Das könnte Ihnen auch gefallen
- 10 Essential Books For Active TradersDokument6 Seiten10 Essential Books For Active TradersChrisTheodorou100% (2)
- LicencesDokument5 SeitenLicencesstopnaggingmeNoch keine Bewertungen
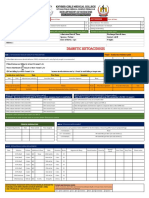
- BIMC Adult DKA Protocol 2012Dokument5 SeitenBIMC Adult DKA Protocol 2012djizhieeNoch keine Bewertungen
- Idiot NotesDokument53 SeitenIdiot NotesRay PerezNoch keine Bewertungen
- Overdose and PoisoningDokument4 SeitenOverdose and PoisoningMahmoud SelimNoch keine Bewertungen
- Blood Glucose-Insulin Administration-Study GuideDokument8 SeitenBlood Glucose-Insulin Administration-Study GuideChandra MuraliNoch keine Bewertungen
- 7 Liver - Spleen TraumaDokument34 Seiten7 Liver - Spleen Traumabagus75% (4)
- Kegawatdaruratan Diabetes Melitus: Terapi Insulin IntravenaDokument27 SeitenKegawatdaruratan Diabetes Melitus: Terapi Insulin IntravenaSesilia Sri Yanti GaddyNoch keine Bewertungen
- 24hr Fluid Balance ADULT Chart - v3Dokument2 Seiten24hr Fluid Balance ADULT Chart - v3anggita diah100% (1)
- Broiler ProductionDokument13 SeitenBroiler ProductionAlexa Khrystal Eve Gorgod100% (1)
- Mark Magazine#65Dokument196 SeitenMark Magazine#65AndrewKanischevNoch keine Bewertungen
- Christena Nippert-Eng - Watching Closely - A Guide To Ethnographic Observation-Oxford University Press (2015)Dokument293 SeitenChristena Nippert-Eng - Watching Closely - A Guide To Ethnographic Observation-Oxford University Press (2015)Emiliano CalabazaNoch keine Bewertungen
- Corvina PRIMEDokument28 SeitenCorvina PRIMEMillerIndigoNoch keine Bewertungen
- ULH Main DKA Pathway v3 July 2018Dokument8 SeitenULH Main DKA Pathway v3 July 2018omarragabselimNoch keine Bewertungen
- New Insulin PolicyDokument8 SeitenNew Insulin Policybelle dyNoch keine Bewertungen
- Intravenous Insulin Prescription and Fluid Protocol: For Diabetic Keto-Acidosis (Dka)Dokument4 SeitenIntravenous Insulin Prescription and Fluid Protocol: For Diabetic Keto-Acidosis (Dka)sunrise755Noch keine Bewertungen
- Guidelines For The Management of Patients With Hyperglycaemia or Diabetes and Suspected Acute Coronary SyndromesDokument4 SeitenGuidelines For The Management of Patients With Hyperglycaemia or Diabetes and Suspected Acute Coronary SyndromesRebecca ChenNoch keine Bewertungen
- Intensive Insulin TherapyDokument54 SeitenIntensive Insulin TherapySiva RamanNoch keine Bewertungen
- InsulinDextroseInfusion2020 0Dokument5 SeitenInsulinDextroseInfusion2020 0ambulatNoch keine Bewertungen
- 1 RBH Icu Insulin Guidelines May 2009Dokument6 Seiten1 RBH Icu Insulin Guidelines May 2009bastarduniverseNoch keine Bewertungen
- Management of Anesthesia: Diabetes MellitusDokument29 SeitenManagement of Anesthesia: Diabetes MellitusHari PrasadNoch keine Bewertungen
- ED Module 4Dokument26 SeitenED Module 4Washi AkunNoch keine Bewertungen
- Basal Insulin Versus Premixed Insulin For The Treatment of T2DmDokument98 SeitenBasal Insulin Versus Premixed Insulin For The Treatment of T2DmMaya SwariNoch keine Bewertungen
