Das könnte Ihnen auch gefallen
- Psychological Disorders Chapter OutlineDokument13 SeitenPsychological Disorders Chapter OutlineCameron PhillipsNoch keine Bewertungen
- I VC GuidelinesDokument22 SeitenI VC Guidelinesganesha trengginasNoch keine Bewertungen
- Brain Abscess in Pediatric AgeDokument12 SeitenBrain Abscess in Pediatric AgeKatrina San GilNoch keine Bewertungen
- Atls Pre Test SolvedDokument18 SeitenAtls Pre Test SolvedDr.Mukesh KumarNoch keine Bewertungen
- TB Meningitis Lancet 2022Dokument15 SeitenTB Meningitis Lancet 2022stephanie bojorquezNoch keine Bewertungen
- Brain AbscessDokument13 SeitenBrain Abscesskashim123Noch keine Bewertungen
- Brain Abcess Journal 2Dokument4 SeitenBrain Abcess Journal 2ansyemomoleNoch keine Bewertungen
- Absceso CerebralDokument8 SeitenAbsceso Cerebralgiseladelarosa2006Noch keine Bewertungen
- Brain AbscessDokument17 SeitenBrain AbscessLaura Fernanda Soto BNoch keine Bewertungen
- Bacterial Infections of the Nervous SystemDokument2 SeitenBacterial Infections of the Nervous SystemRocio LedesmaNoch keine Bewertungen
- Do Brain Abscesses Have A Higher Incidence of Odontogenic Origin Than Previously Thought?Dokument7 SeitenDo Brain Abscesses Have A Higher Incidence of Odontogenic Origin Than Previously Thought?Haytham JamilNoch keine Bewertungen
- (10920684 - Neurosurgical Focus) Pyogenic Brain AbscessDokument10 Seiten(10920684 - Neurosurgical Focus) Pyogenic Brain AbscesschiquitaputriNoch keine Bewertungen
- Bacterial Brain AbscessDokument16 SeitenBacterial Brain AbscessYunike DindaNoch keine Bewertungen
- Brain AbcesDokument6 SeitenBrain AbcesGintar Isnu WardoyoNoch keine Bewertungen
- 1 s2.0 S0165587617302975 Main PDFDokument4 Seiten1 s2.0 S0165587617302975 Main PDFAchmad YunusNoch keine Bewertungen
- Absceso Cerebral en Rn Asociado a Infeccion UmbilicalDokument5 SeitenAbsceso Cerebral en Rn Asociado a Infeccion UmbilicalAbrahamKatimeNoch keine Bewertungen
- Bacterial Brain Abscess: Epidemiology, Diagnosis and TreatmentDokument9 SeitenBacterial Brain Abscess: Epidemiology, Diagnosis and TreatmentDayuKurnia DewantiNoch keine Bewertungen
- Bacterial Brain Abscess: Kevin Patel, MD, and David B. Clifford, MDDokument9 SeitenBacterial Brain Abscess: Kevin Patel, MD, and David B. Clifford, MDRiskalFebriaryNoch keine Bewertungen
- Brain Abscess: State-Of-The-Art Clinical ArticleDokument17 SeitenBrain Abscess: State-Of-The-Art Clinical ArticleAwais KhanNoch keine Bewertungen
- Bacterial Brain Abscess: An Outline For Diagnosis and ManagementDokument10 SeitenBacterial Brain Abscess: An Outline For Diagnosis and ManagementWIWI HRNoch keine Bewertungen
- Current Epidemiological Trends of Brain Abscess: A Clinicopathological StudyDokument9 SeitenCurrent Epidemiological Trends of Brain Abscess: A Clinicopathological StudyNur Fadhilah KusnadiNoch keine Bewertungen
- Putt's Puffy TumorDokument6 SeitenPutt's Puffy Tumorkeith isamelNoch keine Bewertungen
- Pyogenic Brain Abscess A 15 Year SurveryDokument10 SeitenPyogenic Brain Abscess A 15 Year SurverySilvia RoseNoch keine Bewertungen
- Brain Abscess: State-Of-The-Art Clinical ArticleDokument17 SeitenBrain Abscess: State-Of-The-Art Clinical ArticleIqbal AbdillahNoch keine Bewertungen
- Cerebral Abscesses Imaging A Practical ApproachDokument14 SeitenCerebral Abscesses Imaging A Practical Approachhasbi.alginaaNoch keine Bewertungen
- Bacterial Brain AbscessDokument10 SeitenBacterial Brain AbscessTheroux delucNoch keine Bewertungen
- Absceso Cerebral 99Dokument7 SeitenAbsceso Cerebral 99shen_siiNoch keine Bewertungen
