Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Overview of The Nervous System Overview of The Nervous SystemDokument21 SeitenOverview of The Nervous System Overview of The Nervous Systemarlinie100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Basicanatomyand Physiologyofpain Pathways: Sarah Bourne,, Andre G. Machado,, Sean J. NagelDokument10 SeitenBasicanatomyand Physiologyofpain Pathways: Sarah Bourne,, Andre G. Machado,, Sean J. NagelarlinieNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Intervertebral Disc TissuesDokument30 SeitenIntervertebral Disc TissuesarlinieNoch keine Bewertungen
- Intervertebral Disc)Dokument28 SeitenIntervertebral Disc)arlinieNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Central Vertigo PDFDokument6 SeitenCentral Vertigo PDFarlinieNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
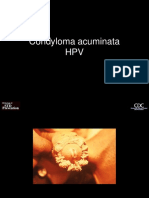
- Condyloma AcuminataDokument6 SeitenCondyloma AcuminataarlinieNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Pharmacology of Crystalloids and ColloidsDokument16 SeitenPharmacology of Crystalloids and ColloidsarlinieNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Birth InjuriesDokument17 SeitenBirth InjuriesarlinieNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Pharmacology of Crystalloids and ColloidsDokument16 SeitenPharmacology of Crystalloids and ColloidsarlinieNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Total Revision For The Primary Frca 2nd EditionDokument53 SeitenTotal Revision For The Primary Frca 2nd Editionizwan taufikNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Treatment in Dental Practice of The Patient Receiving Anticoagulation Therapy PDFDokument7 SeitenTreatment in Dental Practice of The Patient Receiving Anticoagulation Therapy PDFJorge AlvaradoNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Stroke Research Review Issue 27 PDFDokument4 SeitenStroke Research Review Issue 27 PDFGhaidaa AlarajNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Vitamin KDokument17 SeitenVitamin KRuth linayantiNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
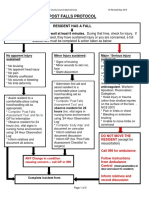
- 4-Hampshire Falls ProtocolDokument5 Seiten4-Hampshire Falls ProtocolsheenaNoch keine Bewertungen
- Chapter 2 Board ExamDokument20 SeitenChapter 2 Board ExamAljohn Galang100% (2)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Patient Counseling PresentationDokument40 SeitenPatient Counseling PresentationMuhammad Umar Farooqi100% (5)
- Seminar - Hemorrhage 25-06-2020Dokument75 SeitenSeminar - Hemorrhage 25-06-2020Chandra dimpleNoch keine Bewertungen
- Ix StrokeDokument6 SeitenIx StrokeWayne MacrohonNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Cardiovascular Pathology: Rolf F. Barth, Sergey V. Brodsky, Miroljub RuzicDokument4 SeitenCardiovascular Pathology: Rolf F. Barth, Sergey V. Brodsky, Miroljub RuzicSoporte CeffanNoch keine Bewertungen
- Past Papers 601 800 1Dokument50 SeitenPast Papers 601 800 1nayeemmajed100% (5)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Switching To-From AnticoagulantsDokument8 SeitenSwitching To-From AnticoagulantsAlex AlxNoch keine Bewertungen
- Avoiding Drug InteractionsDokument4 SeitenAvoiding Drug InteractionssakuraleeshaoranNoch keine Bewertungen
- Coronary Atery Disease-Htn-Thrombo QuestionsDokument38 SeitenCoronary Atery Disease-Htn-Thrombo Questionssrivari sriniNoch keine Bewertungen
- Watchman PresentationDokument179 SeitenWatchman PresentationJackie OliveNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Crozer Manual - Second EditionDokument219 SeitenCrozer Manual - Second EditionsgangamanNoch keine Bewertungen
- Clotting Factors Blood Liver Prothrombin TimeDokument2 SeitenClotting Factors Blood Liver Prothrombin TimeArindah Dinar SafitriNoch keine Bewertungen
- Periprocedural Anticoagulation Guidelines - UKDokument14 SeitenPeriprocedural Anticoagulation Guidelines - UKjoshNoch keine Bewertungen
- Thromboembolic Disease PDFDokument5 SeitenThromboembolic Disease PDFBáĦẳá Y. Ẳl-mársǾúmiNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Patient Safety GoalsDokument59 SeitenPatient Safety GoalsHarby Ongbay Abellanosa100% (1)
- Health Benefits of PoulticesDokument7 SeitenHealth Benefits of PoulticesEduard50% (2)
- PESTICIDESDokument65 SeitenPESTICIDESMuhammad Masoom AkhtarNoch keine Bewertungen
- Atrial Fibrillation Management: Mini-LectureDokument21 SeitenAtrial Fibrillation Management: Mini-LectureFahmi RaziNoch keine Bewertungen
- Plab Emergency Medicine CompleteDokument141 SeitenPlab Emergency Medicine CompleteSyedKashifAli100% (1)
- Heparin - ClinicalKeyDokument85 SeitenHeparin - ClinicalKeydayannaNoch keine Bewertungen
- RevisionDokument17 SeitenRevisionMatt RenaudNoch keine Bewertungen
- MedicationsDokument30 SeitenMedicationsvamshidhNoch keine Bewertungen
- Coagulation Disorders in ICUDokument72 SeitenCoagulation Disorders in ICUMadhusudan H C Gowda100% (1)
- PRADAXA: Dosing Guide: Starting Patients On PRADAXADokument2 SeitenPRADAXA: Dosing Guide: Starting Patients On PRADAXAPapp Szodorai BeátaNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Preoperative Testing and Medication ManagementDokument27 SeitenPreoperative Testing and Medication ManagementWidya JelitaNoch keine Bewertungen