Beruflich Dokumente
Kultur Dokumente
Ass Resp RT Prost CA DWI 3T
Hochgeladen von
Ido N. BramantyaCopyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
Ass Resp RT Prost CA DWI 3T
Hochgeladen von
Ido N. BramantyaCopyright:
Verfügbare Formate
Genitourinar y Imaging Original Research
Song et al.
DWI to Assess Radiotherapy-Treated Prostate Cancer
Genitourinary Imaging
Original Research
Assessment of Response to
Downloaded from www.ajronline.org by 103.213.131.210 on 07/07/17 from IP address 103.213.131.210. Copyright ARRS. For personal use only; all rights reserved
Radiotherapy for Prostate
FOCUS ON:
Cancer: Value of Diffusion-
Weighted MRI at 3 T
Inyoung Song1 OBJECTIVE. The objective of our study was to investigate the changes of apparent dif-
Chan Kyo Kim1 fusion coefficient (ADC) values in prostate cancers before and after radiotherapy at 3 T us-
Byung Kwan Park1 ing a phased-array coil.
Won Park 2 MATERIALS AND METHODS. Forty-nine patients with biopsy-proven prostate can-
cer who received radiotherapy underwent diffusion-weighted imaging (DWI) at 3 T and were
Song I, Kim CK, Park BK, Park W included in the study. Biopsies in all patients were performed before the initial MRI exami-
nation (range, 1535 days before MRI; mean, 23.4 days). All 49 patients underwent DWI (b
values = 0 and 1,000 s/mm2) before and 15 months after the completion of radiotherapy. The
changes in ADC values were measured for cancers and benign tissues before and after thera-
py. Additionally, the changes in serum prostate-specific antigen (PSA) levels were evaluated
before and after therapy.
RESULTS. A total of 57 cancers (peripheral zone, n = 45; transition zone, n = 12) were
found in 46 patients. For the tumors, the mean ADC value after therapy (1.61 10 3 mm2 /s)
was increased compared with the mean ADC value before therapy (1.0 10 3 mm2 /s) (p <
0.001). After radiotherapy, the mean ADC values of benign peripheral zones and of benign
transition zones were statistically significantly decreased compared with those before radio-
therapy (p < 0.05). Before treatment, a significant difference of ADC values between the tu-
mors and benign tissues was found (p < 0.001), whereas there was no significant difference of
ADC values between them after treatment (p > 0.1). The median PSA level after therapy (0.49
ng/mL) was decreased compared with the median PSA level before therapy (20.0 ng/mL).
CONCLUSION. With the use of a 3-T MR scanner, our preliminary results suggest that
ADC values may be useful as an imaging biomarker for monitoring therapeutic response of
Keywords: 3-T MRI, apparent diffusion coefficient, prostate cancer to radiotherapy.
diffusion-weighted imaging, MRI, prostate cancer,
radiotherapy
D
etermination of the serum pros- in those with the most optimal biochemical
DOI:10.2214/AJR.09.3557 tate-specific antigen (PSA) level response. In addition, the most appropriate
has been widely used for screen- biochemical definitions of treatment failure
Received August 31, 2009; accepted after revision
ing, diagnosis, determination of after radiotherapy remain controversial be-
December 7, 2009.
prognosis, and selection of the appropriate cause of substantial differences in the diag-
1
Department of Radiology and Center for Imaging treatment for men with clinically localized nostic accuracies of biochemical levels for
Science, Samsung Medical Center, Sungkyunkwan prostate cancer [14]. Radiotherapy for pros- predicting clinical outcome. Moreover, no
University School of Medicine, 50 Ilwon-dong, tate cancer is currently one of the common pattern of PSA kinetics after radiotherapy
Kangnam-gu, Seoul 135-710, Republic of Korea. Address
correspondence to C. K. Kim (chankyokim@skku.edu).
treatment strategies if the cancer is detected has conclusively differentiated between local
at an early stage and invasive surgical resec- and distant failure [79]. To the contrary, a
2
Department of Radiation and Oncology, Samsung tion can be avoided [5, 6]. After radiothera- functional MR technique such as diffusion-
Medical Center, Sungkyunkwan University School of py, monitoring PSA levels is used to deter- weighted imaging (DWI) may detect and lo-
Medicine, Seoul, Republic of Korea.
mine the effectiveness of treatment as an calize prostate cancer before radiotherapy
WEB early and accurate surrogate. However, PSA and then may provide qualitative or quantita-
This is a Web exclusive article. monitoring has been shown to have a limited tive information for measuring therapeutic
role in defining cancer cure within the first 5 response in patients with prostate cancer
AJR 2010; 194:W477W482 years after radiotherapy because, although a during and after radiotherapy.
