Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- U Muc Doi Muci 3 Muci 4 Muci 5 Muci 6 Muci 7 Muci 8 Muci MuciDokument1 SeiteU Muc Doi Muci 3 Muci 4 Muci 5 Muci 6 Muci 7 Muci 8 Muci MuciDorin Cristian AntalNoch keine Bewertungen
- Clinically Isolated Syndrome (CIS)Dokument12 SeitenClinically Isolated Syndrome (CIS)Dorin Cristian AntalNoch keine Bewertungen
- The Oxford Handbook of Event-Related Potential Components: U Muc Doi Muci 3 Muci 4 Muci 5 Muci 6 Muci 7 Muci 8 Muci MuciDokument1 SeiteThe Oxford Handbook of Event-Related Potential Components: U Muc Doi Muci 3 Muci 4 Muci 5 Muci 6 Muci 7 Muci 8 Muci MuciDorin Cristian AntalNoch keine Bewertungen
- As A Man Thinketh by James AllenDokument22 SeitenAs A Man Thinketh by James AllenDorin Cristian AntalNoch keine Bewertungen
- International Registry of Steroid-Resistant Nephrotic Syndrome: Updated Epidemiological and Clinical DataDokument11 SeitenInternational Registry of Steroid-Resistant Nephrotic Syndrome: Updated Epidemiological and Clinical DataDorin Cristian AntalNoch keine Bewertungen
- 12 Boute 00 NatGenetDokument6 Seiten12 Boute 00 NatGenetDorin Cristian AntalNoch keine Bewertungen
- Childhood Nephrotic Syndrome: Steroid Sensitive, Steroid Resistant and BeyondDokument7 SeitenChildhood Nephrotic Syndrome: Steroid Sensitive, Steroid Resistant and BeyondDorin Cristian AntalNoch keine Bewertungen
- Management of Steroid Resistant Nephrotic Syndrome: GuidelinesDokument13 SeitenManagement of Steroid Resistant Nephrotic Syndrome: GuidelinesDorin Cristian AntalNoch keine Bewertungen
- The Therapeutic Response To Vincristine Was Examined in Seven ChildrenDokument3 SeitenThe Therapeutic Response To Vincristine Was Examined in Seven ChildrenDorin Cristian AntalNoch keine Bewertungen
- Pattern of Steroid-Resistant Nephrotic Syndrome in Children and The Role of Histopathology: A Single-Centre StudyDokument2 SeitenPattern of Steroid-Resistant Nephrotic Syndrome in Children and The Role of Histopathology: A Single-Centre StudyDorin Cristian AntalNoch keine Bewertungen
- Management of Steroid Resistant Nephrotic Syndrome: GuidelinesDokument13 SeitenManagement of Steroid Resistant Nephrotic Syndrome: GuidelinesDorin Cristian AntalNoch keine Bewertungen
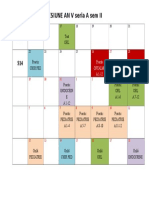
- Sesiune An V Seria A Sem Ii S13: Test ORLDokument1 SeiteSesiune An V Seria A Sem Ii S13: Test ORLDorin Cristian AntalNoch keine Bewertungen
- S2HY SlideHandoutsDokument511 SeitenS2HY SlideHandoutsDorin Cristian AntalNoch keine Bewertungen
- Orar Chirurgie Plastică, Vasculară, Cardiacă - Semestrul IiDokument1 SeiteOrar Chirurgie Plastică, Vasculară, Cardiacă - Semestrul IiDorin Cristian AntalNoch keine Bewertungen
- Icml06TLW ObjectType WolfeDokument4 SeitenIcml06TLW ObjectType WolfeDorin Cristian AntalNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- 2 Medicine MCQs NephrologyDokument3 Seiten2 Medicine MCQs NephrologyDiwakesh C BNoch keine Bewertungen
- Renal Cheat SheetDokument3 SeitenRenal Cheat Sheetkad ourNoch keine Bewertungen