- (10920684 - Neurosurgical Focus) Intracranial Infections - Lessons Learned From 52 Surgically Treated CasesDokument8 Seiten(10920684 - Neurosurgical Focus) Intracranial Infections - Lessons Learned From 52 Surgically Treated CasesIsmail MuhammadNoch keine Bewertungen
- Community-Acquired Bacterial Meningitis in Adults: Review ArticleDokument10 SeitenCommunity-Acquired Bacterial Meningitis in Adults: Review ArticleÁlvaro NBNoch keine Bewertungen
- Bacterial Brain Abscess: Journal ReadingDokument22 SeitenBacterial Brain Abscess: Journal ReadingdinarNoch keine Bewertungen
- Review: PathogenesisDokument15 SeitenReview: PathogenesispatarikuNoch keine Bewertungen
- Focus: Intracranial Infections: Lessons Learned From 52 Surgically Treated CasesDokument8 SeitenFocus: Intracranial Infections: Lessons Learned From 52 Surgically Treated Casesjena maraNoch keine Bewertungen
- Alwahab2017 Article OccipitalMeningoencephaloceleC PDFDokument4 SeitenAlwahab2017 Article OccipitalMeningoencephaloceleC PDFOvamelia JulioNoch keine Bewertungen
- Nej MR A 1216008Dokument11 SeitenNej MR A 1216008guillosarahNoch keine Bewertungen
- Neuroinfeccion en UrgenciasDokument26 SeitenNeuroinfeccion en UrgenciasFabio RBlNoch keine Bewertungen
- Review Article: Recent Advances in Childhood Brain TumoursDokument10 SeitenReview Article: Recent Advances in Childhood Brain Tumoursjosue_wigNoch keine Bewertungen
- Bacterial Meningitis in ChildrenDokument10 SeitenBacterial Meningitis in ChildrenAnny AryanyNoch keine Bewertungen
- Brain Abscess Diagnosis and Management GuideDokument7 SeitenBrain Abscess Diagnosis and Management GuideNadia OktarinaNoch keine Bewertungen
- Meningitis, AAFPDokument8 SeitenMeningitis, AAFPCarlos Danilo Noroña CNoch keine Bewertungen
- Prospective Study of Intracranial Space Occupying Lesions in Children in Correlation With C.T. ScanDokument8 SeitenProspective Study of Intracranial Space Occupying Lesions in Children in Correlation With C.T. Scannurulanisa0703Noch keine Bewertungen
- 1gorgan BrainAbcessesDokument8 Seiten1gorgan BrainAbcessesGema Rizki PratamaNoch keine Bewertungen
- Ophthalmological Findings in Children With EncephalitisDokument8 SeitenOphthalmological Findings in Children With EncephalitisSabila TasyakurNoch keine Bewertungen
- JNeurosciRuralPract 2013 4 5 67 116472Dokument17 SeitenJNeurosciRuralPract 2013 4 5 67 116472Silvia EmyNoch keine Bewertungen
- The Management of Intracranial AbscessesDokument3 SeitenThe Management of Intracranial AbscessesDio AlexanderNoch keine Bewertungen
- Meningitis Thesis StatementDokument9 SeitenMeningitis Thesis StatementMichele Thomas100% (1)
- Abses Cerebri 1Dokument8 SeitenAbses Cerebri 1astri sukma mNoch keine Bewertungen
- Management of Abcess CerebriDokument6 SeitenManagement of Abcess Cerebricamelia musaadNoch keine Bewertungen
- Neonatal Intensive Care EyeDokument2 SeitenNeonatal Intensive Care EyewahyuliastingmailcomNoch keine Bewertungen
- Acute Isolated Sphenoid Sinusitis in Children - 2021 - International Journal ofDokument8 SeitenAcute Isolated Sphenoid Sinusitis in Children - 2021 - International Journal ofHung Son TaNoch keine Bewertungen
- Paediatric Acute Encephalitis: Infection and InflammationDokument10 SeitenPaediatric Acute Encephalitis: Infection and InflammationRajeshKoriyaNoch keine Bewertungen
- Brain Tuberculomas, Tubercular Meningitis, and Post-Tubercular Hydrocephalus in ChildrenDokument5 SeitenBrain Tuberculomas, Tubercular Meningitis, and Post-Tubercular Hydrocephalus in ChildrenDave VentraNoch keine Bewertungen
- Brain Abscesses: An Overview in Children: Andrzej Krzyszto Fiak Paola Zangari Maia de Luca Alberto VillaniDokument4 SeitenBrain Abscesses: An Overview in Children: Andrzej Krzyszto Fiak Paola Zangari Maia de Luca Alberto VillaniSannita Mayusda BadiriNoch keine Bewertungen