0361803X/10/1946W477
lower PSA nadir after radiotherapy has been With the introduction of higher-field-strength
associated with cancer cure, the treatment MR scanners and the parallel imaging tech-
American Roentgen Ray Society ultimately fails in 525% of patientseven nique for prostate MRI, DWI has been shown
AJR:194, June 2010 W477
Song et al.
TABLE 1: Distributions of Gleason All patients underwent a transrectal sonogra- size, 0.35 0.59 3 mm; slice number, 20; and ac-
Scores in 49 Patients phyguided biopsy within 5 weeks before radio- quisition time of each plane, 4 minutes 22 seconds.
Gleason Score No. of Patients (n = 49) therapy. Biopsies in all patients were performed DW images were acquired in the axial plane
before the initial MRI examination (range, 1535 using the single-shot echo-planar imaging tech-
4 3
days; mean, 23.4 days). The median Gleason score nique. The scanning parameters were as follows:
5 0 before therapy was 7 (range, 410). Table 1 pres- 2,7402,750/8385; slice thickness, 3 mm; inter-
Downloaded from www.ajronline.org by 103.213.131.210 on 07/07/17 from IP address 103.213.131.210. Copyright ARRS. For personal use only; all rights reserved
6 10 ents the distributions of Gleason scores. All MR slice gap, 1 mm; matrix, 112 110; FOV, 20 cm;
7 20 scans were obtained before the start of radiother- SENSE factor, 2; and NSA, 3. Diffusion-encoding
apy and 15 months (mean, 3.5 months) after the gradients were applied as a bipolar pair at b val-
8 11
completion of therapy. Twenty-seven patients re- ues of 0 and 1,000 s/mm 2 along the three orthogo-
9 3 ceived simultaneous hormone therapy. nal directions of motion-probing gradients. ADC
10 2 Clinical response was determined from mea- maps were automatically constructed on a pixel-
surements of serum PSA levels. The mean serum by-pixel basis (0 and 1,000 s/mm 2). The acquisi-
to have several potential benefits for the as- PSA level was 42.5 ng/mL (range, 4.25456 ng/ tion time of DWI was within 2 minutes.
sessment of tumor localization and staging. In mL) before biopsy and 0.87 ng/mL (range, 0.34
comparison with the use of conventional MRI, 1.4 ng/mL) after the completion of radiotherapy. Data Analysis and ADC Measurement
DWI can noninvasively show the changes of All images were retrospectively analyzed in
cellularity in malignant tumors in the body; MR Techniques consensus by two genitourinary radiologists with
apparent diffusion coefficient (ADC) maps All images were collected using a 3-T MR sys- 6 and 3 years of experience, respectively, who were
can show the mobility of water in tissues. tem (Intera Achieva, Philips Healthcare) equipped aware of the clinical and histologic findings. Each
After the treatment of malignant tumors, with a phased-array coil (six-channel). All patients reader had completed a genitourinary fellowship
the cellularity and cell membrane integrity in underwent DWI in addition to imaging studies us- and had interpreted more than 700 MR examina-
necrotic tumor cells are reduced and there is a ing a routine prostatic MR protocol. Before un- tions of the prostate at the time of the study.
subsequent increase in water mobility, where- dergoing scanning, each patient received an intra- The localization of prostate cancer was deter-
as viable tumor cells restrict diffusion of wa- muscular injection of 20 mg of butyl scopolamine mined by consensus of the two readers based on a
ter molecules. To date, several clinical studies (Buscopan, Boehringer Ingelheim) to suppress comparison of digital rectal examination findings,
on the usefulness of DWI as a measurement bowel peristalsis; no bowel preparation was per- the pathologic results of biopsies, and the presence
of treatment response have been reported [10 formed. T2-weighted turbo spin-echo images were of a focal low-signal-intensity area in the periph-
13]. For the evaluation of changes of ADC acquired in three orthogonal planes (axial, sagittal, eral zone and transition zone on ADC maps with
values after radiotherapy in localized prostate and coronal). The T2-weighted imaging parame- or without the use of T2-weighted images. ADC
cancer, to our knowledge, few investigations ters were as follows: TR range/TE range, 2,690 maps were processed using workstation software
have been reported [14]. Therefore, the pur- 3,800/8090; slice thickness, 3 mm; interslice (PRIDE tool, Philips Healthcare). With the use of
pose of this study was retrospectively to in- gap, 0.31 mm; 512 304 matrix; field of view MRIcro software (version 1.37, Rorden and Brett,
vestigate the changes of ADC values in pros- (FOV), 18 cm; number of signals acquired (NSA), 2000), ADC values in tumors and in the peripher-
tate cancers before and after radiotherapy at 3; sensitivity-encoding (SENSE) factor, 2; voxel al zone and transition zone of benign tissue before
3 T using a phased-array coil.
Materials and Methods
Patients
The ethics committee of our institute approved
this study. Written informed consent was waived
because of the retrospective nature of the analysis.
