Das könnte Ihnen auch gefallen
- Crime Scene Examination of Murder and Suicide CaseDokument8 SeitenCrime Scene Examination of Murder and Suicide CaseJonathan Dantas PessoaNoch keine Bewertungen
- Answer Key: Unit 1 Identity Unit 7 SuccessDokument1 SeiteAnswer Key: Unit 1 Identity Unit 7 Successflor-calderaro-62190% (2)
- Ows Banking PrepositionDokument6 SeitenOws Banking PrepositionNikita MallickNoch keine Bewertungen
- Unit 8 Test A Key: Gateway B2 Tests Unit 8 Tests/ Answer Keys A and BDokument1 SeiteUnit 8 Test A Key: Gateway B2 Tests Unit 8 Tests/ Answer Keys A and BЧерт Помойный100% (2)
- Problems Set 1Dokument10 SeitenProblems Set 1Tina WalizadehNoch keine Bewertungen
- Roger ArkwrightDokument2 SeitenRoger ArkwrightAlex Polanco-HarperNoch keine Bewertungen
- The Effect of Hemisphere Specific Remediation Strategies On The Academic Performance Outcome of Children With ADD/ADHDDokument10 SeitenThe Effect of Hemisphere Specific Remediation Strategies On The Academic Performance Outcome of Children With ADD/ADHDEderNoch keine Bewertungen
- مراحل النمو عند الطفل و المراهقDokument40 Seitenمراحل النمو عند الطفل و المراهقWalid IchaouiNoch keine Bewertungen
- English Handouts - English-Error Location-Phrasal ReplacementDokument12 SeitenEnglish Handouts - English-Error Location-Phrasal ReplacementtaraNoch keine Bewertungen
- Progress ReportDokument15 SeitenProgress ReportBaby Lyn De MesaNoch keine Bewertungen
- 2003 Texas Hunting Accidents AnalysisDokument12 Seiten2003 Texas Hunting Accidents AnalysisTheo BlevinsNoch keine Bewertungen
- Astrological Research Jack The RipperDokument46 SeitenAstrological Research Jack The RipperlinchiNoch keine Bewertungen
- No. 10-3-00796-4 Scheree Winters V Nicholas WintersDokument422 SeitenNo. 10-3-00796-4 Scheree Winters V Nicholas WintersV Freitas LegalNoch keine Bewertungen
- Performance Task in Statistics and Probability: PASSED BY: Honeygail N. Fortaleza 11-St. Vincent de PaulDokument4 SeitenPerformance Task in Statistics and Probability: PASSED BY: Honeygail N. Fortaleza 11-St. Vincent de PaulHoneygail FortalezaNoch keine Bewertungen
- Minyak Biji KaretDokument4 SeitenMinyak Biji Karetwildan pratamaNoch keine Bewertungen
- 117Dokument6 Seiten117renurathoreNoch keine Bewertungen
- Grade 7: First Term Examination - 2015Dokument1 SeiteGrade 7: First Term Examination - 2015Fathima FazmilaNoch keine Bewertungen
- E4 EoB MOCKDokument4 SeitenE4 EoB MOCKAhmedElhuseiniNoch keine Bewertungen
- Deck DatabaseDokument8 SeitenDeck DatabaseLanaNoch keine Bewertungen
- Answers To Exercises: Unit 1Dokument5 SeitenAnswers To Exercises: Unit 1Amjad MemonNoch keine Bewertungen
- p4 English Ca1 2010 ChijDokument17 Seitenp4 English Ca1 2010 Chijaiwen_wong2428Noch keine Bewertungen
- Crusader: Table 1-1: The Crusader Hit Die: d10Dokument2 SeitenCrusader: Table 1-1: The Crusader Hit Die: d10roddyNoch keine Bewertungen
