Das könnte Ihnen auch gefallen
- Amanda K Scott 3535 W Cambridge AVE Fresno, CA 93722-6561Dokument6 SeitenAmanda K Scott 3535 W Cambridge AVE Fresno, CA 93722-6561Amanda Scott100% (1)
- Kenndal D Crawford 109 Inwood Court Spartanburg, SC 29302: Employer Use Only Corp. DeptDokument2 SeitenKenndal D Crawford 109 Inwood Court Spartanburg, SC 29302: Employer Use Only Corp. Depttaylorizabella1Noch keine Bewertungen
- DOL RDWSU 2020 Form 5500Dokument205 SeitenDOL RDWSU 2020 Form 5500seanredmondNoch keine Bewertungen
- FIRE 2011 Form 990Dokument36 SeitenFIRE 2011 Form 990FIRENoch keine Bewertungen
- File Your NJ Tax Return Online or by E-FileDokument68 SeitenFile Your NJ Tax Return Online or by E-FileStephen HallickNoch keine Bewertungen
- 81601CP575Notice 1692149599160Dokument3 Seiten81601CP575Notice 1692149599160FGHJJ FDJFHDNoch keine Bewertungen
- Windward Fund's 2018 Tax FormsDokument49 SeitenWindward Fund's 2018 Tax FormsJoe SchoffstallNoch keine Bewertungen
- Formsoppsapplication Illinois Birth Record 2018Dokument2 SeitenFormsoppsapplication Illinois Birth Record 2018CynthiaNoch keine Bewertungen
- Compass Application 2.14Dokument11 SeitenCompass Application 2.14Matthew SweeneyNoch keine Bewertungen
- 2019 California Tax Return RefundDokument18 Seiten2019 California Tax Return RefundPolo PoloNoch keine Bewertungen
- 2013 AgriSafe 990Dokument28 Seiten2013 AgriSafe 990AgriSafeNoch keine Bewertungen
- Oddo Brothers Cpas: William & Regina LittleDokument30 SeitenOddo Brothers Cpas: William & Regina Littlebill littleNoch keine Bewertungen
- Annu Acc StatementDokument1 SeiteAnnu Acc StatementAHMAD ANTOINE DELAINENoch keine Bewertungen
- Employer's QUARTERLY Federal Tax Return: 5 3 1 3 1 0 0 1 0 Kenifer Corp Computer SolutionsDokument4 SeitenEmployer's QUARTERLY Federal Tax Return: 5 3 1 3 1 0 0 1 0 Kenifer Corp Computer SolutionsrobbickelNoch keine Bewertungen
- 2021 - TaxReturn 2pagessignedDokument3 Seiten2021 - TaxReturn 2pagessignedDedrick RiversNoch keine Bewertungen
- PUA 1099G tax form summaryDokument1 SeitePUA 1099G tax form summaryClifton WilsonNoch keine Bewertungen
- MyfileDokument1 SeiteMyfileanon-302065Noch keine Bewertungen
- Monetary Determination Pandemic Unemployment Assistance: Michael L PresleyDokument3 SeitenMonetary Determination Pandemic Unemployment Assistance: Michael L PresleyDylan VanslochterenNoch keine Bewertungen
- Cash FlowDokument1 SeiteCash Flowpawan_019Noch keine Bewertungen
- Imigracion 2Dokument15 SeitenImigracion 2erickNoch keine Bewertungen
- Pepco Payment Receipt 10/1/2019Dokument1 SeitePepco Payment Receipt 10/1/2019Ace MereriaNoch keine Bewertungen
- Paula Atkins 17881 Thelma Ave Apt A Jupiter, FL 33458 Claimant ID: 226330Dokument2 SeitenPaula Atkins 17881 Thelma Ave Apt A Jupiter, FL 33458 Claimant ID: 226330Natural Beauty LaserNoch keine Bewertungen
- Payroll Register PD01-31-13 PDFDokument26 SeitenPayroll Register PD01-31-13 PDFJoseph ManriquezNoch keine Bewertungen
- Advanced Scenario 6: Samantha Rollins (2017)Dokument9 SeitenAdvanced Scenario 6: Samantha Rollins (2017)Center for Economic Progress0% (1)
- IRS Form W-2 Tax DocumentDokument1 SeiteIRS Form W-2 Tax DocumentMickeyNoch keine Bewertungen