Between January 2006 and May 2008, 49 patients
with biopsy-proven prostate cancer underwent ex-
ternal beam radiotherapy and MR examinations at
3 T before and after radiotherapy in our hospital.
The median patient age was 67.5 years (age range,
4281 years).
Radiotherapy was administered at 2 Gy/fraction
to a total dose of 6674 Gy (median dose, 70 Gy)
with the use of a 15-MV linear accelerator. Thir-
ty-nine patients were treated with the use of 3D A B
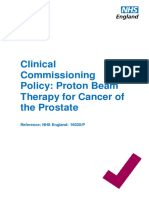
conformal radiotherapy to the prostate only or to Fig. 1On axial apparent diffusion coefficient (ADC) maps (TR/TE, 2,749/84; matrix, 112 110; b = 0 and
the prostate and seminal vesicles. In 10 patients, a 1,000 s/mm2), method of ADC value measurement using region of interest (ROI) in tumor (arrow) and benign
whole-pelvis irradiation dose of 46 Gy was admin- peripheral zone (arrowhead) is shown.
istered, and an additional 2028 Gy was adminis- A and B, ROI was drawn on left lobe of midgland before (A) and after (B) radiotherapy. Mean ADC of tumor
increased from 0.89 10 3 mm2 /s before radiotherapy to 1.48 10 3 mm2 /s after radiotherapy. Note ROI in
tered to the prostate only or to the prostate and sem- benign peripheral zone of right lobe. Mean ADC value of benign peripheral zone decreased from 1.82 10 3
inal vesicles using a cone-down boost technique. mm2 /s before therapy to 1.63 10 3 mm2 /s after radiotherapy.
W478 AJR:194, June 2010
DWI to Assess Radiotherapy-Treated Prostate Cancer
TABLE 2: Results of Mean Apparent Diffusion Coefficient (ADC) Values of 57
Tumors in 46 Patients and Benign Tissues in 49 Patients Before and 2.6
After Radiotherapy
2.4
ADC Value 10 3 mm2 /s, mean SD (range)
2.2
Time of ADC Measurement Tumors Benign Tissues
Downloaded from www.ajronline.org by 103.213.131.210 on 07/07/17 from IP address 103.213.131.210. Copyright ARRS. For personal use only; all rights reserved
2.0
Before radiotherapy
ADC ( 103 mm2/s)
Overall 1.00 0.19 (0.731.58)a 1.8
Peripheral zone 1.03 0.20 (0.771.58)a 2.05 2.07 (1.582.72)b 1.6
Transition zone 0.88 0.13 (0.73,1.08)a 1.72 0.24 (1.242.27)b 1.4
After radiotherapy
1.2
Overall 1.61 0.27 (0.892.46)
1.0
Peripheral zone 1.62 0.29 (0.892.47) 1.77 0.27 (1.352.48)
0.8
Transition zone 1.57 0.18 (1.311.91) 1.59 0.23 (1.222.33)
aComparison of the mean ADC values of tumors before and after radiotherapy, p < 0.001. 0.6
bComparison of the mean ADC values of benign tissues before and after radiotherapy, p < 0.05.
Before After
Radiotherapy Radiotherapy
and after radiotherapy were calculated by place- for benign tissue (range, 1743 mm 2). After radio-
Fig. 2Graph of change in apparent diffusion
ment of regions of interest (ROIs) (Fig. 1). When therapy, the mean ROIs were 97.4 mm2 for tumors coefficient (ADC) values in 57 prostate cancers
the ROIs were drawn, great care was taken to ex- (range, 10404 mm 2) and 22 mm 2 for benign tis- after radiotherapy. These data show statistically
clude both the neurovascular bundle and the ure- sue (range, 1432 mm 2). significant increase in ADC values in all cases except
two cases because of increased water diffusion after
thra to reduce any error in ADC calculations.
radiotherapy.
Before radiotherapy, ROIs of the tumors in the Statistical Analysis
peripheral zone and transition zone were drawn Statistical analysis was performed using SAS
on ADC maps to include as much of the tumor software (version 8, SAS Institute). The paired The mean ADC value of those tumors was
as possible. ADC values in tumors were assessed Students t test was used to compare the ADC val- 1.08 10 3 mm2 /s.
