (Community Mental Health Nursing)Dinda AyundaNoch keine Bewertungen
- Executive Director Senior Center in Tallahassee FL Resume Rodney BigelowDokument2 SeitenExecutive Director Senior Center in Tallahassee FL Resume Rodney BigelowRodneyBigelowNoch keine Bewertungen
- Private Health FacilitiesDokument1 SeitePrivate Health FacilitiesSeriel TismoNoch keine Bewertungen
- Philhealth PPT-1Dokument23 SeitenPhilhealth PPT-1Beatrice BagaoisanNoch keine Bewertungen
- AMCP Pharmaceutical Guide FinalDokument90 SeitenAMCP Pharmaceutical Guide FinalRELNSTNoch keine Bewertungen
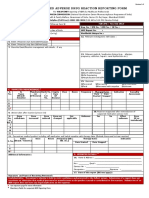
- ADRnewReporting Form 1.4Dokument2 SeitenADRnewReporting Form 1.4Sourabh kundara0% (1)
- Articles: BackgroundDokument15 SeitenArticles: BackgroundMarcus Wong KSNoch keine Bewertungen
- Final MCO Working Group ReportDokument77 SeitenFinal MCO Working Group ReportShira SchoenbergNoch keine Bewertungen
- Resources For Medication Safety Lecture - ViswanathanDokument59 SeitenResources For Medication Safety Lecture - Viswanathanapi-669020994Noch keine Bewertungen
- Basic Medical Billing and Imp Questions.Dokument16 SeitenBasic Medical Billing and Imp Questions.Koppolu SatyaNoch keine Bewertungen