Das könnte Ihnen auch gefallen
- Fetal CirculationDokument5 SeitenFetal Circulationbluemandrake2185Noch keine Bewertungen
- Fetal CirculationDokument5 SeitenFetal CirculationJaime PorscheNoch keine Bewertungen
- Fetal CirculationDokument2 SeitenFetal CirculationTracy88% (8)
- Fetal CirculationDokument5 SeitenFetal CirculationZam PamateNoch keine Bewertungen
- Fetal CirculationDokument13 SeitenFetal CirculationPraveen YadavNoch keine Bewertungen
- Fetal CirculationDokument2 SeitenFetal Circulationanon_414797925Noch keine Bewertungen
- Fetal Circulation...Dokument2 SeitenFetal Circulation...Ezra Dizon Manzano100% (1)
- Systemic Changes During PregnancyDokument2 SeitenSystemic Changes During PregnancyARAugusto67% (3)
- Fetal CirculationDokument2 SeitenFetal CirculationLeslie Cristine Abad0% (1)
- Fetal CirculationDokument6 SeitenFetal Circulationkc-orense-1005Noch keine Bewertungen
- High Risk Newborn2Dokument15 SeitenHigh Risk Newborn2Catherine Villanueva Sta Monica100% (1)
- Fetal CirculationDokument1 SeiteFetal CirculationMark James MelendresNoch keine Bewertungen
- Alterations in Oxygenation 1Dokument15 SeitenAlterations in Oxygenation 1alejandrino_leoaugustoNoch keine Bewertungen
- Pathophysiology of Birth AsphyxiaDokument14 SeitenPathophysiology of Birth AsphyxiaEduardo Rios DuboisNoch keine Bewertungen
- 07.04.05 Venturi Face Mask PDFDokument2 Seiten07.04.05 Venturi Face Mask PDFRosintchi MirsalNoch keine Bewertungen
- Fetal CirculationDokument27 SeitenFetal CirculationSureshChevagoniNoch keine Bewertungen
- Placental AbnormalitiesDokument3 SeitenPlacental AbnormalitiesThakoon TtsNoch keine Bewertungen
- Fetal CirculationDokument2 SeitenFetal CirculationgoldiemareNoch keine Bewertungen
- Endotracheal Tube SuctioningDokument5 SeitenEndotracheal Tube SuctioningArlene DalisayNoch keine Bewertungen
- Immediate Care of The NewbornDokument4 SeitenImmediate Care of The Newbornmelinda100% (1)
- Birth Asphyxia: by Anne E. Odaro MCM/2017/69852Dokument26 SeitenBirth Asphyxia: by Anne E. Odaro MCM/2017/69852ElvisNoch keine Bewertungen
- Machanical Ventilator Nursing Care PalnDokument13 SeitenMachanical Ventilator Nursing Care PalnAnnie Priscilla100% (1)
- Fetal CirculationDokument4 SeitenFetal CirculationTina Tin100% (1)
- Securing and Suctioning Endotracheal TubeDokument28 SeitenSecuring and Suctioning Endotracheal TubeJohn Mark ParacadNoch keine Bewertungen
- The PlacentaDokument3 SeitenThe PlacentaLiezelNoch keine Bewertungen
- Fetal CirculationDokument2 SeitenFetal CirculationLhovely ConwiNoch keine Bewertungen
- TracheostomyDokument4 SeitenTracheostomySuchismita SethiNoch keine Bewertungen
- Icu Equipments BY: Presented Bhupender Kumar MehtoDokument35 SeitenIcu Equipments BY: Presented Bhupender Kumar Mehtobhupendermehto012Noch keine Bewertungen
- Anaemia in Pregnancy: Dr. Lama MehaisenDokument11 SeitenAnaemia in Pregnancy: Dr. Lama MehaisenWendy EvansNoch keine Bewertungen
- Informatics Applications in Evidenced-Based Nursing PracticeDokument19 SeitenInformatics Applications in Evidenced-Based Nursing PracticeFiona Marie Berlon DyangkoNoch keine Bewertungen
- Anatomy and Physiology of The HeartDokument9 SeitenAnatomy and Physiology of The HeartNina Anne ParacadNoch keine Bewertungen
- CMCA LEC 12-IntrapartumDokument189 SeitenCMCA LEC 12-IntrapartumCarl Josef C. GarciaNoch keine Bewertungen
- Mechanical Ventilation Practice Guidelines: 1. 2. Initial Settings - ModeDokument12 SeitenMechanical Ventilation Practice Guidelines: 1. 2. Initial Settings - ModeGayathri RNoch keine Bewertungen