- Interviews Extra: Intermediate Answer KeyDokument2 SeitenInterviews Extra: Intermediate Answer Keynadin nNoch keine Bewertungen
- Screenshot 2023-09-22 at 00.53.52Dokument1 SeiteScreenshot 2023-09-22 at 00.53.52kyfkn5xqq4Noch keine Bewertungen
- Ayuda PedagogicaDokument1 SeiteAyuda PedagogicaAnderson RojasNoch keine Bewertungen
- Restday Schedule: Sidekick Force Security AgencyDokument1 SeiteRestday Schedule: Sidekick Force Security AgencyAnfernee Ramzel Castro BuenavistaNoch keine Bewertungen
- CH 5 Principles of Inheritance and Variations - Sundar - Notes - Final-22.08.21 - Part Ii.Dokument20 SeitenCH 5 Principles of Inheritance and Variations - Sundar - Notes - Final-22.08.21 - Part Ii.priyamprakash0107Noch keine Bewertungen
- Socheolas DisgraceDokument19 SeitenSocheolas DisgraceJacques AswadNoch keine Bewertungen
- Lelm206 PDFDokument5 SeitenLelm206 PDFPrakhar VermaNoch keine Bewertungen
- Exercise 8: ProcedureDokument5 SeitenExercise 8: Proceduresuryansh bhantiNoch keine Bewertungen
- The Crew Deep Sea Mission CardsDokument6 SeitenThe Crew Deep Sea Mission CardsFrederico Morgado100% (1)
- Lelm 206Dokument5 SeitenLelm 206Kritika MishraNoch keine Bewertungen
- Grade 10 - Talaan NG PagbasaDokument8 SeitenGrade 10 - Talaan NG PagbasaMarietta ArgaoNoch keine Bewertungen
- Speakout 2nd Edition Intermediate BBC Interviews Extra WorksheetsDokument36 SeitenSpeakout 2nd Edition Intermediate BBC Interviews Extra WorksheetsVlada isay80% (5)
- The History of English in 10 Minutes - Sub ENGDokument20 SeitenThe History of English in 10 Minutes - Sub ENGJelena JelenaNoch keine Bewertungen
- Ampero II Stage - Drum Rhythm List - EN - Firmware V1.0.4.1706583962737Dokument4 SeitenAmpero II Stage - Drum Rhythm List - EN - Firmware V1.0.4.1706583962737Виталий ИвановNoch keine Bewertungen
- Citizens Arrest LawDokument3 SeitenCitizens Arrest LawMark RossNoch keine Bewertungen
- English Foundation BatchDokument4 SeitenEnglish Foundation BatchAshutosh RajNoch keine Bewertungen
- Betar Preference AssessmentDokument9 SeitenBetar Preference Assessmentapi-391858777Noch keine Bewertungen
- 57 at PHIDokument4 Seiten57 at PHIascomakNoch keine Bewertungen
- 100 Excellent DILR Sets Compiled PDF File Part 1Dokument41 Seiten100 Excellent DILR Sets Compiled PDF File Part 1anvitNoch keine Bewertungen
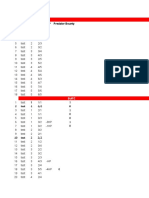
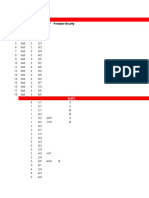
- # Name Stats Cost HP Predator Bounty: Vanilla Baby - F CreaturesDokument8 Seiten# Name Stats Cost HP Predator Bounty: Vanilla Baby - F CreaturesLanaNoch keine Bewertungen
- Are Human Beings Getting Smarter?Dokument11 SeitenAre Human Beings Getting Smarter?English EnglishNoch keine Bewertungen
- McCauley USMuslims911 2009Dokument14 SeitenMcCauley USMuslims911 2009Ananda Fathiyyah UtamiNoch keine Bewertungen
- Probability Assignment NewDokument32 SeitenProbability Assignment NewhareshtankNoch keine Bewertungen