twice in the same site, and the average was calcu- ues of tumors and benign tissues before and after Of the four patients with residual tumors,
lated. If a tumor was located in several imaging radiotherapy and to compare the mean PSA lev- follow-up ADC maps obtained 7 months af-
slices of ADC maps, ADC values were measured els before and after radiotherapy. The comparison ter the completion of radiotherapy showed
on each image of the ADC maps and the average of mean ADC values of tumors and benign tis- that residual tumor had disappeared in two
was calculated. Tumors with a transverse greatest sues before radiotherapy was performed using the patients; however, in the other two patients
diameter of more than 0.5 cm were included to re- paired Students t test. A correlation in the degree who had one tumor each, the mean ADC val-
duce false-positive findings. High-resolution T2- of change between serum PSA levels and ADC ue did not increase after radiotherapy. There
weighted images corresponding to the ADC maps values was performed by use of Pearsons correla- was no change in one patient (from 0.96
were observed in the transverse orientation to as- tion. Two-tailed tests were used to calculate all p 10 3 before therapy to 0.96 10 3 mm2 /s af-
sist in the identification of the detailed anatomy values. A p value of < 0.05 was considered statis- ter therapy) and a decrease in the other pa-
of the prostate. For measurement of ADC values tically significant. tient (from 1.04 to 0.89 10 3 mm2 /s) (Figs.
in the peripheral zone and transition zone of be- 2 and 3). These two patients showed a de-
nign tissue, ROIs at the contralateral side of the Results crease in PSA level (from 21.12 ng/mL be-
tumor were selected. In three different sites of be- In 46 of 49 patients, 57 cancers (peripher- fore therapy to 3.2 ng/mL after therapy and
nign tissue, ADC values were measured and the al zone, n = 45; transition zone, n = 12) were from 16.62 ng/mL before therapy to 12.09
average was calculated. found; in the remaining three patients, all of ng/mL after therapy, respectively) and a con-
After the completion of radiotherapy, there was whom had a Gleason score of 4, no focal mass siderable rise in PSA level after the comple-
no visible residual tumor in most cases, particular- was seen on ADC maps. On the ADC maps tion of radiotherapy.
ly for patients with a good response. In this situa- obtained before therapy, the mean size of the Before radiotherapy, the mean ADC val-
tion, the ROI was drawn on what was considered tumors was 2.2 cm (range, 0.83.2 cm). ues of tumors in both the peripheral zone
the normal residual prostate by two radiologists In 57 tumors of 46 patients, the mean and transition zone were statistically lower
in consensus; usually the ROI was drawn in the ADC value before therapy was 1.0 10 3 than the corresponding values of benign tis-
same area as that initially used in the pretherapy mm2 /s, which is significantly lower than the sues (p < 0.001). After radiotherapy, a sig-
MR examination. ROIs were assessed twice in the mean ADC value after therapy (1.61 10 3 nificant difference of ADC values between
same site, and the average was calculated. For be- mm2 /s) (p < 0.001) (Table 2). After the com- the tumors and benign tissues was not found
nign tissues, the ROIs were drawn on the same pletion of radiotherapy, there was no visible (p > 0.1) (Table 2). The mean ADC values of
area that was initially used in preradiotherapy im- tumor in 42 patients. However, in the remain- the peripheral zone and transition zone of be-
ages, and the average was calculated. ing four patients who had one tumor each, nign tissue were statistically decreased com-
Before radiotherapy, the mean ROIs were 208 residual tumor was seen on ADC maps 15 pared with the corresponding values before
mm2 for tumors (range, 10979 mm 2) and 28 mm 2 months after the completion of radiotherapy. radiotherapy (p < 0.05).
AJR:194, June 2010 W479
Song et al.
1,000
100
Downloaded from www.ajronline.org by 103.213.131.210 on 07/07/17 from IP address 103.213.131.210. Copyright ARRS. For personal use only; all rights reserved
10
PSA (ng/mL)
1
0.1
0.01
A B
0.001
Before After
Radiotherapy Radiotherapy
Fig. 4Graph of change in serum prostate-specific
antigen (PSA) levels in 49 patients with prostate
cancer after radiotherapy. These data show
statistically significant decrease in all cases after
radiotherapy.
tate cancer increased statistically in both the
peripheral zone and transition zone after ra-
diotherapy. One potential explanation for this
change was that an increase of the ADC af-
ter radiotherapy might be correlated with cel-
lularity increases because of a decrease in
C D the size and number of neoplastic glands, al-
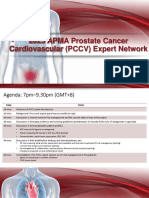
Fig. 363-year-old man with left-sided prostate cancer with extracapsular extension (prostate-specific though tumors might still exist [21]. The re-
antigen level: before radiotherapy, 16.62 ng/mL; after radiotherapy, 12.09 ng/mL). sults of our study for malignant tumors after
A and B, Before radiotherapy, axial T2-weighted fast spin-echo image (TR/TE, 3,680/80) (A) and apparent therapy were found to be equivalent to those
diffusion coefficient (ADC) map (2,749/84: matrix, 112 110; b = 0 and 1,000 s/mm2) (B) show prostate cancer
of previous studies for other malignant tu-
(arrows) of low signal intensity in left lobe. Mean ADC value of cancer was 1.04 10 3 mm2 /s.
