Das könnte Ihnen auch gefallen
- Attracting Outstanding Students (Premedical and Medical) To A Career in Cardiothoracic SurgeryDokument3 SeitenAttracting Outstanding Students (Premedical and Medical) To A Career in Cardiothoracic Surgeryfluid_man_brazilNoch keine Bewertungen
- Benefit of Partial Right-Bilateral Internal Thoracic Artery Harvesting in Patients at Risk of Sternal Wound ComplicationsDokument5 SeitenBenefit of Partial Right-Bilateral Internal Thoracic Artery Harvesting in Patients at Risk of Sternal Wound Complicationsfluid_man_brazilNoch keine Bewertungen
- Tumor Necrosis Factor Alpha Influences The Inflammatory Response After Coronary SurgeryDokument6 SeitenTumor Necrosis Factor Alpha Influences The Inflammatory Response After Coronary Surgeryfluid_man_brazilNoch keine Bewertungen
- Wrapping of The Left Internal Thoracic Artery With An Expanded Polytetrafluoroethylene MembraneDokument3 SeitenWrapping of The Left Internal Thoracic Artery With An Expanded Polytetrafluoroethylene Membranefluid_man_brazilNoch keine Bewertungen
- Coapsys Mitral Annuloplasty For Chronic Functional Ischemic Mitral Regurgitation: 1-Year ResultsDokument5 SeitenCoapsys Mitral Annuloplasty For Chronic Functional Ischemic Mitral Regurgitation: 1-Year Resultsfluid_man_brazilNoch keine Bewertungen
- Comparative Effects of Tolazoline and Nitroprusside On Human Isolated Radial ArteryDokument7 SeitenComparative Effects of Tolazoline and Nitroprusside On Human Isolated Radial Arteryfluid_man_brazilNoch keine Bewertungen
- Effects of Papaverine and Glycerilnitrate-Verapamil Solution As Topical and Intraluminal Vasodilators For Internal Thoracic ArteryDokument5 SeitenEffects of Papaverine and Glycerilnitrate-Verapamil Solution As Topical and Intraluminal Vasodilators For Internal Thoracic Arteryfluid_man_brazilNoch keine Bewertungen
- Myocardial Thievery: The Coronary-Subclavian Steal SyndromeDokument7 SeitenMyocardial Thievery: The Coronary-Subclavian Steal Syndromefluid_man_brazilNoch keine Bewertungen
- Aprotinin Shows Both Hemostatic and Antithrombotic Effects During Off-Pump Coronary Artery Bypass GraftingDokument8 SeitenAprotinin Shows Both Hemostatic and Antithrombotic Effects During Off-Pump Coronary Artery Bypass Graftingfluid_man_brazilNoch keine Bewertungen
- Splanchnic Organ Injury During Coronary Surgery With or Without Cardiopulmonary Bypass: A Randomized, Controlled TrialDokument7 SeitenSplanchnic Organ Injury During Coronary Surgery With or Without Cardiopulmonary Bypass: A Randomized, Controlled Trialfluid_man_brazilNoch keine Bewertungen
- Off-Pump Myocardial Revascularization: Critical Analysis of 23 Years' Experience in 3,866 PatientsDokument5 SeitenOff-Pump Myocardial Revascularization: Critical Analysis of 23 Years' Experience in 3,866 Patientsfluid_man_brazilNoch keine Bewertungen
- Personal Communication - A Piece of Glass in The HeartDokument2 SeitenPersonal Communication - A Piece of Glass in The Heartfluid_man_brazilNoch keine Bewertungen
- How To Do It - Alternative Bi-Pectoral Muscle Flaps For Postoperative Sternotomy MediastinitisDokument2 SeitenHow To Do It - Alternative Bi-Pectoral Muscle Flaps For Postoperative Sternotomy Mediastinitisfluid_man_brazilNoch keine Bewertungen
- Long-Term Neurocognitive Function After Mechanical Aortic Valve ReplacementDokument5 SeitenLong-Term Neurocognitive Function After Mechanical Aortic Valve Replacementfluid_man_brazilNoch keine Bewertungen
- Physicians Assistants in Cardiothoracic Surgery: A 30-Year Experience in A University CenterDokument6 SeitenPhysicians Assistants in Cardiothoracic Surgery: A 30-Year Experience in A University Centerfluid_man_brazilNoch keine Bewertungen
