Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- DR ErinaDokument14 SeitenDR ErinaFemmy RuthNoch keine Bewertungen
- Application LetterDokument1 SeiteApplication LetterFemmy RuthNoch keine Bewertungen
- Ebram Assigment (Ma'Am Sondang)Dokument7 SeitenEbram Assigment (Ma'Am Sondang)Femmy RuthNoch keine Bewertungen
- Biogrpy of William BlakeDokument7 SeitenBiogrpy of William BlakeFemmy RuthNoch keine Bewertungen
- Biogrpy of William BlakeDokument7 SeitenBiogrpy of William BlakeFemmy RuthNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Nursing Care Plan Placenta PreviaDokument2 SeitenNursing Care Plan Placenta PreviaApril Ann HortilanoNoch keine Bewertungen
- Dr. Khairiyadi, M.Kes., Sp.A Departemen Ilmu Kesehatan Anak RSUD Ulin BanjarmasinDokument78 SeitenDr. Khairiyadi, M.Kes., Sp.A Departemen Ilmu Kesehatan Anak RSUD Ulin BanjarmasinEldhaNoch keine Bewertungen
- 0199975744Dokument305 Seiten0199975744nicoletaelenaNoch keine Bewertungen
- Slides From McCullough 10-27-2021 PresentationDokument83 SeitenSlides From McCullough 10-27-2021 PresentationAssociation of American Physicians and Surgeons100% (10)
- Sepsis and CellulitisDokument2 SeitenSepsis and Cellulitisryan_weldon_3Noch keine Bewertungen
- Disorders of Coagulation FactorsDokument35 SeitenDisorders of Coagulation FactorsMelesNoch keine Bewertungen
- Case Study On Nephrotic SyndromeDokument7 SeitenCase Study On Nephrotic SyndromeArchana VermaNoch keine Bewertungen
- ICD-10 TK Pedsos 2013Dokument10 SeitenICD-10 TK Pedsos 2013Ludi Dhyani RahmartaniNoch keine Bewertungen
- Diabetis 2Dokument33 SeitenDiabetis 2Fercho MedNoch keine Bewertungen
- Metformin, Glucophage, Glucophage XR, Glumetza, Fortamet, RiometDokument5 SeitenMetformin, Glucophage, Glucophage XR, Glumetza, Fortamet, RiometAgronaSlaughterNoch keine Bewertungen
- Drug Name Gemcitabine: Synonym (S) : Common Trade Name (S) : ClassificationDokument8 SeitenDrug Name Gemcitabine: Synonym (S) : Common Trade Name (S) : ClassificationOka Robi MuhammadNoch keine Bewertungen
- Buttaravoli, Philip - Minor Emergencies - Blunt Scrotal Trauma (2007)Dokument3 SeitenButtaravoli, Philip - Minor Emergencies - Blunt Scrotal Trauma (2007)Vivian ChanNoch keine Bewertungen
- Broiler Breeder DiseasesDokument12 SeitenBroiler Breeder DiseasesvetbcasNoch keine Bewertungen
- Kaposi SarcomaDokument11 SeitenKaposi Sarcomaedgar mandengNoch keine Bewertungen
- Neck Pain: Simple ExercisesDokument2 SeitenNeck Pain: Simple ExercisesVijaya Krishna DevarapalliNoch keine Bewertungen
- Aches and Pains in The ElderlyDokument34 SeitenAches and Pains in The ElderlyAna CampeanuNoch keine Bewertungen
- em Exam - 1-AnswersDokument3 Seitenem Exam - 1-AnswersAzra MuzafarNoch keine Bewertungen
- A Case Study of Bronchial Asthma in Acute Exacerbation (Baiae)Dokument13 SeitenA Case Study of Bronchial Asthma in Acute Exacerbation (Baiae)Samantha BolanteNoch keine Bewertungen
- Jabeen & TahirDokument12 SeitenJabeen & TahirSanaNoch keine Bewertungen
- Using Sugar To Treat Those Nasty Wounds: American Farriers Journal Special Management Report #1..Dokument3 SeitenUsing Sugar To Treat Those Nasty Wounds: American Farriers Journal Special Management Report #1..alfirafresdiNoch keine Bewertungen
- Therapy of Acute Respiratory Infections in Children: NoveltiesDokument11 SeitenTherapy of Acute Respiratory Infections in Children: NoveltiesrizkaNoch keine Bewertungen
- TB in Special SituationsDokument49 SeitenTB in Special SituationsVipul KumarNoch keine Bewertungen
- Berikut Ini Macam Macam Penyakit Dan Istilah MedisDokument24 SeitenBerikut Ini Macam Macam Penyakit Dan Istilah MedisIis Izy IssooNoch keine Bewertungen
- HealthMeans Lets Talk About AutoimmunityDokument37 SeitenHealthMeans Lets Talk About AutoimmunityvaleriabostanNoch keine Bewertungen
- THC AspergerDokument168 SeitenTHC AspergerMICHAELNoch keine Bewertungen
- MetoprololDokument3 SeitenMetoprololapi-3797941100% (3)
- Endocrine NCLEX PN Pract & ANS Questions IIDokument13 SeitenEndocrine NCLEX PN Pract & ANS Questions IIYA HONoch keine Bewertungen
- AZ Heart Angioscreen - Biltmore Lifestyles Dec 2022Dokument1 SeiteAZ Heart Angioscreen - Biltmore Lifestyles Dec 2022Brittany LudwigNoch keine Bewertungen
- Kode Kombinasi Icd 10 Dan Icd 9 Indonesia Update 2018Dokument10 SeitenKode Kombinasi Icd 10 Dan Icd 9 Indonesia Update 2018Dini AzizahNoch keine Bewertungen
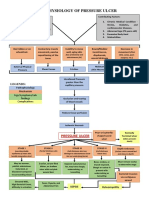
- Pathophysiology of Pressure UlcerDokument1 SeitePathophysiology of Pressure UlcerSTORAGE FILENoch keine Bewertungen