C, After radiotherapy, axial T2-weighted fast spin-echo image (3,680/80) shows diffusely ill-defined area of low mors after treatment such as hepatocellular
signal intensity in both lobes. This finding is indeterminate for assessing residual cancer. carcinomas [22], rectal cancers [12], brain
D, After radiotherapy, axial ADC map (2,749/84: matrix, 112 110; b = 0 and 1,000 s/mm2) shows residual cancer tumors [10, 11], and breast cancers [13].
(arrows) of low signal intensity in left lobe. Mean ADC value of residual cancer was 0.89 10 3 mm2 /s. This
finding suggests poor response for treatment. Compared with the use of 1.5 T, the use
of 3 T has several advantages [23]. Theo-
Figure 4 shows the changes in PSA lev- in ADC values are inversely correlated with retically, the signal-to-noise ratio (SNR) in-
els before and after radiotherapy. The medi- changes in cellularity: Increases in ADC creased twofold on moving from 1.5 to 3 T,
an PSA level before therapy was 20.0 ng/mL, values reflect an increase in the mobility of and an increased SNR can be translated into
which is significantly higher than the median water through a decrease in cellular size or improvements in spatial, temporal, and spec-
PSA level after therapy of 0.49 ng/mL (p < number, and decreases in ADC values reflect tral resolution. A limited SNR at 1.5 T may
0.001). A correlation in the degree of chang- a decrease in free extracellular water by an impair MR sensitivity for subtle changes in
es between the PSA levels and ADC values increase of total cellular size or number, as ADC values of the prostate. The increase in
was not found (p > 0.05). can be seen with tumor progression, fibrosis, SNR from 3-T imaging enables either an in-
or edema [15, 20]. crease in spatial resolution or an increase in
Discussion Takayama et al. [14] recently reported that the SNR of the ADC maps, so a possible in-
DWI as a functional imaging technique ADC values of prostate cancer significant- crease in the accuracy of MRI for prostate
can measure the mobility of water within ly increased after radiotherapy. In our study, cancer localization and of the measurements
tissues in addition to depicting tumor size DWI performed at 3 T with a phased-array of ADC values in prostate cancers using
and shape [15]. To date, several studies have coil was used to evaluate the changes of ADC ROIs may be expected. Therefore, we think
shown that the ADC values of prostate can- values of prostate cancer before and after ra- that the potential measurement error for tu-
cer are lower than the ADC values of be- diotherapy. As in the previous study [14], our mor ADC values at 3 T might be lower than
nign noncancerous tissue [1619]. Changes results showed that the ADC values of pros- that at 1.5 T.
W480 AJR:194, June 2010
DWI to Assess Radiotherapy-Treated Prostate Cancer
In our study, after undergoing radiothera- tumors, DWI findings can reflect cellular surement of prostate-specific antigen in serum as
py of prostate cancer, all patients except two changes in malignant tissues earlier than 15 a screening test for prostate cancer. N Engl J Med
showed an increase in the mean ADC val- months after therapy, as early as 24 hours af- 1991; 324:11561161
ues of tumors in both the peripheral zone and ter treatment. For future studies, earlier and 3. Ito K, Yamamoto T, Ohi M, et al. Usefulness of
the transition zone. In the remaining two pa- more frequent examinations should be per- prostate-specific antigen velocity in screening for
tients, each of whom had one tumor, an in- formed during and after radiotherapy to as- prostate cancer. Int J Urol 2002; 9:316321
Downloaded from www.ajronline.org by 103.213.131.210 on 07/07/17 from IP address 103.213.131.210. Copyright ARRS. For personal use only; all rights reserved
crease in the ADC values was not shown: sess the dynamic changes of ADC values. 4. DAmico AV, Whittington R, Malkowicz SB, et
The ADC value of one tumor was slightly Second, all patients underwent a transrectal al. Biochemical outcome after radical prostatec-
decreased, and the ADC value of the remain- sonographyguided biopsy with the pretreat- tomy or external beam radiation therapy for pa-
ing tumor showed no change. As determined ment MR examinations, which might have tients with clinically localized prostate carcinoma
at subsequent follow-up of the two patients, affected the ADC values in benign pros- in the prostate specific antigen era. Cancer 2002;
local treatment had failed; the patients un- tate tissues due to hemorrhage or inflamma- 95:281286
derwent salvage high-intensity focused ultra- tory changes. Third, we could not evaluate 5. Albertsen PC, Hanley JA, Penson DF, Barrows G,
sound ablation. for any correlation between MR images and Fine J. 13-year outcomes following treatment for
As compared with a previous study [14] histopathologic findings because we did not clinically localized prostate cancer in a popula-
that showed no significant changes of ADC obtain surgical specimens. With the use of tion based cohort. J Urol 2007; 177:932936