- Sample Balane Legitimes Quiz PDFDokument1 SeiteSample Balane Legitimes Quiz PDFJames Francis VillanuevaNoch keine Bewertungen
- 4 - 08-10-2022 - 16-54-31 - MBA 5-Year (Integrated)Dokument55 Seiten4 - 08-10-2022 - 16-54-31 - MBA 5-Year (Integrated)Sneha MaliyaNoch keine Bewertungen
- LI L1 MidYear EndYear Tests AnswersDokument2 SeitenLI L1 MidYear EndYear Tests AnswersHenry GsNoch keine Bewertungen
- SO UI Tests KeyDokument14 SeitenSO UI Tests Keyboj210462% (29)
- Together kl4 Standard Tests Answer KeyDokument12 SeitenTogether kl4 Standard Tests Answer KeyRufi StreamNoch keine Bewertungen
- English Scheme of Work Year 3 2012Dokument18 SeitenEnglish Scheme of Work Year 3 2012Anonymous xGCiF6oNoch keine Bewertungen
- KooBits - Engaging The Digital KidsDokument18 SeitenKooBits - Engaging The Digital KidsNiladri ChatterjeeNoch keine Bewertungen
- SteelDokument3 SeitenSteelS. BalcrickNoch keine Bewertungen
- CPA Study Material Book ForDokument31 SeitenCPA Study Material Book ForParth SavaliyaNoch keine Bewertungen
- Bahan Referat 3 CDCDokument6 SeitenBahan Referat 3 CDCLeviPerdaNaNoch keine Bewertungen
- Keakuratan Kode Diagnosis Stroke Di Rumah Sakit Islam Amal Sehat SragenDokument9 SeitenKeakuratan Kode Diagnosis Stroke Di Rumah Sakit Islam Amal Sehat SragenLeviPerdaNaNoch keine Bewertungen
- KODE ICD 10 - Anak & ObgynDokument1 SeiteKODE ICD 10 - Anak & ObgynLeviPerdaNaNoch keine Bewertungen
- Posttraumatic Stress Disorder (PTSD)Dokument1 SeitePosttraumatic Stress Disorder (PTSD)LeviPerdaNaNoch keine Bewertungen
- Faring It IsDokument41 SeitenFaring It IsLeviPerdaNaNoch keine Bewertungen
- Judul, Lembar Pengesahan, Daftar Isi Dan Abstrak (Rizkita Ria)Dokument13 SeitenJudul, Lembar Pengesahan, Daftar Isi Dan Abstrak (Rizkita Ria)LeviPerdaNaNoch keine Bewertungen
- KODE ICD 10 - Anak & ObgynDokument1 SeiteKODE ICD 10 - Anak & ObgynLeviPerdaNaNoch keine Bewertungen
- KODE ICD 10 - Anak & ObgynDokument1 SeiteKODE ICD 10 - Anak & ObgynLeviPerdaNaNoch keine Bewertungen
- Name: Kartikeya Thadani Reg No.: 19bma0029Dokument4 SeitenName: Kartikeya Thadani Reg No.: 19bma0029Kartikeya ThadaniNoch keine Bewertungen
- Organizational Behavior (Perception & Individual Decision Making)Dokument23 SeitenOrganizational Behavior (Perception & Individual Decision Making)Irfan ur RehmanNoch keine Bewertungen
- Meike SchalkDokument212 SeitenMeike SchalkPetra BoulescuNoch keine Bewertungen
- Ulangan Harian Lesson 4 Kls 6Dokument3 SeitenUlangan Harian Lesson 4 Kls 6Megadevegaalgifari Minozholic Full100% (2)
- EMI - Module 1 Downloadable Packet - Fall 2021Dokument34 SeitenEMI - Module 1 Downloadable Packet - Fall 2021Eucarlos MartinsNoch keine Bewertungen
- KalamDokument8 SeitenKalamRohitKumarSahuNoch keine Bewertungen
- Language Analysis - GRAMMAR/FUNCTIONS Context Anticipated ProblemsDokument2 SeitenLanguage Analysis - GRAMMAR/FUNCTIONS Context Anticipated Problemsshru_edgyNoch keine Bewertungen