- True or False LaborDokument4 SeitenTrue or False LaborromyNoch keine Bewertungen
- Fetal CirculationDokument13 SeitenFetal CirculationHarish Kumar Kumawat100% (2)
- Ret Dem Bed Bath Hair Shampoo WUPDokument4 SeitenRet Dem Bed Bath Hair Shampoo WUPCarissa De Luzuriaga-BalariaNoch keine Bewertungen
- Fetal CirculationDokument15 SeitenFetal Circulationveegeer67% (3)
- Pregnancy Induced HypertensionDokument4 SeitenPregnancy Induced HypertensionMjhay SalvadorNoch keine Bewertungen
- Fetal Circulation ComprehensiveDokument2 SeitenFetal Circulation ComprehensiveMarisol Jane Jomaya100% (1)
- Assessment of A Pregnant FamilyDokument4 SeitenAssessment of A Pregnant FamilyLuna Sang-anNoch keine Bewertungen
- Umbilical Cord ProlapseDokument6 SeitenUmbilical Cord ProlapseCeth BeltranNoch keine Bewertungen
- Saint Paul University Philippines: School of Nursing and Allied Health SciencesDokument3 SeitenSaint Paul University Philippines: School of Nursing and Allied Health SciencesRaRe TVNoch keine Bewertungen
- Chapter 9: Nursing Care During Normal Pregnancy and Care of The Developing FetusDokument8 SeitenChapter 9: Nursing Care During Normal Pregnancy and Care of The Developing FetusAlyssaGrandeMontimor100% (1)
- TRANSPOSITION OF THE GREAT VESSELS PrintDokument8 SeitenTRANSPOSITION OF THE GREAT VESSELS PrintAnandhu GNoch keine Bewertungen
- Tracheostomy Slide Presentation-ZayChung - Pro.ksaDokument33 SeitenTracheostomy Slide Presentation-ZayChung - Pro.ksaZayChung100% (2)
- Respiratory Distress SyndromeDokument9 SeitenRespiratory Distress SyndromeRamina HiponiaNoch keine Bewertungen
- SuctioningDokument27 SeitenSuctioningMoni Mbumba MelekeNoch keine Bewertungen
- Fetal CirculationDokument22 SeitenFetal CirculationJSeasharkNoch keine Bewertungen
- NebulisationDokument26 SeitenNebulisationSilpa Jose TNoch keine Bewertungen
- Oral Medication PharmacologyDokument4 SeitenOral Medication PharmacologyElaisa Mae Delos SantosNoch keine Bewertungen
- Essential Newborn Care (Enc) & Delivery Room ProtocolsDokument95 SeitenEssential Newborn Care (Enc) & Delivery Room ProtocolsEyySiEffVeeNoch keine Bewertungen
- NEWBORN ASSESSMENT DajuuuuuuuuuuuuuuuuDokument31 SeitenNEWBORN ASSESSMENT Dajuuuuuuuuuuuuuuuuamal abdulrahmanNoch keine Bewertungen
- Foetal CirculationDokument107 SeitenFoetal CirculationDr_ibkNoch keine Bewertungen
- Birth Asphyxia: Prof RL Mbise PCH, ImtuDokument38 SeitenBirth Asphyxia: Prof RL Mbise PCH, ImtuCharles FrankNoch keine Bewertungen
- Abortion and Ectopic PregnancyDokument3 SeitenAbortion and Ectopic PregnancyJefelson Eu Palaña NahidNoch keine Bewertungen
- Practice Teaching Demonstration: Intracath InsertionDokument13 SeitenPractice Teaching Demonstration: Intracath InsertionMegha lakra100% (1)
- Croup PathwayDokument30 SeitenCroup Pathwayshluly23Noch keine Bewertungen
- Foetal CirculationDokument39 SeitenFoetal CirculationDr. Haricharan ANoch keine Bewertungen
- Congenital Heart DIseasesDokument3 SeitenCongenital Heart DIseasesAshan BopitiyaNoch keine Bewertungen
- Fetal Circulation in The WombDokument2 SeitenFetal Circulation in The WombChristineAlaNoch keine Bewertungen
- Karron 2022 Oi 220780 1661274164.53022Dokument14 SeitenKarron 2022 Oi 220780 1661274164.53022yusrinastitiNoch keine Bewertungen
- Jamapediatrics Chang 2021 Oi 210031 1630088703.56331Dokument11 SeitenJamapediatrics Chang 2021 Oi 210031 1630088703.56331yusrinastitiNoch keine Bewertungen
