Das könnte Ihnen auch gefallen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- BASL Statement On Fuel Shortages and Its Impact 27th Jun 22Dokument3 SeitenBASL Statement On Fuel Shortages and Its Impact 27th Jun 22Thavam RatnaNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Oral Update On Global Human Rights Developments and The Activities of The UN Human Rights OfficeDokument13 SeitenOral Update On Global Human Rights Developments and The Activities of The UN Human Rights OfficeThavam RatnaNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- As A 3757232022 EnglishDokument3 SeitenAs A 3757232022 EnglishThavam RatnaNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Agriculture Faculties - Strategies For Addressing The Crises June 2022Dokument21 SeitenAgriculture Faculties - Strategies For Addressing The Crises June 2022Thavam RatnaNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Israeli Left Has Broken The Nakba TabooDokument15 SeitenThe Israeli Left Has Broken The Nakba TabooThavam RatnaNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Critical Resources, Imperialism and The War Against Russia: Ruined Total EstimatesDokument17 SeitenCritical Resources, Imperialism and The War Against Russia: Ruined Total EstimatesThavam RatnaNoch keine Bewertungen
- Situation BriefingDokument14 SeitenSituation BriefingThavam RatnaNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Proposals of The Bar Association of Sri Lanka To Restore Political and Economic Stability in The Country.Dokument8 SeitenProposals of The Bar Association of Sri Lanka To Restore Political and Economic Stability in The Country.Adaderana OnlineNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The War On YouthDokument16 SeitenThe War On YouthThavam RatnaNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- ITJP 1989 Mass Grave Report v6 WEBDokument43 SeitenITJP 1989 Mass Grave Report v6 WEBThavam RatnaNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Manoomin May DayDokument14 SeitenManoomin May DayThavam RatnaNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Why The IMF Is Bad For Sri LankaDokument15 SeitenWhy The IMF Is Bad For Sri LankaThavam RatnaNoch keine Bewertungen
- GGG Media Statement 09 MayDokument1 SeiteGGG Media Statement 09 MayThavam RatnaNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Draft of The Proposed 21st AmendmentDokument60 SeitenDraft of The Proposed 21st AmendmentNews CutterNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- YJA Lawyers For People Letter To UN On Freedom of Expression Assembly 19april2022 1Dokument4 SeitenYJA Lawyers For People Letter To UN On Freedom of Expression Assembly 19april2022 1Thavam RatnaNoch keine Bewertungen
- As A 3752782022 EnglishDokument26 SeitenAs A 3752782022 EnglishThavam RatnaNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Building Resilience in Stressful TimesDokument9 SeitenBuilding Resilience in Stressful TimesThavam RatnaNoch keine Bewertungen
- The Impacts of Green New Deals On Latin AmericaDokument10 SeitenThe Impacts of Green New Deals On Latin AmericaThavam RatnaNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- SLB Update 11 April 22 Key Takeaways of Week 2 GoHome Gota Protests in Sri LankaDokument2 SeitenSLB Update 11 April 22 Key Takeaways of Week 2 GoHome Gota Protests in Sri LankaThavam RatnaNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Dots Were All ThereDokument10 SeitenThe Dots Were All ThereThavam RatnaNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- ICE Continues To Abuse and Traumatize Under BidenDokument13 SeitenICE Continues To Abuse and Traumatize Under BidenThavam RatnaNoch keine Bewertungen
- Additional Joint Letter To Lord Ahmad by Tamil MPs & Leaders (3 Signatories) - March 2022Dokument7 SeitenAdditional Joint Letter To Lord Ahmad by Tamil MPs & Leaders (3 Signatories) - March 2022Thavam RatnaNoch keine Bewertungen
- SLB Briefing Note No 24. Easter Sunday Attacks Accountability Justice and The Deep StateDokument24 SeitenSLB Briefing Note No 24. Easter Sunday Attacks Accountability Justice and The Deep StateThavam RatnaNoch keine Bewertungen
- Plantation Workers Protest - March 08th, 2022Dokument2 SeitenPlantation Workers Protest - March 08th, 2022Thavam RatnaNoch keine Bewertungen
- FR Petititon SDIG Ravi SenvirathnaDokument35 SeitenFR Petititon SDIG Ravi SenvirathnaThavam RatnaNoch keine Bewertungen
- Chirantha Amerasinghe: Very UrentDokument6 SeitenChirantha Amerasinghe: Very UrentThavam RatnaNoch keine Bewertungen
