Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- 7 Protocol For CCT RT-PCRDokument3 Seiten7 Protocol For CCT RT-PCRsukapilNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- English Plain and Simple by Jose ADokument2 SeitenEnglish Plain and Simple by Jose AsukapilNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- BiophysicsDokument6 SeitenBiophysicssukapilNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- New Microsoft Office Power Point PresentationDokument22 SeitenNew Microsoft Office Power Point PresentationsukapilNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Blood GroupingDokument2 SeitenBlood GroupingsukapilNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- MDLQSARreprintDokument2 SeitenMDLQSARreprintsukapilNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Nsejs Practice Test FiitjeeDokument9 SeitenNsejs Practice Test FiitjeeVandana Saini0% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hepatitis B Virus PDFDokument474 SeitenHepatitis B Virus PDFJoaquin Hernandez Gomez100% (1)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- IIsc Biological SciencesDokument17 SeitenIIsc Biological SciencesdhurvasNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- Castro Et Al. 2017. RNA Isolation Microalgae IquitosDokument7 SeitenCastro Et Al. 2017. RNA Isolation Microalgae IquitosLeonardo Mendoza CarbajalNoch keine Bewertungen
- Primescript™ Reverse Transcriptase: Code No. 2680Q Size: 2,000 Units Shipping at 20 Store at 20Dokument2 SeitenPrimescript™ Reverse Transcriptase: Code No. 2680Q Size: 2,000 Units Shipping at 20 Store at 20Isaac Nicholas NotorioNoch keine Bewertungen
- HIV Transmission, Pathophysiology, Clinical Manifestations and TreatmentDokument4 SeitenHIV Transmission, Pathophysiology, Clinical Manifestations and TreatmentBatch V Med 2 SY 21-22Noch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Reverse TranscriptionDokument14 SeitenReverse TranscriptionKannan Kannan N SNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Real-Time qPCR Methods for miRNA Expression ProfilingDokument6 SeitenReal-Time qPCR Methods for miRNA Expression ProfilingJyotsna MishraNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Applied Biosystems Absolute Quantitation ManualDokument110 SeitenApplied Biosystems Absolute Quantitation ManualLimin MaNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
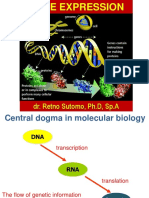
- Dr. Retno Sutomo, PH.D, Sp.ADokument37 SeitenDr. Retno Sutomo, PH.D, Sp.ADoni RevaiNoch keine Bewertungen
- Chapter 12: DNA Technology and The Human Genome: Biology: Concepts and Connections, 5e (Campbell)Dokument10 SeitenChapter 12: DNA Technology and The Human Genome: Biology: Concepts and Connections, 5e (Campbell)abeer khawwamNoch keine Bewertungen
- Cdna Synthesis Made For Momentum: Superscript Iv Reverse TranscriptasesDokument4 SeitenCdna Synthesis Made For Momentum: Superscript Iv Reverse TranscriptasesPombas ConcurseirosNoch keine Bewertungen
- Are Viruses Living or Non-Living Organisms?Dokument8 SeitenAre Viruses Living or Non-Living Organisms?Sydney Cloyce NagalNoch keine Bewertungen
- Polymerase Chain ReactionDokument16 SeitenPolymerase Chain ReactionAbdulati Abu RewillaNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Introduction To HIV and Its LifecycleDokument41 SeitenIntroduction To HIV and Its LifecycleJohnson BrownNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- IAL Biology SB2 Answers 8CDokument5 SeitenIAL Biology SB2 Answers 8CsalmaNoch keine Bewertungen
- Krok1 2017 Explanation Ewlm PDFDokument96 SeitenKrok1 2017 Explanation Ewlm PDFHimanshu Rana0% (1)
- Horowitz Aids and EbolaDokument11 SeitenHorowitz Aids and EboladeliriousheterotopiasNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Inverse PCR amplifies unknown DNA flanking known sequencesDokument8 SeitenInverse PCR amplifies unknown DNA flanking known sequencesNiraj Agarwal100% (1)
- Viral Classification: DNA VirusesDokument10 SeitenViral Classification: DNA Virusess.khan9211rediffmail.comNoch keine Bewertungen
- COVID-19 - A Special Report On The 2020 Novel Coronavirus Pandemic - SOTN - Alternative News, Analysis & CommentaryDokument71 SeitenCOVID-19 - A Special Report On The 2020 Novel Coronavirus Pandemic - SOTN - Alternative News, Analysis & CommentaryRuss TaylorNoch keine Bewertungen
- Study Guide For CHP 15Dokument4 SeitenStudy Guide For CHP 15Fati UmaruNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- AIDS Western Blot #275Dokument18 SeitenAIDS Western Blot #275Pedro_J_Colon__5052Noch keine Bewertungen
- TransposonsDokument6 SeitenTransposonsnikhilsathwikNoch keine Bewertungen
- Cloning Tech GuideDokument40 SeitenCloning Tech GuideioncacaciosuNoch keine Bewertungen
- New England Biolabs Certificate of Analysis: 240 County Road Ipswich, MA 01938-2723 Tel 978-927-5054 Fax 978-921-1350Dokument2 SeitenNew England Biolabs Certificate of Analysis: 240 County Road Ipswich, MA 01938-2723 Tel 978-927-5054 Fax 978-921-1350HoweleNoch keine Bewertungen
- Goscript Reverse Transcriptase ProtocolDokument2 SeitenGoscript Reverse Transcriptase Protocolinvestbiz optionstarNoch keine Bewertungen
- BB101 Answer Key Mid-SemDokument4 SeitenBB101 Answer Key Mid-SemBhushanNoch keine Bewertungen
- TOEFL Test 2Dokument23 SeitenTOEFL Test 2Rio HandokoNoch keine Bewertungen
- Nsejs Exam Solutions Paper 2019 PDFDokument27 SeitenNsejs Exam Solutions Paper 2019 PDFMrinalini SinghNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)