- Bodil Sen 2018Dokument15 SeitenBodil Sen 2018Sannita Mayusda BadiriNoch keine Bewertungen
- Diagnostic Approach To Recurrent Bacterial Meningitis ChildrenDokument12 SeitenDiagnostic Approach To Recurrent Bacterial Meningitis ChildrenIRINANoch keine Bewertungen
- Mold Infections of the Central Nervous SystemDokument15 SeitenMold Infections of the Central Nervous SystemJohn TusselNoch keine Bewertungen
- Brain Abscess in Immunocompetent Adult PatientsDokument6 SeitenBrain Abscess in Immunocompetent Adult PatientsshofwaNoch keine Bewertungen
- Diagnosis and Treatment of CNS Infections in the Emergency DepartmentDokument26 SeitenDiagnosis and Treatment of CNS Infections in the Emergency DepartmentSirGonzNoch keine Bewertungen
- Do Brain Abscesses Have A Higher Incidence of Odontogenic Origin Than Previously ThoughtDokument4 SeitenDo Brain Abscesses Have A Higher Incidence of Odontogenic Origin Than Previously ThoughtHaytham JamilNoch keine Bewertungen
- Selulitis PDFDokument5 SeitenSelulitis PDFDhisa Zainita HabsariNoch keine Bewertungen
- Acutebacterialmeningitis: Current Review and Treatment UpdateDokument11 SeitenAcutebacterialmeningitis: Current Review and Treatment UpdateWidya Niendy PrameswariiNoch keine Bewertungen
- Meningitis Vs Ensefalitis MeganDokument10 SeitenMeningitis Vs Ensefalitis MeganFandi ArgiansyaNoch keine Bewertungen
- Cerebral MalariaDokument16 SeitenCerebral MalariaNLailyrahmaNoch keine Bewertungen
- Atlas of Clinical Cases on Brain Tumor ImagingVon EverandAtlas of Clinical Cases on Brain Tumor ImagingYelda ÖzsunarNoch keine Bewertungen
- Jurnal MH PDFDokument12 SeitenJurnal MH PDFcamelia musaadNoch keine Bewertungen
- Resources Used in This Design Url: Background - 3956685.htmDokument1 SeiteResources Used in This Design Url: Background - 3956685.htmcamelia musaadNoch keine Bewertungen
- Jurnal SistitisDokument5 SeitenJurnal Sistitiscamelia musaadNoch keine Bewertungen
- kjr-US For Benign and Maligna PDFDokument9 Seitenkjr-US For Benign and Maligna PDFLiaNoch keine Bewertungen
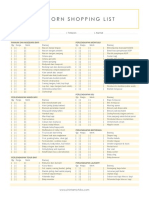
- Newborn Shopping List TemplateDokument1 SeiteNewborn Shopping List TemplateShellaCharismaAgryanandhaNoch keine Bewertungen
- Ebm Jurnal PDFDokument198 SeitenEbm Jurnal PDFcamelia musaadNoch keine Bewertungen
- Referat Asma AnakDokument26 SeitenReferat Asma Anakcamelia musaadNoch keine Bewertungen
- Jurnal Ebm KedkelDokument8 SeitenJurnal Ebm Kedkelcamelia musaadNoch keine Bewertungen
- Ebm JurnalDokument198 SeitenEbm Jurnalcamelia musaadNoch keine Bewertungen
- Surat Sponsor 1Dokument1 SeiteSurat Sponsor 1camelia musaadNoch keine Bewertungen
- Management of Abcess CerebriDokument6 SeitenManagement of Abcess Cerebricamelia musaadNoch keine Bewertungen
- Surat Pernyataaan NPWPDokument1 SeiteSurat Pernyataaan NPWPcamelia musaadNoch keine Bewertungen
- Epid, MK, ManagementDokument4 SeitenEpid, MK, Managementcamelia musaadNoch keine Bewertungen
- Brain Abscess: H. R W, M.DDokument1 SeiteBrain Abscess: H. R W, M.Dcamelia musaadNoch keine Bewertungen
- DentaPure Sell SheetDokument2 SeitenDentaPure Sell SheetJeff HowesNoch keine Bewertungen
- Jayden Alexander Tirta - Speech PreparationDokument5 SeitenJayden Alexander Tirta - Speech PreparationJAYDEN ALEXANDER TIRTANoch keine Bewertungen
- Philippine eHealth Program: Enabling Digital Transformation in HealthcareDokument33 SeitenPhilippine eHealth Program: Enabling Digital Transformation in HealthcareBads BrandaresNoch keine Bewertungen