values in benign prostate tissue after ra- a preclinical animal study, a detailed corre- 6. Gwede CK, Pow-Sang J, Seigne J, et al. Treatment
diotherapy, our results showed a statisti- lation between MR images and histopatho- decision-making strategies and influences in pa-
cally significant decrease in the ADC val- logic findings should be determined dur- tients with localized prostate carcinoma. Cancer
ues for the peripheral zone and transition ing or after radiotherapy. Fourth, this study 2005; 104:13811390
zone of benign noncancerous tissue. After was retrospective in design with the use of 7. Roach M 3rd, Hanks G, Thames H Jr, et al. Defin-
radiotherapy, benign prostate tissue might some different parameters such as TR and ing biochemical failure following radiotherapy
show histologic changes of acinar distortion TE. These differences in imaging parame- with or without hormonal therapy in men with
and atrophy as well as stromal fibrosis with ters might have affected ADC values of tu- clinically localized prostate cancer: recommen-
granulation tissue formation that may cause mor and benign prostate tissues. Finally, the dations of the RTOG-ASTRO Phoenix Consensus
a decrease of ADC values. Furthermore, a images in our study were interpreted by con- Conference. Int J Radiat Oncol Biol Phys 2006;
decrease of ADC values in benign prostate sensus of two readers instead of by separate 65:965974
tissue after radiotherapy might result from analyses. However, the aim of this study was 8. Kestin LL, Vicini FA, Martinez AA. Practical ap-
a decrease in the extracellular space due to not to evaluate the diagnostic performance plication of biochemical failure definitions: what
inflammatory swelling of cells associated for detecting localized cancer on DWI but to do and when to do it. Int J Radiat Oncol Biol
with radiotherapy. to determine ADC changes in prostate can- Phys 2002; 53:304315
Before radiotherapy, the ADC values of cer and normal prostate tissue before and af- 9. Vicini FA, Vargas C, Abner A, Kestin L, Horwitz
prostate cancer in our study were lower than ter radiotherapy using 3 T. Moreover, the in- E, Martinez A. Limitations in the use of serum
the corresponding values of noncancerous be- terreader agreement of MRI including DWI prostate specific antigen levels to monitor patients
nign prostate tissue, as described in previous is not perfect for the detection of localized after treatment for prostate cancer. J Urol 2005;
investigations [1719, 24]. Lower ADC values prostate cancer. Thus, the localization of 173:14561462
in prostate cancer reflect the restriction of wa- prostate cancer in this study was determined 10. Moffat BA, Chenevert TL, Lawrence TS, et al.
ter mobility due to the dense, high cellularity by consensus of two readers. Functional diffusion map: a noninvasive MRI bio-
of prostate cancer. Thus, prostate cancer pos- In conclusion, with the use of a 3-T MR marker for early stratification of clinical brain tu-
sibly showing a higher ADC value was auto- scanner, our preliminary results suggest that mor response. Proc Natl Acad Sci U S A 2005;
matically excluded from this study because ac- ADC values may be useful as an imaging bio- 102:55245529
curate localization of the cancer on ADC maps marker for monitoring therapeutic responses of 11. Hamstra DA, Chenevert TL, Moffat BA, et al.
was not possible. In three patients in our study prostate cancer to radiotherapy. However, larg- Evaluation of the functional diffusion map as an
who had Gleason score 4, the use of DWI er, more definitive studies with clinical end- early biomarker of time-to-progression and over-
could not delineate localized prostate cancer points such as early response assessment with- all survival in high-grade glioma. Proc Natl Acad
and ADC values could not be measured. in 7 days after the initiation of radiotherapy or Sci U S A 2005; 102:16,75916,764
In our study, the mean ROIs for tumors pretherapeutic prediction of biochemical fail- 12. DeVries AF, Kremser C, Hein PA, et al. Tumor
and benign tissue were different before and ure after radiotherapy should be performed. microcirculation and diffusion predict therapy
after radiotherapy. The reason is that the size outcome for primary rectal carcinoma. Int J Ra-
and volume of the prostate were markedly References diat Oncol Biol Phys 2003; 56:958965
decreased after radiotherapy as compared 1. Lawton CA, DeSilvio M, Roach M 3rd, et al. An 13. Pickles MD, Gibbs P, Lowry M, Turnbull LW.
with before radiotherapy. update of the phase III trial comparing whole pel- Diffusion changes precede size reduction in neo-
There are several limitations to this study. vic to prostate only radiotherapy and neoadjuvant adjuvant treatment of breast cancer. Magn Reson
First, we did not perform frequent follow- to adjuvant total androgen suppression: updated Imaging 2006; 24:843847
up MR examinations in all patients. Patients analysis of RTOG 94-13, with emphasis on unex- 14. Takayama Y, Kishimoto R, Hanaoka S, et al.