- IV Insulin Infusion ProtocolDokument4 SeitenIV Insulin Infusion ProtocolWeeranan Sueb-LaNoch keine Bewertungen
- 003 DkaDokument9 Seiten003 DkaMohammedNoch keine Bewertungen
- Vriii PresentationDokument29 SeitenVriii Presentationsundance127Noch keine Bewertungen
- Endocrine System: Capillary Glucose MonitoringDokument34 SeitenEndocrine System: Capillary Glucose Monitoringjoel david knda mj100% (1)
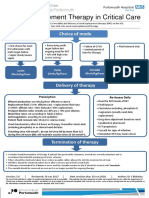
- Renal Replacement Therapy in Critical Care: Choice of ModeDokument15 SeitenRenal Replacement Therapy in Critical Care: Choice of ModePeter AgabaNoch keine Bewertungen
- Inpatient Guideline JoslinDokument8 SeitenInpatient Guideline Joslinospinu6780Noch keine Bewertungen
- Insulin Section O FINALDokument26 SeitenInsulin Section O FINALMc FoeyNoch keine Bewertungen
- Sliding Scale REGULAR HUMULIN INSULIN - Physician Order SetDokument1 SeiteSliding Scale REGULAR HUMULIN INSULIN - Physician Order SetDimas RendhykaNoch keine Bewertungen
- Protocol For Intensive Intravenous Insulin Infusion For ICUDokument2 SeitenProtocol For Intensive Intravenous Insulin Infusion For ICUburlacuraduuNoch keine Bewertungen
- Adjunting Insuline DosisDokument5 SeitenAdjunting Insuline DosisPaco TrooperNoch keine Bewertungen
- Hyperglycemia Algorithm 2Dokument1 SeiteHyperglycemia Algorithm 2damondouglasNoch keine Bewertungen
- Guidelines in The Treatment of Hyper Osmolar Non Ketotic Coma (Honk)Dokument4 SeitenGuidelines in The Treatment of Hyper Osmolar Non Ketotic Coma (Honk)picassowaffleNoch keine Bewertungen
- Insulin Drip YALEDokument4 SeitenInsulin Drip YALEnikeNoch keine Bewertungen
- Blood Glucose MonitoringDokument19 SeitenBlood Glucose Monitoringkessiabon459Noch keine Bewertungen
- PedomanDokument2 SeitenPedomanandi namirahNoch keine Bewertungen
- Fit-Diploma 3-2-2024Dokument57 SeitenFit-Diploma 3-2-2024light tweenNoch keine Bewertungen
- DiabetesDokument7 SeitenDiabetesapi-142637023Noch keine Bewertungen
- Renal Replacement Therapy in Critical Care: Choice of ModeDokument15 SeitenRenal Replacement Therapy in Critical Care: Choice of ModeJelena Obrenovic StankovicNoch keine Bewertungen
- Glycemic ManagementDokument39 SeitenGlycemic ManagementZayar HmunNoch keine Bewertungen
- Critical Care Adult Insulin InfusionDokument2 SeitenCritical Care Adult Insulin InfusionTunas AndriantoNoch keine Bewertungen
- Pharmacokinetics Common Insulin Preps - UpToDateDokument1 SeitePharmacokinetics Common Insulin Preps - UpToDateTyler KingNoch keine Bewertungen
- Diabetic Ketoacidosis (D.K.A) Beaumont Hospital Protocol: DiagnosisDokument1 SeiteDiabetic Ketoacidosis (D.K.A) Beaumont Hospital Protocol: Diagnosislouglee9174100% (1)
- Samba Consensus For Diabetes During Ambulatory SurgeryDokument5 SeitenSamba Consensus For Diabetes During Ambulatory Surgeryabirray65Noch keine Bewertungen
- InsulinDokument4 SeitenInsulinHa Zizzle100% (1)
- Pharmacology 2: Diabetes Assignment 1Dokument17 SeitenPharmacology 2: Diabetes Assignment 1Daniel PerlasNoch keine Bewertungen