- University of Cebu-BaniladDokument3 SeitenUniversity of Cebu-BaniladArgie DionioNoch keine Bewertungen
- Mental Health Issues Among University Students (Iman)Dokument4 SeitenMental Health Issues Among University Students (Iman)Asma IzlynNoch keine Bewertungen
- Journal Reading on Evaluation and Management of Infants Exposed to HIVDokument19 SeitenJournal Reading on Evaluation and Management of Infants Exposed to HIVIis Rica MustikaNoch keine Bewertungen
- Melissa Lockhart Resume 2021Dokument2 SeitenMelissa Lockhart Resume 2021api-581746859Noch keine Bewertungen
- MortuaryDokument6 SeitenMortuaryDr.Rajesh KamathNoch keine Bewertungen
- 326 Mental - Status - Examination Directions and RubricDokument4 Seiten326 Mental - Status - Examination Directions and Rubricmp1757Noch keine Bewertungen
- Lesson 3: Health Information System How Do Health Information Systems Look Like and What Architectures Are Appropriate?Dokument13 SeitenLesson 3: Health Information System How Do Health Information Systems Look Like and What Architectures Are Appropriate?ajengwedaNoch keine Bewertungen
- FPTP - Amoxicillin - Clavulanic Acid in Cats With & Without Chronic Kidney DiseaseDokument2 SeitenFPTP - Amoxicillin - Clavulanic Acid in Cats With & Without Chronic Kidney DiseaseMabe AguirreNoch keine Bewertungen
- Managing Hyperglycaemia in People With DKD - Final DraftDokument90 SeitenManaging Hyperglycaemia in People With DKD - Final DraftRiched LhyneNoch keine Bewertungen
- PEH 11 Q3 Mod1 Week 1 2 MELC01 Thelma R. SacsacDokument16 SeitenPEH 11 Q3 Mod1 Week 1 2 MELC01 Thelma R. Sacsaccalvin adralesNoch keine Bewertungen
- EU CBRN CoE Project 61 - Sound Management of ChemicalsDokument8 SeitenEU CBRN CoE Project 61 - Sound Management of ChemicalsTonyo LinaNoch keine Bewertungen
- Evaluation and Management of Splenic Injury in Blunt Abdominal TraumaDokument32 SeitenEvaluation and Management of Splenic Injury in Blunt Abdominal TraumaImam Hakim SuryonoNoch keine Bewertungen
- Safety Data Sheet: Armohib Ci-28Dokument21 SeitenSafety Data Sheet: Armohib Ci-28SJHEIK AbdullahNoch keine Bewertungen
- Tumor StagingDokument9 SeitenTumor Stagingmalaran.deboraheloisaNoch keine Bewertungen
- BHS INGGRIS Proper Hand WashingDokument11 SeitenBHS INGGRIS Proper Hand WashingAfifa RahmahNoch keine Bewertungen
- To Define Clinical Psychology, Here Is A Definition From American Psychological Association's Division 12Dokument14 SeitenTo Define Clinical Psychology, Here Is A Definition From American Psychological Association's Division 12Summer LoveNoch keine Bewertungen
- Psychological Psychoeducational Neuropsychological Assessment Information For Adults Families 1Dokument3 SeitenPsychological Psychoeducational Neuropsychological Assessment Information For Adults Families 1ClaudiaNoch keine Bewertungen
- Eneza Ujumbe: The Voices of Mathare YouthDokument4 SeitenEneza Ujumbe: The Voices of Mathare YouthakellewagumaNoch keine Bewertungen
- Dr. Sanjida Sultana's CVDokument4 SeitenDr. Sanjida Sultana's CVHasibul Hassan ShantoNoch keine Bewertungen
- Coping StrategyDokument2 SeitenCoping StrategyJeffson BalmoresNoch keine Bewertungen
- Mcdonalds Case Study Final ArtifactDokument10 SeitenMcdonalds Case Study Final Artifactapi-340015164Noch keine Bewertungen
- Soca PPT 2021Dokument44 SeitenSoca PPT 2021MSWD BAMBANGNoch keine Bewertungen
- Schonert-Reichl-Educating The Heart As Well As The MindDokument7 SeitenSchonert-Reichl-Educating The Heart As Well As The MindnewoldnoneNoch keine Bewertungen
- BBA Enrollment Form Front Page PDFDokument2 SeitenBBA Enrollment Form Front Page PDFYaj EstefanoNoch keine Bewertungen