underwent MR examinations before radio- pected hormone/radiation interactions. Int J Ra- ADC value and diffusion tensor imaging of pros-
therapy and 15 months after radiotherapy. diat Oncol Biol Phys 2007; 69:646655 tate cancer: changes in carbon-ion radiotherapy. J
As shown in previous studies of other body 2. Catalona WJ, Smith DS, Ratliff TL, et al. Mea- Magn Reson Imaging 2008; 27:13311335
AJR:194, June 2010 W481
Song et al.
15. Hamstra DA, Rehemtulla A, Ross BD. Diffusion prostate cancer location at 3T using a phased-ar- 2007; 22:107118
magnetic resonance imaging: a biomarker for ray coil: preliminary results. Invest Radiol 2007; 22. Chen CY, Li CW, Kuo YT, et al. Early response of
treatment response in oncology. J Clin Oncol 42:842847 hepatocellular carcinoma to transcatheter arterial
2007; 25:41044109 19. Pickles MD, Gibbs P, Sreenivas M, Turnbull LW. chemoembolization: choline levels and MR diffu-
16. Kumar V, Jagannathan NR, Kumar R, et al. Cor- Diffusion-weighted imaging of normal and ma- sion constantsinitial experience. Radiology
relation between metabolite ratios and ADC val- lignant prostate tissue at 3.0T. J Magn Reson Im- 2006; 239:448456
Downloaded from www.ajronline.org by 103.213.131.210 on 07/07/17 from IP address 103.213.131.210. Copyright ARRS. For personal use only; all rights reserved
ues of prostate in men with increased PSA level. aging 2006; 23:130134 23. Kim CK, Park BK. Update of prostate magnetic
Magn Reson Imaging 2006; 24:541548 20. Armitage PA, Schwindack C, Bastin ME, Whittle resonance imaging at 3 T. J Comput Assist To-
17. Kim CK, Park BK, Han JJ, Kang TW, Lee HM. IR. Quantitative assessment of intracranial tumor mogr 2008; 32:163172
Diffusion-weighted imaging of the prostate at 3 T response to dexamethasone using diffusion, per- 24. Tamada T, Sone T, Jo Y, et al. Apparent diffusion
for differentiation of malignant and benign tissue fusion and permeability magnetic resonance im- coefficient values in peripheral and transition
in transition and peripheral zones: preliminary re- aging. Magn Reson Imaging 2007; 25:303310 zones of the prostate: comparison between nor-
sults. J Comput Assist Tomogr 2007; 31:449454 21. Petraki CD, Sfikas CP. Histopathological changes mal and malignant prostatic tissues and correla-
18. Kim CK, Park BK, Lee HM, Kwon GY. Value of induced by therapies in the benign prostate and tion with histologic grade. J Magn Reson Imaging
diffusion-weighted imaging for the prediction of prostate adenocarcinoma. Histol Histopathol 2008; 28:720726
W482 AJR:194, June 2010
Das könnte Ihnen auch gefallen
- A Clinically Relev Appr Imaging Prost CADokument10 SeitenA Clinically Relev Appr Imaging Prost CAIdo N. BramantyaNoch keine Bewertungen
- CXR English TemplateDokument2 SeitenCXR English TemplateIdo N. BramantyaNoch keine Bewertungen
- How Can China Respond To Global Market TurmoilDokument6 SeitenHow Can China Respond To Global Market TurmoilIdo N. BramantyaNoch keine Bewertungen
- He Touched Me LyricDokument1 SeiteHe Touched Me LyricIdo N. BramantyaNoch keine Bewertungen
- Directly Quantitated Dietary (N-3) Fatty Acid Intakes of Pregnant CanadianDokument6 SeitenDirectly Quantitated Dietary (N-3) Fatty Acid Intakes of Pregnant CanadianIdo N. BramantyaNoch keine Bewertungen
- NEURORADIOLOGYDokument1 SeiteNEURORADIOLOGYIdo N. BramantyaNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- A Guide For Gay and Bisexual MenDokument36 SeitenA Guide For Gay and Bisexual MenpantelisNoch keine Bewertungen
- Case Study On Prostatic CancerDokument21 SeitenCase Study On Prostatic CancerJai - Ho100% (3)
- Proton Beam Therapy For Cancer of The ProstateDokument14 SeitenProton Beam Therapy For Cancer of The Prostateالفيزياء الطبيةNoch keine Bewertungen