- 2598-Article Text-10075-1-10-20211219Dokument16 Seiten2598-Article Text-10075-1-10-20211219yusrinastitiNoch keine Bewertungen
- Surgery WHODokument133 SeitenSurgery WHOKaterina NahampunNoch keine Bewertungen
- 2598-Article Text-10075-1-10-20211219Dokument16 Seiten2598-Article Text-10075-1-10-20211219yusrinastitiNoch keine Bewertungen
- Nej MR A 2206573Dokument10 SeitenNej MR A 2206573yusrinastitiNoch keine Bewertungen
- Jamapediatrics Chang 2021 Oi 210031 1630088703.56331Dokument11 SeitenJamapediatrics Chang 2021 Oi 210031 1630088703.56331yusrinastitiNoch keine Bewertungen
- Kaplan 2021 Oi 211048 1637685010.99285Dokument13 SeitenKaplan 2021 Oi 211048 1637685010.99285yusrinastitiNoch keine Bewertungen
- Pediculosis of The Pubis: Images in Clinical MedicineDokument1 SeitePediculosis of The Pubis: Images in Clinical MedicineyusrinastitiNoch keine Bewertungen
- Eracs 1Dokument11 SeitenEracs 1Medissia Pasaribu0% (1)
- A Systematic Review of The Role of Hydrolyzed Infant Formulas in Allergy PreventionDokument7 SeitenA Systematic Review of The Role of Hydrolyzed Infant Formulas in Allergy PreventionyusrinastitiNoch keine Bewertungen
- Hypothesis Testing: Lab: Epidemiology and Biostatistics DepartmentDokument29 SeitenHypothesis Testing: Lab: Epidemiology and Biostatistics DepartmentyusrinastitiNoch keine Bewertungen
- PIIS2666524720301725Dokument10 SeitenPIIS2666524720301725baskoroNoch keine Bewertungen
- Eracs 1Dokument11 SeitenEracs 1Medissia Pasaribu0% (1)
- Logiq v5 - SpecificationDokument3 SeitenLogiq v5 - SpecificationserubimNoch keine Bewertungen
- Document 2Dokument7 SeitenDocument 2yusrinastitiNoch keine Bewertungen
- Document 2Dokument7 SeitenDocument 2yusrinastitiNoch keine Bewertungen
- Spesifikasi Produk GE Logiq E With 3 Probes Operation RoomDokument2 SeitenSpesifikasi Produk GE Logiq E With 3 Probes Operation RoomyusrinastitiNoch keine Bewertungen
- Logiq v5 - SpecificationDokument3 SeitenLogiq v5 - SpecificationserubimNoch keine Bewertungen
- Spesifikasi Produk GE Logiq E With 3 Probes Operation RoomDokument2 SeitenSpesifikasi Produk GE Logiq E With 3 Probes Operation RoomyusrinastitiNoch keine Bewertungen
- Logiq v5 - SpecificationDokument3 SeitenLogiq v5 - SpecificationserubimNoch keine Bewertungen
- 1stlab Hypothesis TestingDokument14 Seiten1stlab Hypothesis TestingyusrinastitiNoch keine Bewertungen
- Jamapediatrics Viner 2020 Oi 200071 1611604170.25358Dokument14 SeitenJamapediatrics Viner 2020 Oi 200071 1611604170.25358yusrinastitiNoch keine Bewertungen
- Paediatrica IndonesianaDokument6 SeitenPaediatrica IndonesianayusrinastitiNoch keine Bewertungen
- Growth ChartDokument4 SeitenGrowth ChartGenevieve Caecilia Linda KartonoNoch keine Bewertungen
- Rotavirus: Structure & Composition PathogenesisDokument4 SeitenRotavirus: Structure & Composition PathogenesisyusrinastitiNoch keine Bewertungen
- Transport of Oxygen and Carbon Dioxide in Blood and Tissue Fluids - 2Dokument2.618 SeitenTransport of Oxygen and Carbon Dioxide in Blood and Tissue Fluids - 2yusrinastitiNoch keine Bewertungen
- ARIA 07 at A Glance 1st Edition July 07Dokument8 SeitenARIA 07 at A Glance 1st Edition July 07amru_adjiNoch keine Bewertungen
- Pat Pat Alergic RhinitisDokument6 SeitenPat Pat Alergic RhinitisyusrinastitiNoch keine Bewertungen
- Orbit Arpita 111 (1) (New)Dokument31 SeitenOrbit Arpita 111 (1) (New)WALID HOSSAINNoch keine Bewertungen
- 4Dokument5 Seiten4Anonymous czrvb3h100% (3)
