Das könnte Ihnen auch gefallen
- Dialysis Access ManagementVon EverandDialysis Access ManagementSteven WuNoch keine Bewertungen
- 2020 - Feasibility and Safety of Peripheral Intravenous Administration of Vasopressor Agents in Resource-Limited SettingsDokument7 Seiten2020 - Feasibility and Safety of Peripheral Intravenous Administration of Vasopressor Agents in Resource-Limited SettingsAndre OliveiraNoch keine Bewertungen
- Vsa Por PerisfericoDokument8 SeitenVsa Por PerisfericoMaritza Alejandra Baeza EricesNoch keine Bewertungen
- Device Selection: Nancy L. Moureau and Evan AlexandrouDokument19 SeitenDevice Selection: Nancy L. Moureau and Evan AlexandrouCarmen T OrtizNoch keine Bewertungen
- Peripherally Inserted Central Venous Acces - 2021 - Seminars in Pediatric SurgerDokument8 SeitenPeripherally Inserted Central Venous Acces - 2021 - Seminars in Pediatric Surgeralergo.ramirezNoch keine Bewertungen
- Central or Peripheral Catheters For Initial Venous Access of ICU Patients: A Randomized Controlled TrialDokument8 SeitenCentral or Peripheral Catheters For Initial Venous Access of ICU Patients: A Randomized Controlled TrialAndrés Fuica de la VegaNoch keine Bewertungen
- Exercise Is Feasible in Patients Receiving Vasoactive Medication in A Cardiac Surgical Intensive Care Unit - A Prospective Observational StudyDokument6 SeitenExercise Is Feasible in Patients Receiving Vasoactive Medication in A Cardiac Surgical Intensive Care Unit - A Prospective Observational Studyrayanna dornelesNoch keine Bewertungen
- Inferior Vena Cava Ultrasonography For Volume Status EvaluationDokument13 SeitenInferior Vena Cava Ultrasonography For Volume Status Evaluationtavo570Noch keine Bewertungen
- JPediatrNeurosci132176-312375 084037Dokument6 SeitenJPediatrNeurosci132176-312375 084037afriska chandraNoch keine Bewertungen
- 10 1053@j Jvca 2019 05 017 PDFDokument6 Seiten10 1053@j Jvca 2019 05 017 PDFangelicaNoch keine Bewertungen
- Augmentation - of - Dural - Closure - Following - Cerebro-SpDokument7 SeitenAugmentation - of - Dural - Closure - Following - Cerebro-SpChiNdy AfiSaNoch keine Bewertungen
- Bmjopen 2014 007257Dokument7 SeitenBmjopen 2014 007257rezzkNoch keine Bewertungen
- Nso Week-03Dokument3 SeitenNso Week-03HAILA NICOLE S. ALVAREZNoch keine Bewertungen
- Transcortical Approach Surgery Versus External Ventricular Drainage in Treating IVHDokument6 SeitenTranscortical Approach Surgery Versus External Ventricular Drainage in Treating IVHResiden BedahNoch keine Bewertungen
- Vanc Article 5BTDokument7 SeitenVanc Article 5BTLeslie AdamsNoch keine Bewertungen
- ResOpinAnesthIntensiveCare83159-6419947 174959Dokument8 SeitenResOpinAnesthIntensiveCare83159-6419947 174959paulosabino1977Noch keine Bewertungen
- Clinical Review - Full PDFDokument5 SeitenClinical Review - Full PDFsitikhumaironiNoch keine Bewertungen
- ATLS Tenth EdDokument45 SeitenATLS Tenth Edakreditasi standar2Noch keine Bewertungen
- Drugs Icu Iv OkDokument26 SeitenDrugs Icu Iv OkManuela CormioNoch keine Bewertungen
- UgiendosDokument12 SeitenUgiendosManoj BurdakNoch keine Bewertungen
- Positive Effect of Care Bundles On Patients With Central Venous Catheter Insertions at A Tertiary Hospital in Beijing, ChinaDokument10 SeitenPositive Effect of Care Bundles On Patients With Central Venous Catheter Insertions at A Tertiary Hospital in Beijing, ChinaElfina NataliaNoch keine Bewertungen
- s13054 021 03553 1Dokument12 Seitens13054 021 03553 1algoNoch keine Bewertungen
- Prevalence of Phlebitis Among Patients Receiving Peripheral Intravenous Therapy in A Tertiary Care Hospital in IndiaDokument6 SeitenPrevalence of Phlebitis Among Patients Receiving Peripheral Intravenous Therapy in A Tertiary Care Hospital in IndiaIJAR JOURNALNoch keine Bewertungen
- Contemporary Analysis of The Intraoperative and Perioperative Complications of Neurosurgical Procedures Performed in The Sitting PositionDokument7 SeitenContemporary Analysis of The Intraoperative and Perioperative Complications of Neurosurgical Procedures Performed in The Sitting PositionLloyd AllenNoch keine Bewertungen