- Effect of Aprotinin and Recombinant Variants On Platelet Protease-Activated Receptor 1 ActivationDokument6 SeitenEffect of Aprotinin and Recombinant Variants On Platelet Protease-Activated Receptor 1 Activationfluid_man_brazilNoch keine Bewertungen
- Intraoperative and Postoperative Evaluation of Cavitation in Mechanical Heart Valve PatientsDokument8 SeitenIntraoperative and Postoperative Evaluation of Cavitation in Mechanical Heart Valve Patientsfluid_man_brazilNoch keine Bewertungen
- (Radial String Sign) PDFDokument8 Seiten(Radial String Sign) PDFfluid_man_brazilNoch keine Bewertungen
- Portable Coronary Active Perfusion System For Off-Pump Coronary Artery Bypass GraftingDokument5 SeitenPortable Coronary Active Perfusion System For Off-Pump Coronary Artery Bypass Graftingfluid_man_brazilNoch keine Bewertungen
- Early Postoperative Anticoagulation After Mechanical Valve Replacement: A Systematic ReviewDokument12 SeitenEarly Postoperative Anticoagulation After Mechanical Valve Replacement: A Systematic Reviewfluid_man_brazilNoch keine Bewertungen
- Images - Multiple Penetrating Aortic UlcersDokument1 SeiteImages - Multiple Penetrating Aortic Ulcersfluid_man_brazilNoch keine Bewertungen
- The Society of Thoracic Surgeons/American Association For Thoracic Surgery Off-Pump Training ProgramDokument3 SeitenThe Society of Thoracic Surgeons/American Association For Thoracic Surgery Off-Pump Training Programfluid_man_brazilNoch keine Bewertungen
- Three-Dimensional Demonstration of The Collateral Circulation To The Artery of Adamkiewicz With 16-Row Multislice Computed TomographyDokument1 SeiteThree-Dimensional Demonstration of The Collateral Circulation To The Artery of Adamkiewicz With 16-Row Multislice Computed Tomographyfluid_man_brazilNoch keine Bewertungen
- Prevention of Postoperative Pericardial Adhesions With A Novel Regenerative Collagen SheetDokument8 SeitenPrevention of Postoperative Pericardial Adhesions With A Novel Regenerative Collagen Sheetfluid_man_brazilNoch keine Bewertungen
- Coronary Artery Revascularization After Chest Wall Reconstruction With Rectus Abdominis Myocutaneous FlapDokument4 SeitenCoronary Artery Revascularization After Chest Wall Reconstruction With Rectus Abdominis Myocutaneous Flapfluid_man_brazilNoch keine Bewertungen
- Effect of Aprotinin and Recombinant Variants On Platelet Protease-Activated Receptor 1 ActivationDokument6 SeitenEffect of Aprotinin and Recombinant Variants On Platelet Protease-Activated Receptor 1 Activationfluid_man_brazilNoch keine Bewertungen
- Invited Commentary - New Technology - New Perfusion System For Opcabg (Koshida Et Al)Dokument2 SeitenInvited Commentary - New Technology - New Perfusion System For Opcabg (Koshida Et Al)fluid_man_brazilNoch keine Bewertungen
- Invited Commentary - Preoperative WBC Link To Cabg Outcome (Newall Et Al)Dokument2 SeitenInvited Commentary - Preoperative WBC Link To Cabg Outcome (Newall Et Al)fluid_man_brazilNoch keine Bewertungen
- Invited Commentary - Aprotinin and Recombinant Variants (Day Et Al)Dokument1 SeiteInvited Commentary - Aprotinin and Recombinant Variants (Day Et Al)fluid_man_brazilNoch keine Bewertungen
- Invited Commentary - No Volume-Outcome Relationship For Opcabg (Plomondon Et Al)Dokument2 SeitenInvited Commentary - No Volume-Outcome Relationship For Opcabg (Plomondon Et Al)fluid_man_brazilNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Learner Cardiogenic Shock Secondary To Acute Myocardial InfarctionDokument5 SeitenLearner Cardiogenic Shock Secondary To Acute Myocardial InfarctionHailee YakishNoch keine Bewertungen
- Pocket Medicine High - Yield Board Review 2021Dokument298 SeitenPocket Medicine High - Yield Board Review 2021Omar Hassan83% (6)
- Prof Qaisar Khan TrialsDokument56 SeitenProf Qaisar Khan TrialsAsim NajamNoch keine Bewertungen