- Nutrition and Metabolism: (Carbohydrates, Lipids, Protein)Dokument37 SeitenNutrition and Metabolism: (Carbohydrates, Lipids, Protein)Trishia BonNoch keine Bewertungen
- Medicidefamilie 2011Dokument6 SeitenMedicidefamilie 2011Mesaros AlexandruNoch keine Bewertungen
- Genomics - FAODokument184 SeitenGenomics - FAODennis AdjeiNoch keine Bewertungen
- MCS 033 NotesDokument7 SeitenMCS 033 NotesAshikNoch keine Bewertungen
- Europe Landmarks Reading Comprehension Activity - Ver - 1Dokument12 SeitenEurope Landmarks Reading Comprehension Activity - Ver - 1Plamenna Pavlova100% (1)
- Panera Bread Company: Case AnalysisDokument9 SeitenPanera Bread Company: Case AnalysisJaclyn Novak FreemanNoch keine Bewertungen
- List of Vocabulary C2Dokument43 SeitenList of Vocabulary C2Lina LilyNoch keine Bewertungen
- Pediatric ECG Survival Guide - 2nd - May 2019Dokument27 SeitenPediatric ECG Survival Guide - 2nd - May 2019Marcos Chusin MontesdeocaNoch keine Bewertungen
- Abramson, Glenda (Ed.) - Oxford Book of Hebrew Short Stories (Oxford, 1996) PDFDokument424 SeitenAbramson, Glenda (Ed.) - Oxford Book of Hebrew Short Stories (Oxford, 1996) PDFptalus100% (2)
- Logic of English - Spelling Rules PDFDokument3 SeitenLogic of English - Spelling Rules PDFRavinder Kumar80% (15)
- Recent Cases On Minority RightsDokument10 SeitenRecent Cases On Minority RightsHarsh DixitNoch keine Bewertungen
- 1634313583!Dokument24 Seiten1634313583!Joseph Sanchez TalusigNoch keine Bewertungen
- Apple Festival Program 2017Dokument3 SeitenApple Festival Program 2017Elizabeth JanneyNoch keine Bewertungen
- Account Intel Sample 3Dokument28 SeitenAccount Intel Sample 3CI SamplesNoch keine Bewertungen
- Grammar For TOEFLDokument23 SeitenGrammar For TOEFLClaudia Alejandra B0% (1)
- Alice (Alice's Adventures in Wonderland)Dokument11 SeitenAlice (Alice's Adventures in Wonderland)Oğuz KarayemişNoch keine Bewertungen
- Grossman 1972 Health CapitalDokument33 SeitenGrossman 1972 Health CapitalLeonardo SimonciniNoch keine Bewertungen
- DMSCO Log Book Vol.25 1947Dokument49 SeitenDMSCO Log Book Vol.25 1947Des Moines University Archives and Rare Book RoomNoch keine Bewertungen
- Sample Behavioral Interview QuestionsDokument3 SeitenSample Behavioral Interview QuestionssanthoshvNoch keine Bewertungen
- Wetlands Denote Perennial Water Bodies That Originate From Underground Sources of Water or RainsDokument3 SeitenWetlands Denote Perennial Water Bodies That Originate From Underground Sources of Water or RainsManish thapaNoch keine Bewertungen
- Physiology PharmacologyDokument126 SeitenPhysiology PharmacologyuneedlesNoch keine Bewertungen
- LAW OF ContractDokument1 SeiteLAW OF ContractKhurshid Manzoor Malik50% (2)
- Morocco Top ScientistsDokument358 SeitenMorocco Top Scientistsa.drioicheNoch keine Bewertungen