- KDIGO GD Membranous NephropathyDokument1 SeiteKDIGO GD Membranous NephropathyF AudreyNoch keine Bewertungen
- SN Vs SNADokument26 SeitenSN Vs SNAChofi QolbiNoch keine Bewertungen
- Diseases of Glomerulus: Chronic Glomerulonephritis (CGN)Dokument7 SeitenDiseases of Glomerulus: Chronic Glomerulonephritis (CGN)mnr hmcNoch keine Bewertungen
- The Columbia Renal Biopsy Course: JULY 12 - JULY 14, 2023Dokument8 SeitenThe Columbia Renal Biopsy Course: JULY 12 - JULY 14, 2023Freddy Shanner Chávez VásquezNoch keine Bewertungen
- Rapidly Progressive Glomerulonephritis - P. Devarajan PDFDokument48 SeitenRapidly Progressive Glomerulonephritis - P. Devarajan PDFHerman HermanNoch keine Bewertungen
- Daftar PustakaDokument3 SeitenDaftar PustakaMiranda NNoch keine Bewertungen
- Pathology of Urinary SystemDokument384 SeitenPathology of Urinary SystemNzau MuangeNoch keine Bewertungen
- Nephrotic SyndromeDokument23 SeitenNephrotic SyndromeamlymarsNoch keine Bewertungen
- Glomerular Diseases My NotesDokument5 SeitenGlomerular Diseases My Notesmalar_km43Noch keine Bewertungen
- 6 - Woc CKD: Sklerosis SiskemikDokument1 Seite6 - Woc CKD: Sklerosis SiskemikWidyarti yerikaNoch keine Bewertungen
- Boala Polichistica Hepato-RenalaDokument1 SeiteBoala Polichistica Hepato-RenaladoinaNoch keine Bewertungen
- Manejo y Tratamiento de Enfermedades Glomerulares (Parte 2) : Conclusiones KDIGODokument25 SeitenManejo y Tratamiento de Enfermedades Glomerulares (Parte 2) : Conclusiones KDIGORodrigo Avellaneda CamposNoch keine Bewertungen
- E CalyptusDokument1 SeiteE CalyptusArdito GollerNoch keine Bewertungen
- Glomerular Diseases: DR Rashmi NazarethDokument49 SeitenGlomerular Diseases: DR Rashmi NazarethRohit RajeevanNoch keine Bewertungen
- Daftar Pustaka FixDokument2 SeitenDaftar Pustaka FixAlmira Shabrina SaraswatiNoch keine Bewertungen
- NephrologyDokument7 SeitenNephrologyYT ShortsNoch keine Bewertungen
- Block 4 Renal Lecture 1 MCQDokument5 SeitenBlock 4 Renal Lecture 1 MCQMahmoud ElshrkawyNoch keine Bewertungen
- SRS Kidney - 2016BDokument3 SeitenSRS Kidney - 2016ByayayanizaNoch keine Bewertungen
- Kidney QuizDokument3 SeitenKidney QuizBindashboy0100% (1)
- MCQ2Dokument5 SeitenMCQ2Amir Ibnu HizbullahNoch keine Bewertungen
- Nephrotic SyndromeDokument6 SeitenNephrotic SyndromeSanthosh KumarNoch keine Bewertungen
- Rangkuman Terminologi MedisDokument6 SeitenRangkuman Terminologi MedisAlissa RevoliusNoch keine Bewertungen
- Renal Pathology-Mreh 32104: Disorders of KidneyDokument3 SeitenRenal Pathology-Mreh 32104: Disorders of KidneyArvinth Guna SegaranNoch keine Bewertungen
- Nephrotic Syndrome PresentationDokument39 SeitenNephrotic Syndrome PresentationEzekiel moraraNoch keine Bewertungen
- Hematuria: Preseptor: Dr. Sawkar Vijay Pramod, Sp.UDokument39 SeitenHematuria: Preseptor: Dr. Sawkar Vijay Pramod, Sp.UFIKRI MUHAMMADNoch keine Bewertungen
- What Is Glomerulonephritis?Dokument7 SeitenWhat Is Glomerulonephritis?SSNoch keine Bewertungen
- MCQDokument40 SeitenMCQLuthie Singh100% (2)
- Nephrotic Syndrome - Armando HasudunganDokument18 SeitenNephrotic Syndrome - Armando HasudunganzahraaNoch keine Bewertungen