Das könnte Ihnen auch gefallen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Dopamina Ira 2004Dokument8 SeitenDopamina Ira 2004Diego Bedon AscurraNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Estudio Dirofilariosis CaninaDokument5 SeitenEstudio Dirofilariosis CaninaDiego Bedon AscurraNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Acute Lyphocytic (Lymphoblastic) Leukemia Fallon, Nevada: Review and Recommendations of The Expert PanelDokument12 SeitenAcute Lyphocytic (Lymphoblastic) Leukemia Fallon, Nevada: Review and Recommendations of The Expert PanelDiego Bedon AscurraNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Tto Neuropatias AgudasDokument4 SeitenTto Neuropatias AgudasDiego Bedon AscurraNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Keith Edwards Score For Diagnosis of Tuberculosis. IJP.03Dokument3 SeitenKeith Edwards Score For Diagnosis of Tuberculosis. IJP.03Diego Bedon AscurraNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Dirofiliarosis Canina PDFDokument4 SeitenDirofiliarosis Canina PDFDiego Bedon AscurraNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- CHN ComputationDokument3 SeitenCHN ComputationRhyann AdvinculaNoch keine Bewertungen
- Community Medicine & RehabilitationDokument22 SeitenCommunity Medicine & Rehabilitationhfyfvgskfaj83% (6)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- WHSO Vaginal Discharge PosterDokument1 SeiteWHSO Vaginal Discharge PosterHervis FantiniNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- NCP PreeclampsiaDokument1 SeiteNCP PreeclampsiaMonica Cruz Dalida74% (23)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Pak301 GDB SolutionDokument2 SeitenPak301 GDB Solutionbc190407543 ALEENA BIBINoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Coccidiosis in Poultry - Laying HensDokument5 SeitenCoccidiosis in Poultry - Laying HensRobert AdrianNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
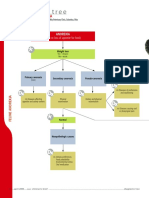
- Diagnostic Tree: Feline AnorexiaDokument2 SeitenDiagnostic Tree: Feline Anorexializ solanoNoch keine Bewertungen
- GiardiaDokument2 SeitenGiardiaKristal ForteNoch keine Bewertungen
- ColisepicemiaDokument8 SeitenColisepicemiajazz100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- HIV in South AfricaDokument17 SeitenHIV in South AfricaMadelineNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- PsychiatryDokument19 SeitenPsychiatryAnet Augustine AnetNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Diarrhea DehydrationDokument39 SeitenDiarrhea DehydrationBirhanu ShiferawNoch keine Bewertungen
- Inflamasi Akut Dan Kronik. 1Dokument40 SeitenInflamasi Akut Dan Kronik. 1shintaandiNoch keine Bewertungen
- 5 Things You Should Know About DysautonomiaDokument2 Seiten5 Things You Should Know About DysautonomianoomNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Atypical Manifestations of Acute Coronary Syndrome - Throat Discomfort: A Multi-Center Observational StudyDokument8 SeitenAtypical Manifestations of Acute Coronary Syndrome - Throat Discomfort: A Multi-Center Observational StudyYo MeNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- Explanation Text Covid-19Dokument2 SeitenExplanation Text Covid-19Mr ClawNoch keine Bewertungen
- Classification of Mental DisordersDokument4 SeitenClassification of Mental DisordersStuti Peter100% (1)
- Advisory On Leave CertificateDokument4 SeitenAdvisory On Leave CertificateSharavana KumarNoch keine Bewertungen
- 2.Post-Lecture Exam - General Pathology and Histopathologic TechniquesDokument10 Seiten2.Post-Lecture Exam - General Pathology and Histopathologic TechniqueslenvycahpdelusaNoch keine Bewertungen
- EASL Clinical Practice Guidelines: Autoimmune HepatitisDokument34 SeitenEASL Clinical Practice Guidelines: Autoimmune HepatitisBety Puma PauccaraNoch keine Bewertungen
- HIV Transmission FAQsDokument8 SeitenHIV Transmission FAQsbaradiNoch keine Bewertungen
- GNG Health Screening FormDokument2 SeitenGNG Health Screening FormGeorge NakojaNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- CPC Case 1Dokument9 SeitenCPC Case 1Astarte DimasalangNoch keine Bewertungen
- 200-Article Text-1119-1-10-20200603Dokument6 Seiten200-Article Text-1119-1-10-20200603miaNoch keine Bewertungen
- Oumme Rushaa Sairally FINAL5PAGEDokument6 SeitenOumme Rushaa Sairally FINAL5PAGERushaa SairallyNoch keine Bewertungen
- Hemophilia and Factor Assay PDFDokument17 SeitenHemophilia and Factor Assay PDFSumaira JunaidNoch keine Bewertungen
- AlopeciaDokument9 SeitenAlopeciaapi-502059670Noch keine Bewertungen
- ADC Part 1 - TG Keynotes II v1.0 PDFDokument17 SeitenADC Part 1 - TG Keynotes II v1.0 PDFDrSaif Ullah KhanNoch keine Bewertungen
- Simple EmergenciesDokument177 SeitenSimple Emergenciesharsh89100% (1)
- PODCAST #67 DR.B The Vet Show - Drh. Syavira EkdhiasmaraDokument26 SeitenPODCAST #67 DR.B The Vet Show - Drh. Syavira EkdhiasmaraLailatun NafisahNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)