- Manajemen EpistaksisDokument2 SeitenManajemen EpistaksistiaraaaindahNoch keine Bewertungen
- Infiltration and Extravasation Update On.10Dokument9 SeitenInfiltration and Extravasation Update On.10Beauty CassieNoch keine Bewertungen
- Use of Short Peripheral Intravenous Catheters: Characteristics, Management, and Outcomes WorldwideDokument7 SeitenUse of Short Peripheral Intravenous Catheters: Characteristics, Management, and Outcomes WorldwidemochkurniawanNoch keine Bewertungen
- 508 - 7 CardiologyDokument9 Seiten508 - 7 CardiologymlinaballerinaNoch keine Bewertungen
- Interventional Nephrology: From Episodic To Coordinated Vascular Access CareDokument8 SeitenInterventional Nephrology: From Episodic To Coordinated Vascular Access Caredal81_aksNoch keine Bewertungen
- 2009 Venous AccessDokument3 Seiten2009 Venous AccessDaniela MéndezNoch keine Bewertungen
- NPPEDokument8 SeitenNPPEjijocasoNoch keine Bewertungen
- Jurnal VaskularDokument5 SeitenJurnal VaskulardrelvNoch keine Bewertungen
- Enfermeria CateterDokument13 SeitenEnfermeria CateterJaime Augusto Quimbayo GuarnizoNoch keine Bewertungen
- Safety and Effectiveness of Inferior Vena Cava Filters Used To Protect Against Pulmonary EmbolusDokument26 SeitenSafety and Effectiveness of Inferior Vena Cava Filters Used To Protect Against Pulmonary EmbolusCalifornia Technology Assessment ForumNoch keine Bewertungen
- Infusion Nursing Standards of PracticeDokument2 SeitenInfusion Nursing Standards of Practiceajip ejepNoch keine Bewertungen
- Complications of Arteriovenous Fistula For Haemodialysis AccessDokument6 SeitenComplications of Arteriovenous Fistula For Haemodialysis AccessAkiko Syawalidhany TahirNoch keine Bewertungen
- Tip 2Dokument5 SeitenTip 2Anis Eka SukmadadariNoch keine Bewertungen
- Cerebral Oximetry Monitoring To Maintain Normal Cerebral ExplainDokument11 SeitenCerebral Oximetry Monitoring To Maintain Normal Cerebral ExplainDaniel EllerNoch keine Bewertungen
- Fluid Administration For Acute Circulatory Dysfunction Using Basic Monitoring Narrative Review and Expert Panel Recommendations From An ESICM Task Force Maurizio CecconDokument12 SeitenFluid Administration For Acute Circulatory Dysfunction Using Basic Monitoring Narrative Review and Expert Panel Recommendations From An ESICM Task Force Maurizio CecconEllys Macías PeraltaNoch keine Bewertungen
- Academic Emergency Medicine - July 1996 - Shoemaker - Noninvasive Hemodynamic Monitoring of Critical Patients in TheDokument9 SeitenAcademic Emergency Medicine - July 1996 - Shoemaker - Noninvasive Hemodynamic Monitoring of Critical Patients in TheAndres Pimentel AlvarezNoch keine Bewertungen
- CVC RemovalDokument5 SeitenCVC RemovalRiza ZaharaNoch keine Bewertungen
- Loss of A Guidewire: SciencedirectDokument3 SeitenLoss of A Guidewire: SciencedirectSA SHNoch keine Bewertungen
- cm9 134 1043Dokument9 Seitencm9 134 1043Yudha PramanaNoch keine Bewertungen
- Active Fluid De-Resuscitacion in Crtiticalli III Patients Whitj ShockDokument8 SeitenActive Fluid De-Resuscitacion in Crtiticalli III Patients Whitj ShockMartha Isabel BurgosNoch keine Bewertungen
- Practice Guidelines For Central Venous Access 2020 An Updated Report by The American Society of Anesthesiologists Task Force On Central Venous Access PDFDokument36 SeitenPractice Guidelines For Central Venous Access 2020 An Updated Report by The American Society of Anesthesiologists Task Force On Central Venous Access PDFDaniel Castro VeintimillaNoch keine Bewertungen
- 06 2010 Jun Central-Venous-CatheterDokument6 Seiten06 2010 Jun Central-Venous-CatheterFrancisco VigenorNoch keine Bewertungen
- Hestin 2022 Time To Medical Fitness For DischarDokument8 SeitenHestin 2022 Time To Medical Fitness For DischarAmro MahmoudNoch keine Bewertungen
- Temporary Inferior Vena Cava Filters: How Do We Move Forward?Dokument3 SeitenTemporary Inferior Vena Cava Filters: How Do We Move Forward?MostafaNoch keine Bewertungen
