Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Cognitive, Perceptual, and Motor Bases of Early Language and Speech (Mr. Fachri)Dokument2 SeitenCognitive, Perceptual, and Motor Bases of Early Language and Speech (Mr. Fachri)Mukhlisul Ibad SatriatamaNoch keine Bewertungen
- Overcoming: The Source of FearDokument6 SeitenOvercoming: The Source of FearSai BhargavNoch keine Bewertungen
- Foreword To 'Carl Rogers - The Quiet Revolutionary, An Oral History'Dokument8 SeitenForeword To 'Carl Rogers - The Quiet Revolutionary, An Oral History'rebellin100% (1)
- Understanding The Self - FINAL EXAM Reviewer (AutoRecovered)Dokument7 SeitenUnderstanding The Self - FINAL EXAM Reviewer (AutoRecovered)Yasmin Pheebie BeltranNoch keine Bewertungen
- Lesson 2.2 - Psychological Foundations of Curriculum DevelopmentDokument29 SeitenLesson 2.2 - Psychological Foundations of Curriculum DevelopmentDarryl BarrientosNoch keine Bewertungen
- Facial Expression Recognition Using Convolutional Neural Networks: State of The ArtDokument6 SeitenFacial Expression Recognition Using Convolutional Neural Networks: State of The Arttrương xuân thànhNoch keine Bewertungen
- Neuro-Fuzzy Systems and Their Applications: BogdanDokument15 SeitenNeuro-Fuzzy Systems and Their Applications: BogdanYk1Noch keine Bewertungen
- Mindfulness Based Stress ReductionDokument1 SeiteMindfulness Based Stress ReductionJodiMBrownNoch keine Bewertungen
- Brezan Stukovnik Vodusek - NFB, EEG CORRELATES OF HYPNOSIS, ROGLA CONGRESS ON PSYCHOTHERAPY AND NEUROSCIENCEDokument2 SeitenBrezan Stukovnik Vodusek - NFB, EEG CORRELATES OF HYPNOSIS, ROGLA CONGRESS ON PSYCHOTHERAPY AND NEUROSCIENCEsimon brežanNoch keine Bewertungen
- Electromyography & It's Application in OrthodonticsDokument22 SeitenElectromyography & It's Application in Orthodonticsprasadgayake100% (1)
- Mindfulness and Urges: The Hungry GhostDokument31 SeitenMindfulness and Urges: The Hungry GhostSugiharto GunawanNoch keine Bewertungen
- Imagenes Psicologia FisiologicaDokument18 SeitenImagenes Psicologia FisiologicaMayra VillegasNoch keine Bewertungen
- AUNLP - All Course Competencies & SkillsDokument8 SeitenAUNLP - All Course Competencies & SkillsSteve-39Noch keine Bewertungen
- National Geographic - May (2010) (Malestrom)Dokument81 SeitenNational Geographic - May (2010) (Malestrom)GNoch keine Bewertungen
- Central Coherence in Adults With A High-Functioning Autism Spectrum Disorder. in A Search For A Non-Self-Reporting Screening ToolDokument8 SeitenCentral Coherence in Adults With A High-Functioning Autism Spectrum Disorder. in A Search For A Non-Self-Reporting Screening ToolNp Luis Gómez0% (1)
- Applied Psychology II PDFDokument4 SeitenApplied Psychology II PDFSaba Khalid100% (1)
- Stangor2 - 1 TIF Ch01Dokument29 SeitenStangor2 - 1 TIF Ch01Chinonso Ahuna100% (1)
- Review Inside OutDokument1 SeiteReview Inside OutwibiNoch keine Bewertungen
- AI Lec1Dokument16 SeitenAI Lec1CG Art VfxNoch keine Bewertungen
- Ankur Bhaumik 18895 UB201L Neurobiology Assignment Lab 1 and 2 PDFDokument4 SeitenAnkur Bhaumik 18895 UB201L Neurobiology Assignment Lab 1 and 2 PDFAnkur BhaumikNoch keine Bewertungen
- Independent Variable in Psychology ExperimentsDokument9 SeitenIndependent Variable in Psychology ExperimentsLAliNoch keine Bewertungen
- ABIOG, Perceptual Learning Style PreferenceDokument3 SeitenABIOG, Perceptual Learning Style Preferenceashley abiogNoch keine Bewertungen
- Communicative FunctionsmeansDokument4 SeitenCommunicative FunctionsmeansmedotoNoch keine Bewertungen
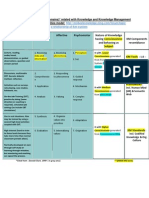
- Bloom's Taxonomy (Learning Domains) Related With Knowledge and Knowledge Management (KM)Dokument1 SeiteBloom's Taxonomy (Learning Domains) Related With Knowledge and Knowledge Management (KM)Md SantoNoch keine Bewertungen
- Organisational Behaviour-Jan 2006 To July-2008Dokument3 SeitenOrganisational Behaviour-Jan 2006 To July-2008Raj KamalNoch keine Bewertungen
- Brainsci 10 00502 v2Dokument18 SeitenBrainsci 10 00502 v2Serque777Noch keine Bewertungen
- Coatnet: Marrying Convolution and Attention For All Data SizesDokument18 SeitenCoatnet: Marrying Convolution and Attention For All Data SizesLịch Nguyễn ĐăngNoch keine Bewertungen
- Outdoor Plays Effect On Childhood DevelopmentDokument11 SeitenOutdoor Plays Effect On Childhood DevelopmentRobert LavarnwayNoch keine Bewertungen
- Multiple Intelligences TestDokument2 SeitenMultiple Intelligences TestRodrigo GonzálezNoch keine Bewertungen
- Revisiting Snodgrass and Vanderwart's Object Databank: Color and Texture Improve Object RecognitionDokument18 SeitenRevisiting Snodgrass and Vanderwart's Object Databank: Color and Texture Improve Object RecognitionMaca Martínez-CuitiñoNoch keine Bewertungen