- DM Before and After OperateDokument5 SeitenDM Before and After OperateNararto PrijogoNoch keine Bewertungen
- 1 SlidingScalePCHSDokument1 Seite1 SlidingScalePCHSHaziq MarsNoch keine Bewertungen
- Gent and Vanc Calculator 290709Dokument19 SeitenGent and Vanc Calculator 290709Alisdair MacDonaldNoch keine Bewertungen
- DKA Adults Management Protocol - DR Anwar Ul HaqDokument3 SeitenDKA Adults Management Protocol - DR Anwar Ul HaqAnwar ul HaqNoch keine Bewertungen
- CH 39 Anaesthesia and Diabetes MellitusDokument6 SeitenCH 39 Anaesthesia and Diabetes MellitusChristian LeepoNoch keine Bewertungen
- CTU Insulin Sliding ScalesDokument2 SeitenCTU Insulin Sliding ScalesnindylistyNoch keine Bewertungen
- Diabetic Ketoacidosis Acute Management: A State of Absolute Insulin BankruptcyDokument24 SeitenDiabetic Ketoacidosis Acute Management: A State of Absolute Insulin BankruptcyGwEn LimNoch keine Bewertungen
- Patient Units Severe Sepsis Screening ToolDokument2 SeitenPatient Units Severe Sepsis Screening ToolArnelli HutagalungNoch keine Bewertungen
- Management of Diabetic Cats With Long Acting InsulinDokument16 SeitenManagement of Diabetic Cats With Long Acting Insulindia_dianneNoch keine Bewertungen
- Diabetic Care in Acute Febrile IllnessDokument27 SeitenDiabetic Care in Acute Febrile IllnessDr-Ajay TripathiNoch keine Bewertungen
- Item 6f - Acute Management of Hyperosmolar Hyperglycaemic StateDokument1 SeiteItem 6f - Acute Management of Hyperosmolar Hyperglycaemic StateStef AnNoch keine Bewertungen
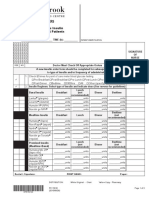
- Sunnybrook Insulin OrdersDokument5 SeitenSunnybrook Insulin OrderskaybeeNoch keine Bewertungen
- STD Heparin Protocol MethodistDokument1 SeiteSTD Heparin Protocol Methodistd40sithuiNoch keine Bewertungen
- HIP MalesDokument3 SeitenHIP MalesMaddy HuckelNoch keine Bewertungen
- Sick Day Plan For Type 2 Diabetes - TemplateDokument4 SeitenSick Day Plan For Type 2 Diabetes - Templatehernandez2812Noch keine Bewertungen
- PCC HandbookDokument193 SeitenPCC HandbookMusa LandeNoch keine Bewertungen
- Simpo 3 - DR Hemi SPPD KEMD - Can We Use Sliding Scale On Critical and Emergency HyperglicemiaDokument19 SeitenSimpo 3 - DR Hemi SPPD KEMD - Can We Use Sliding Scale On Critical and Emergency HyperglicemiaAgnes Irene ZagotoNoch keine Bewertungen
- Review of Efficacy and Safety of Insulin Agents 3Dokument14 SeitenReview of Efficacy and Safety of Insulin Agents 3sendhilkumarNoch keine Bewertungen
- Paket Rasa Sayang RestaurantDokument10 SeitenPaket Rasa Sayang Restaurantnostra83Noch keine Bewertungen
- TG 13 PDFDokument109 SeitenTG 13 PDFnostra83Noch keine Bewertungen
- Use of Restraint Form - Education Points For CompletionDokument2 SeitenUse of Restraint Form - Education Points For Completionnostra83Noch keine Bewertungen
- 13EmergencyRooms FountainDokument82 Seiten13EmergencyRooms Fountainnostra83Noch keine Bewertungen