- Cardiology LastDokument101 SeitenCardiology Lastxaltra100% (1)
- Hypertension Diagnosis and ManagementDokument54 SeitenHypertension Diagnosis and ManagementdrsalilsidhqueNoch keine Bewertungen
- CV Ruby GuptaDokument4 SeitenCV Ruby GuptaAshish PatilNoch keine Bewertungen
- MidcabDokument7 SeitenMidcabNs PadiludinNoch keine Bewertungen
- Index To Volume 326Dokument45 SeitenIndex To Volume 326vhitaNoch keine Bewertungen
- PWKI Art 23954-10Dokument5 SeitenPWKI Art 23954-10Oeij Henri WijayaNoch keine Bewertungen
- Antiplatelet Therapy After Percutaneous Coronary InterventionDokument26 SeitenAntiplatelet Therapy After Percutaneous Coronary Interventionnazim bencharifNoch keine Bewertungen
- Merec Bulletin Vol15 No6Dokument4 SeitenMerec Bulletin Vol15 No6n4dn4dNoch keine Bewertungen
- Untitled DocumentDokument121 SeitenUntitled DocumentNur SanaaniNoch keine Bewertungen
- Cardiogenic Shock (BSN 3b)Dokument7 SeitenCardiogenic Shock (BSN 3b)Laurence ZernaNoch keine Bewertungen
- GROUP 3. Peripheral Arterial Occlusive Diseases PAODDokument73 SeitenGROUP 3. Peripheral Arterial Occlusive Diseases PAODLeslie Anne Oayan DaulayanNoch keine Bewertungen
- A Beginner's Guide To Interpreting Odds Ratios, Confidence Intervals and P-Values - Students 4 Best EvidenceDokument35 SeitenA Beginner's Guide To Interpreting Odds Ratios, Confidence Intervals and P-Values - Students 4 Best EvidenceABID ALINoch keine Bewertungen
- Loog Book Kardiologi Khusus-1Dokument8 SeitenLoog Book Kardiologi Khusus-1marjuwarNoch keine Bewertungen
- Panvascular Disease - Diagnosis and Management: SciencedirectDokument9 SeitenPanvascular Disease - Diagnosis and Management: SciencedirectAndikaputra Brahma WidiantoroNoch keine Bewertungen
- Study-Guide-2-Management-of-Patients-with-Cardiovacular-Copy For StudentsDokument17 SeitenStudy-Guide-2-Management-of-Patients-with-Cardiovacular-Copy For StudentsDan Dan ManaoisNoch keine Bewertungen
- Jakarta Cardiovascular Care Unit Network System OverviewDokument52 SeitenJakarta Cardiovascular Care Unit Network System OverviewekaNoch keine Bewertungen
- Atwood Management of Acute Coronary Syndrome 2022Dokument14 SeitenAtwood Management of Acute Coronary Syndrome 2022goten ramirezNoch keine Bewertungen
- Presentasi Ska PIT IDIDokument63 SeitenPresentasi Ska PIT IDIAyu WahyuniNoch keine Bewertungen
- Impact of Leukocytosis With Mortality and Bleeding in PCIDokument9 SeitenImpact of Leukocytosis With Mortality and Bleeding in PCIIntan Karnina PutriNoch keine Bewertungen
- Jama 2021 326 1840Dokument11 SeitenJama 2021 326 1840silviaNoch keine Bewertungen
- Evolving Concepts of The Vulnerable Atherosclerotic Plaque and TheDokument16 SeitenEvolving Concepts of The Vulnerable Atherosclerotic Plaque and TheKhánh Nguyễn NgọcNoch keine Bewertungen
- Coronary Artery Stent Thrombosis - Incidence and Risk Factors - UpToDateDokument21 SeitenCoronary Artery Stent Thrombosis - Incidence and Risk Factors - UpToDateCarlos Rubio LópezNoch keine Bewertungen
- Dual Antiplatelet Therapy Benefits for Prior MI PatientsDokument40 SeitenDual Antiplatelet Therapy Benefits for Prior MI PatientsKarren Taquiqui PleteNoch keine Bewertungen
- NCLEX Review of Integumentary, Eye, Ear, Respiratory TopicsDokument131 SeitenNCLEX Review of Integumentary, Eye, Ear, Respiratory TopicsRhika Mae ObraNoch keine Bewertungen
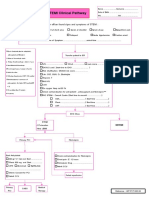
- STEMI Clinical PathwayDokument1 SeiteSTEMI Clinical PathwayKanoknun PisitpatcaragulNoch keine Bewertungen
- Nejm 09-04-2015Dokument107 SeitenNejm 09-04-2015Javier B GreenNoch keine Bewertungen
- Preventing perioperative myocardial ischemiaDokument7 SeitenPreventing perioperative myocardial ischemiaHalim SudonoNoch keine Bewertungen