- Intravenous Fluids in Acute Decompensated Heart FailureDokument7 SeitenIntravenous Fluids in Acute Decompensated Heart FailureaulianaNoch keine Bewertungen
- 2020 Bilateral-Pectoral Major Muscle Advancement Flap Combined With Vacuumassisted Closure Therapy For The Treatment of Deep Sternal Wound Infections AfterDokument8 Seiten2020 Bilateral-Pectoral Major Muscle Advancement Flap Combined With Vacuumassisted Closure Therapy For The Treatment of Deep Sternal Wound Infections Afterplay259Noch keine Bewertungen
- 17 Dirckx, Wound TherapyDokument3 Seiten17 Dirckx, Wound TherapyTor ChiuNoch keine Bewertungen
- Management of Epistaxis in Patients With Ventricular Assist Device: A Retrospective ReviewDokument6 SeitenManagement of Epistaxis in Patients With Ventricular Assist Device: A Retrospective ReviewDenta HaritsaNoch keine Bewertungen
- Deep Venous Thrombosis After Percutaneous Insertion of Vena Caval FiltersDokument9 SeitenDeep Venous Thrombosis After Percutaneous Insertion of Vena Caval Filtersari kurniawanNoch keine Bewertungen
- VP Shunt ComplicationDokument6 SeitenVP Shunt ComplicationMary Christina ElsaNoch keine Bewertungen
- Effects of Intraoperative Epidural Anesthesia During Hepatectomy On Intraoperative and Post-Operative Patient OutcomesDokument8 SeitenEffects of Intraoperative Epidural Anesthesia During Hepatectomy On Intraoperative and Post-Operative Patient OutcomesAfniNoch keine Bewertungen
- Ultrasound Guidance For Central Venous AccessDokument19 SeitenUltrasound Guidance For Central Venous AccessCAMILO FERRERO RESTREPONoch keine Bewertungen
- Retrospective Observational Study of Patient Outcomes With Local Wound Infusion Vs Epidural Analgesia After Open Hepato-Pancreato-Biliary SurgeryDokument8 SeitenRetrospective Observational Study of Patient Outcomes With Local Wound Infusion Vs Epidural Analgesia After Open Hepato-Pancreato-Biliary Surgeryvalerio.messinaNoch keine Bewertungen
- External Jugular Vein Peripheral IntravenousDokument7 SeitenExternal Jugular Vein Peripheral Intravenoushector nuñezNoch keine Bewertungen
- ProspectDokument8 SeitenProspectValentina MerolaNoch keine Bewertungen
- Man Zur 2017Dokument7 SeitenMan Zur 2017sinidok SinidokNoch keine Bewertungen
- Bonus 6 - Mastering ASP - NET Core SecurityDokument147 SeitenBonus 6 - Mastering ASP - NET Core SecurityDark Shadow100% (1)
- Apples-to-Apples in Cross-Validation Studies: Pitfalls in Classifier Performance MeasurementDokument9 SeitenApples-to-Apples in Cross-Validation Studies: Pitfalls in Classifier Performance MeasurementLuis Martínez RamírezNoch keine Bewertungen
- This Tutorial Will Help To Test The Throttle Position Sensor On Your 1989 To 1997 1Dokument7 SeitenThis Tutorial Will Help To Test The Throttle Position Sensor On Your 1989 To 1997 1HERBERT SITORUS100% (1)
- Add MITx Credentials To Resume and LinkedIn PDFDokument5 SeitenAdd MITx Credentials To Resume and LinkedIn PDFRizwanNoch keine Bewertungen
- Land Surveying Chapter 2 Leveling p1Dokument66 SeitenLand Surveying Chapter 2 Leveling p1Azrul ZulwaliNoch keine Bewertungen
- PCIB Vs Escolin DigestDokument3 SeitenPCIB Vs Escolin DigestsamontedianneNoch keine Bewertungen
- Ten Rules of NetiquetteDokument11 SeitenTen Rules of NetiquetteAriel CancinoNoch keine Bewertungen
- Corality ModelOff Sample Answer Hard TimesDokument81 SeitenCorality ModelOff Sample Answer Hard TimesserpepeNoch keine Bewertungen
- Cold Rolled CoilDokument23 SeitenCold Rolled Coilmametcool100% (1)
- Invoice SummaryDokument2 SeitenInvoice SummarymuNoch keine Bewertungen
- ADM3346A Midterm Fall 2010 SolutionDokument10 SeitenADM3346A Midterm Fall 2010 SolutionJohn BecksNoch keine Bewertungen
- Sample Deed of DonationDokument2 SeitenSample Deed of DonationMenchie Ann Sabandal Salinas100% (1)
- Best of SEO#1 SEO Training & Content Marketing Course 2022Dokument2 SeitenBest of SEO#1 SEO Training & Content Marketing Course 2022Oscar MascarenoNoch keine Bewertungen
- DS - LWT300 - SF - A4 EN Rev BDokument4 SeitenDS - LWT300 - SF - A4 EN Rev BZts MksNoch keine Bewertungen