- Adedayo Ashana, MS1 .: Univ. of Pennsylvania, School of MedicineDokument12 SeitenAdedayo Ashana, MS1 .: Univ. of Pennsylvania, School of Medicinenostra83Noch keine Bewertungen
- Current MNGMNT Splenic InjDokument52 SeitenCurrent MNGMNT Splenic Injnostra83Noch keine Bewertungen
- Disorders of Neural Tube ClosureDokument46 SeitenDisorders of Neural Tube Closurenostra83Noch keine Bewertungen
- Bigbazaar PDFDokument14 SeitenBigbazaar PDFazhagu sundaramNoch keine Bewertungen
- Course Projects PDFDokument1 SeiteCourse Projects PDFsanjog kshetriNoch keine Bewertungen
- Minuets of The Second SCTVE MeetingDokument11 SeitenMinuets of The Second SCTVE MeetingLokuliyanaNNoch keine Bewertungen
- Cad Data Exchange StandardsDokument16 SeitenCad Data Exchange StandardskannanvikneshNoch keine Bewertungen
- Antibiotics MCQsDokument4 SeitenAntibiotics MCQsPh Israa KadhimNoch keine Bewertungen
- Kefauver Harris AmendmentsDokument7 SeitenKefauver Harris AmendmentsAnil kumarNoch keine Bewertungen
- BioremediationDokument21 SeitenBioremediationagung24864Noch keine Bewertungen
- AFAR - 07 - New Version No AnswerDokument7 SeitenAFAR - 07 - New Version No AnswerjonasNoch keine Bewertungen
- Health and Safety For The Meat Industry: Guidance NotesDokument198 SeitenHealth and Safety For The Meat Industry: Guidance NotesPredrag AndjelkovicNoch keine Bewertungen
- Intervensi Terapi Pada Sepsis PDFDokument28 SeitenIntervensi Terapi Pada Sepsis PDFifan zulfantriNoch keine Bewertungen
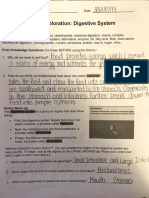
- Student Exploration: Digestive System: Food Inio Simple Nutrien/oDokument9 SeitenStudent Exploration: Digestive System: Food Inio Simple Nutrien/oAshantiNoch keine Bewertungen
- QuinnmcfeetersresumeDokument1 SeiteQuinnmcfeetersresumeapi-510833585Noch keine Bewertungen
- LS01 ServiceDokument53 SeitenLS01 ServicehutandreiNoch keine Bewertungen
- Unit 4Dokument15 SeitenUnit 4David Lopez LaraNoch keine Bewertungen
- Planning EngineerDokument1 SeitePlanning EngineerChijioke ObiNoch keine Bewertungen
- Technion - Computer Science Department - Technical Report CS0055 - 1975Dokument25 SeitenTechnion - Computer Science Department - Technical Report CS0055 - 1975MoltKeeNoch keine Bewertungen
- Revit 2023 Architecture FudamentalDokument52 SeitenRevit 2023 Architecture FudamentalTrung Kiên TrầnNoch keine Bewertungen
- Using The Monopoly Board GameDokument6 SeitenUsing The Monopoly Board Gamefrieda20093835Noch keine Bewertungen
- Distribution BoardDokument7 SeitenDistribution BoardmuralichandrasekarNoch keine Bewertungen
- Countable 3Dokument2 SeitenCountable 3Pio Sulca Tapahuasco100% (1)
- Ideal Gas Law Lesson Plan FinalDokument5 SeitenIdeal Gas Law Lesson Plan FinalLonel SisonNoch keine Bewertungen
- BECIL Registration Portal: How To ApplyDokument2 SeitenBECIL Registration Portal: How To ApplySoul BeatsNoch keine Bewertungen
- List of The Legend of Korra Episodes - Wikipedia PDFDokument27 SeitenList of The Legend of Korra Episodes - Wikipedia PDFEmmanuel NocheNoch keine Bewertungen
- Blake 2013Dokument337 SeitenBlake 2013Tushar AmetaNoch keine Bewertungen