- ONC1119 Ezine PDFDokument48 SeitenONC1119 Ezine PDFdanishNoch keine Bewertungen
- New TNMDokument157 SeitenNew TNMShouvik ChowdhuryNoch keine Bewertungen
- Red FlagsDokument215 SeitenRed FlagsNovia Diba100% (1)
- Ayurvedic Treatment of Enlarged Prostate GlandDokument28 SeitenAyurvedic Treatment of Enlarged Prostate GlandRajeshKizziNoch keine Bewertungen
- Diabetes and Cancer: A Consensus ReportDokument12 SeitenDiabetes and Cancer: A Consensus ReportDeekay06Noch keine Bewertungen
- 12 Health Healing FoodsDokument10 Seiten12 Health Healing FoodsBahukhandiNoch keine Bewertungen
- 2018 - Alshammari The Benign Prostatic Hyperplasia and It's AetiologiesDokument6 Seiten2018 - Alshammari The Benign Prostatic Hyperplasia and It's AetiologieskanaNoch keine Bewertungen
- NLS DiagnosticsDokument71 SeitenNLS DiagnosticsMarkus van der WesthuizenNoch keine Bewertungen
- One Cancer Cure - March 2012Dokument52 SeitenOne Cancer Cure - March 2012ed_corcoran83% (6)
- Medical Facts and Mcq's Urology MCQDokument14 SeitenMedical Facts and Mcq's Urology MCQSmart Urosurgeon100% (2)
- Genitourinary Radiology ExamDokument9 SeitenGenitourinary Radiology ExamNour NoorNoch keine Bewertungen
- 2020 1Dokument38 Seiten2020 1Nasser AlbaddaiNoch keine Bewertungen
- Axumin Image Interpretation 8-28-2020Dokument86 SeitenAxumin Image Interpretation 8-28-2020Joseph GlaserNoch keine Bewertungen
- Medicare National Coverage Determinations ManualDokument142 SeitenMedicare National Coverage Determinations ManualEvaNoch keine Bewertungen
- Methods of Cancer Diagnosis, Therapy and Prognosis - Brain Cancer (Methods of Cancer Diagnosis, Therapy and Prognosis, Volume 8) (PDFDrive)Dokument426 SeitenMethods of Cancer Diagnosis, Therapy and Prognosis - Brain Cancer (Methods of Cancer Diagnosis, Therapy and Prognosis, Volume 8) (PDFDrive)dynamite 430Noch keine Bewertungen
- Lessons To Be Learned From Recent Biosafety Incidents in The UsaDokument5 SeitenLessons To Be Learned From Recent Biosafety Incidents in The UsaSANTIAGO HARVEY BENAVIDES RINCONNoch keine Bewertungen
- Murtaghs Patient Education, 6th Edition by John MurtaghDokument369 SeitenMurtaghs Patient Education, 6th Edition by John MurtaghHelp Line100% (2)
- Tumor Markers: Universiti Kuala Lumpur (Unikl) - Where Knowledge Is Applied and Dreams RealizedDokument29 SeitenTumor Markers: Universiti Kuala Lumpur (Unikl) - Where Knowledge Is Applied and Dreams RealizedNida RidzuanNoch keine Bewertungen
- Biology of Prostate Specific Antigen PDFDokument9 SeitenBiology of Prostate Specific Antigen PDFKaren BotiaNoch keine Bewertungen
- Homologous Recombination Deficiency (HRD) Score in Aggressive Prostatic Adenocarcinoma With or Without Intraductal Carcinoma of The Prostate (IDC-P)Dokument13 SeitenHomologous Recombination Deficiency (HRD) Score in Aggressive Prostatic Adenocarcinoma With or Without Intraductal Carcinoma of The Prostate (IDC-P)Dr Meenakshi ParwaniNoch keine Bewertungen
- Kelley Eidem Recipes For CancerDokument4 SeitenKelley Eidem Recipes For CancerRohinee SinghNoch keine Bewertungen
- 2023 Pca CV Expert Panel Virtual Meeting - Pre-ReadDokument48 Seiten2023 Pca CV Expert Panel Virtual Meeting - Pre-ReadPashoKiatNoch keine Bewertungen
- LABORATORY - ACP DeterminationDokument2 SeitenLABORATORY - ACP DeterminationTrisha GarciaNoch keine Bewertungen
- Abstracts USICON2017Dokument618 SeitenAbstracts USICON2017rdLuis1Noch keine Bewertungen
- Ayurstate Prostate HealthDokument11 SeitenAyurstate Prostate Healthnewlance777Noch keine Bewertungen
- (Basic Surg A) Oncology-Dr. Acuna (Sleepy Crammers)Dokument3 Seiten(Basic Surg A) Oncology-Dr. Acuna (Sleepy Crammers)Mildred DagaleaNoch keine Bewertungen
- Cancer BookDokument82 SeitenCancer Bookvarg12184315100% (15)