- Puch Moped Horn Wiring Diagram (Chrome Oval Switches)Dokument1 SeitePuch Moped Horn Wiring Diagram (Chrome Oval Switches)MopedgalNoch keine Bewertungen
- Epsilon Range Bomba HorizontalDokument8 SeitenEpsilon Range Bomba HorizontalsalazarafaelNoch keine Bewertungen
- Contoh CV Pelaut Untuk CadetDokument1 SeiteContoh CV Pelaut Untuk CadetFadli Ramadhan100% (1)
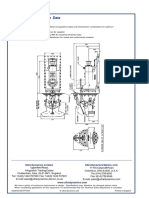
- Ultrajet 376 Installation Data: Ultra Dynamics Marine, LCC Ultra Dynamics LimitedDokument2 SeitenUltrajet 376 Installation Data: Ultra Dynamics Marine, LCC Ultra Dynamics LimitedhaujesNoch keine Bewertungen
- Hydraulic Power Unit: RE 51057, Edition: 2020-11, Bosch Rexroth AGDokument20 SeitenHydraulic Power Unit: RE 51057, Edition: 2020-11, Bosch Rexroth AGHanzil HakeemNoch keine Bewertungen
- Cronbach's AlphaDokument4 SeitenCronbach's AlphaHeide Orevillo Apa-apNoch keine Bewertungen
- School MemoDokument1 SeiteSchool MemoBellaNoch keine Bewertungen
- Taxicab Operators V BOTDokument2 SeitenTaxicab Operators V BOTHazel P.Noch keine Bewertungen
- CRM Short QuizDokument1 SeiteCRM Short QuizDaria Par-HughesNoch keine Bewertungen
- Production of BiodieselDokument49 SeitenProduction of Biodieselteja100% (1)
- FBL ManualDokument12 SeitenFBL Manualaurumstar2000Noch keine Bewertungen
- Peir Nts Section 8 BeDokument14 SeitenPeir Nts Section 8 BethamestunnelNoch keine Bewertungen
- Introduction To Investment AppraisalDokument43 SeitenIntroduction To Investment AppraisalNURAIN HANIS BINTI ARIFFNoch keine Bewertungen
- Guide To Manually Importing/Transferring Your Livery For FH4/FM7/FH3 PCDokument12 SeitenGuide To Manually Importing/Transferring Your Livery For FH4/FM7/FH3 PCLennike SantosNoch keine Bewertungen
- Clark Hess1Dokument668 SeitenClark Hess1Jeyner Chavez VasquezNoch keine Bewertungen
- OEM - Fuel Manager Brand Cross Reference P/Ns For Service Filter Elements 99642 - January 2006Dokument6 SeitenOEM - Fuel Manager Brand Cross Reference P/Ns For Service Filter Elements 99642 - January 2006Miguel RojasNoch keine Bewertungen
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (404)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 4 von 5 Sternen4/5 (4)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (34)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (4)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Von EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Bewertung: 3 von 5 Sternen3/5 (1)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipVon EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipBewertung: 4.5 von 5 Sternen4.5/5 (1135)
- Breaking the Habit of Being YourselfVon EverandBreaking the Habit of Being YourselfBewertung: 4.5 von 5 Sternen4.5/5 (1461)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 4.5 von 5 Sternen4.5/5 (82)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsVon EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsBewertung: 4.5 von 5 Sternen4.5/5 (170)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- Peaceful Sleep Hypnosis: Meditate & RelaxVon EverandPeaceful Sleep Hypnosis: Meditate & RelaxBewertung: 4.5 von 5 Sternen4.5/5 (144)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Deep Sleep Hypnosis: Guided Meditation For Sleep & HealingVon EverandDeep Sleep Hypnosis: Guided Meditation For Sleep & HealingBewertung: 4.5 von 5 Sternen4.5/5 (104)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (44)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeVon EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeBewertung: 4.5 von 5 Sternen4.5/5 (254)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisVon EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisBewertung: 3.5 von 5 Sternen3.5/5 (2)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeVon EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeBewertung: 4.5 von 5 Sternen4.5/5 (2)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesVon EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesBewertung: 4.5 von 5 Sternen4.5/5 (1412)