- Sharni A FR Petition Re Imminant ArrestDokument36 SeitenSharni A FR Petition Re Imminant ArrestThavam RatnaNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- As A 3752412022 EnglishDokument10 SeitenAs A 3752412022 EnglishThavam RatnaNoch keine Bewertungen
- Sharni A FR Petition Re Imminant ArrestDokument36 SeitenSharni A FR Petition Re Imminant ArrestThavam RatnaNoch keine Bewertungen
- Project Descriptions Covid Recovery FundDokument2 SeitenProject Descriptions Covid Recovery FundThavam RatnaNoch keine Bewertungen
- Nsa 2021Dokument32 SeitenNsa 2021Mayank Mani SinghNoch keine Bewertungen
- My RubricDokument2 SeitenMy RubricLouie PaaNoch keine Bewertungen
- The Social Studies Curriculum, 1Dokument21 SeitenThe Social Studies Curriculum, 1Felix III AlcarezNoch keine Bewertungen
- FS 2 - Episode 2Dokument6 SeitenFS 2 - Episode 2ginelyn.tarimanNoch keine Bewertungen
- Lesson 3.1 NSQF and Implementation in Vocational TrainingDokument5 SeitenLesson 3.1 NSQF and Implementation in Vocational TrainingAkhil MuraliNoch keine Bewertungen
- San Roque Catholic School: Mendiola St. Alabang, Muntinlupa City / 1770 Tel No's: 842/2017 - 850/4236Dokument1 SeiteSan Roque Catholic School: Mendiola St. Alabang, Muntinlupa City / 1770 Tel No's: 842/2017 - 850/4236Ricky John TeruelNoch keine Bewertungen
- Instructional CoachingDokument257 SeitenInstructional CoachingAnandraj Govindaraj100% (3)
- JAGANNATHDokument42 SeitenJAGANNATHforhadNoch keine Bewertungen
- 3-Way TOS PE 8Dokument3 Seiten3-Way TOS PE 8ANN QUIBERNoch keine Bewertungen
- MC4 CoCU 6 - Welding Records and Report DocumentationDokument8 SeitenMC4 CoCU 6 - Welding Records and Report Documentationnizam1372100% (1)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Challenges With Project An (All Numerates)Dokument11 SeitenChallenges With Project An (All Numerates)zaldy mendozaNoch keine Bewertungen
- Be Inspired by Global Opportunities!Dokument3 SeitenBe Inspired by Global Opportunities!HASIBA MithunNoch keine Bewertungen
- THESISDokument37 SeitenTHESISMiah RM95% (104)
- Diana Mihalache Supervision Note Template PDFDokument2 SeitenDiana Mihalache Supervision Note Template PDFDiana MihalacheNoch keine Bewertungen
- 10-20-2022 Apb Lesson PlanDokument2 Seiten10-20-2022 Apb Lesson Planapi-674548860Noch keine Bewertungen
- RPH Mat THN 3 DLP 2.3.1Dokument2 SeitenRPH Mat THN 3 DLP 2.3.1Mikeru4lee MikeruliNoch keine Bewertungen
- DifferentiationDokument3 SeitenDifferentiationapi-286258588Noch keine Bewertungen
- Proforma KPN4053 Semester 2 20222023Dokument14 SeitenProforma KPN4053 Semester 2 20222023Fiza HamzahNoch keine Bewertungen
- Jill K. Hatanaka: San Joaquin County Office of Education 2707 Transworld Drive Stockton, CA 95206 209-401-2406Dokument3 SeitenJill K. Hatanaka: San Joaquin County Office of Education 2707 Transworld Drive Stockton, CA 95206 209-401-2406api-114772135Noch keine Bewertungen
- Thesis Topics For PHD in CommerceDokument4 SeitenThesis Topics For PHD in Commerceafcnftqep100% (2)
- Determinants of Business Student Satisfaction and Retention in Higher Education: Applying Herzberg's Two Factor TheoryDokument8 SeitenDeterminants of Business Student Satisfaction and Retention in Higher Education: Applying Herzberg's Two Factor TheoryRakesh KumarNoch keine Bewertungen
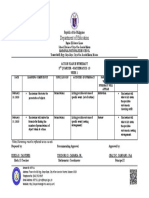
- Action Plan in NumeracyDokument1 SeiteAction Plan in NumeracyBeverly FlorentinoNoch keine Bewertungen
- Degree Abbreviations and GradingDokument6 SeitenDegree Abbreviations and GradingWitlrNoch keine Bewertungen
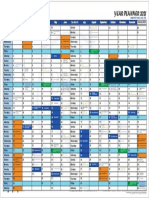
- Year Planner 2021 - Final - 18-1-21-Shabebarat-Web2Dokument1 SeiteYear Planner 2021 - Final - 18-1-21-Shabebarat-Web2Song AlexNoch keine Bewertungen
- Perception of High School Students About TheDokument24 SeitenPerception of High School Students About Theronnie gallanoNoch keine Bewertungen
- Educ3025 Science in Early Childhood Assessment 2 Activity Planner Neo TandyDokument21 SeitenEduc3025 Science in Early Childhood Assessment 2 Activity Planner Neo Tandyapi-396981495Noch keine Bewertungen
- UCAS Co Ordinator Applicant Information PackDokument8 SeitenUCAS Co Ordinator Applicant Information PackJames BennettNoch keine Bewertungen
- Ap Eng Lit Comp Teachers GuideDokument114 SeitenAp Eng Lit Comp Teachers Guideapi-252721756Noch keine Bewertungen
- 2023 COT (Second Quarter)Dokument5 Seiten2023 COT (Second Quarter)Aura Lee Carisma100% (1)
- The Nature of Scientific KnowledgeDokument281 SeitenThe Nature of Scientific KnowledgeAfa100% (4)