- Handout 1 - Body RegionsDokument3 SeitenHandout 1 - Body RegionsminionofcthulhuNoch keine Bewertungen
- Under The Guidance Of:: Dr. Sandeep Tandon Professor and Head of Dept. of PedodonticsDokument79 SeitenUnder The Guidance Of:: Dr. Sandeep Tandon Professor and Head of Dept. of PedodonticsMarivic DianoNoch keine Bewertungen
- Lec.11 Parotid RegionDokument7 SeitenLec.11 Parotid RegionothmanNoch keine Bewertungen
- Brain ImagesDokument24 SeitenBrain Imagesmemoumou27Noch keine Bewertungen
- Neet Wizz Bio Class 12Dokument89 SeitenNeet Wizz Bio Class 12Aarthi T. UNoch keine Bewertungen
- Autopsy Who Peforms The Autopsy?: Aut-+ Opsis Sight, Appearance - More at OpticDokument5 SeitenAutopsy Who Peforms The Autopsy?: Aut-+ Opsis Sight, Appearance - More at Opticmiguel gaquitNoch keine Bewertungen
- Connective TissueDokument62 SeitenConnective Tissuehnm mnhNoch keine Bewertungen
- BIO201L Lab 5 TissuesDokument12 SeitenBIO201L Lab 5 Tissuesmyra Thiong'oNoch keine Bewertungen
- Histology of Male Reproductive SystemDokument56 SeitenHistology of Male Reproductive SystemMuhammad Irfan100% (2)
- 478-Article Text-909-1-10-20210923Dokument10 Seiten478-Article Text-909-1-10-20210923Puspitadewi HensNoch keine Bewertungen
- Acute Phase ProteinsDokument3 SeitenAcute Phase ProteinswaihenyaNoch keine Bewertungen
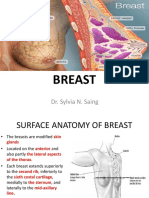
- Breast: Dr. Sylvia N. SaingDokument26 SeitenBreast: Dr. Sylvia N. SaingRichard 151289100% (1)
- Dictyosome: Modifying, and Packaging Proteins and Lipids Into Vesicles ForDokument11 SeitenDictyosome: Modifying, and Packaging Proteins and Lipids Into Vesicles ForASHFAQ AHMAD100% (1)
- 2 Saliva PhysiologyDokument20 Seiten2 Saliva PhysiologyvelangniNoch keine Bewertungen
- Skeletal SystemDokument1 SeiteSkeletal SystemEzekiel De GuzmanNoch keine Bewertungen
- Blood Transfusion Basic Concepts Blood Transfusion inDokument103 SeitenBlood Transfusion Basic Concepts Blood Transfusion iniahmad9Noch keine Bewertungen
- Mindmap Bio621 Chapter1Dokument3 SeitenMindmap Bio621 Chapter1MizahNoch keine Bewertungen
- Quiz 3Dokument3 SeitenQuiz 3Vannie MonderoNoch keine Bewertungen
- 10 Biology BitsDokument34 Seiten10 Biology BitsSuresh Raghava100% (1)
- 2 Abdominal and Pelvic AnatomyDokument47 Seiten2 Abdominal and Pelvic AnatomyNatalia VergaraNoch keine Bewertungen
- Blood Cell Morphology TutorialDokument176 SeitenBlood Cell Morphology TutorialCharles Jebb Belonio JuanitasNoch keine Bewertungen
- Legal MedicLegal MediciineDokument1 SeiteLegal MedicLegal MediciineJuan S. EnricoNoch keine Bewertungen
- SP 21Dokument1 SeiteSP 21ray72roNoch keine Bewertungen
- Grade 9 CardioDokument16 SeitenGrade 9 CardioJamoi Ray VedastoNoch keine Bewertungen
- Test Bank For Textbook of Diagnostic Microbiology 6th Edition MahonDokument13 SeitenTest Bank For Textbook of Diagnostic Microbiology 6th Edition MahonNorma Elliot97% (29)
- Pharmaceutical Sciences: ArticleinfoDokument8 SeitenPharmaceutical Sciences: ArticleinfoMario CastroNoch keine Bewertungen
- Test Bank Clinically Oriented Anatomy 7th Edition Moore Agur DalleyDokument9 SeitenTest Bank Clinically Oriented Anatomy 7th Edition Moore Agur Dalleyloganzv0meyer100% (11)
- Diagnostic Imaging - 11 - Regional Pathologies and Evaluation - Shoulder - Elbow - Wrist - Hand - Prof - Dr.i̇smet TAMERDokument34 SeitenDiagnostic Imaging - 11 - Regional Pathologies and Evaluation - Shoulder - Elbow - Wrist - Hand - Prof - Dr.i̇smet TAMERAly MssreNoch keine Bewertungen