- Emergency Replacement Parts for Grove RT 760E CraneDokument1 SeiteEmergency Replacement Parts for Grove RT 760E CraneraulNoch keine Bewertungen
- Profit or Loss From Business: Linda Gercken 156-56-8670Dokument2 SeitenProfit or Loss From Business: Linda Gercken 156-56-8670ROB100% (1)
- Aaron Berg w2Dokument2 SeitenAaron Berg w2kevin kuhnNoch keine Bewertungen
- Adrian LLCDokument3 SeitenAdrian LLCfunny videosNoch keine Bewertungen
- Direct Deposit Enrollment Form: Account Information AmountDokument1 SeiteDirect Deposit Enrollment Form: Account Information AmountClifton WilsonNoch keine Bewertungen
- Signature Card InfoDokument1 SeiteSignature Card Infosadik lawanNoch keine Bewertungen
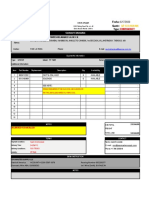
- 1013 ALC Quotation ALCSN201029001 20201111080153Dokument2 Seiten1013 ALC Quotation ALCSN201029001 20201111080153TRABAJANDIÑO PEREZNoch keine Bewertungen
- Confirmation Number and Date for Illinois Business RegistrationDokument7 SeitenConfirmation Number and Date for Illinois Business RegistrationMohammed HussainNoch keine Bewertungen
- Is in Kind 03-16-09Dokument1 SeiteIs in Kind 03-16-09Azi PaybarahNoch keine Bewertungen
- Captura de Pantalla 2022-02-05 A La(s) 4.03.49 A.M.Dokument4 SeitenCaptura de Pantalla 2022-02-05 A La(s) 4.03.49 A.M.Adriana AnsurezNoch keine Bewertungen
- FDA II LLC Lease AgreementDokument40 SeitenFDA II LLC Lease AgreementJulian CuellarNoch keine Bewertungen
- ICF FORMDokument4 SeitenICF FORMFrank ValenzuelaNoch keine Bewertungen
- Garner, D 4:21 PDFDokument1 SeiteGarner, D 4:21 PDFAaliyahNoch keine Bewertungen
- Two Wheeler Insurance Policy DetailsDokument4 SeitenTwo Wheeler Insurance Policy DetailsShashanth Kumar (CS - OMTP)Noch keine Bewertungen
- 2022 Uber 1099-NECDokument2 Seiten2022 Uber 1099-NECmwgageNoch keine Bewertungen
- 1098T17Dokument2 Seiten1098T17RegrubdiupsNoch keine Bewertungen
- 1099-G unemployment benefitsDokument1 Seite1099-G unemployment benefitsKristine McVeighNoch keine Bewertungen
- 2019 Chandler D Form 1040 Individual Tax Return - Records-ALDokument7 Seiten2019 Chandler D Form 1040 Individual Tax Return - Records-ALwhat is thisNoch keine Bewertungen
- UntitledDokument10 SeitenUntitledJosh SofferNoch keine Bewertungen
- 71 Gooo 007040320000 R 631 B4 BB0 AF3621Dokument1 Seite71 Gooo 007040320000 R 631 B4 BB0 AF3621JaCoby HutchinsonNoch keine Bewertungen
- CertainGovernmentPaymentsPUA 1099G CharrisePhelps 654202101193245Dokument1 SeiteCertainGovernmentPaymentsPUA 1099G CharrisePhelps 654202101193245c phelpsNoch keine Bewertungen
- Base Builder - New Hire PaperworkDokument10 SeitenBase Builder - New Hire Paperworkelhard shalloNoch keine Bewertungen
- 2014 Alabama Possible 990Dokument39 Seiten2014 Alabama Possible 990Alabama PossibleNoch keine Bewertungen
- FD 941 Apr-Jun 2017 PDFDokument3 SeitenFD 941 Apr-Jun 2017 PDFScott WinklerNoch keine Bewertungen
- Vba 21 674 AreDokument3 SeitenVba 21 674 AreCynthia StovallNoch keine Bewertungen
- AZ Argan Ventures LTDDokument20 SeitenAZ Argan Ventures LTDBarangaySanLuisNoch keine Bewertungen
- Exemption Certificate - SalesDokument2 SeitenExemption Certificate - SalesExecutive F&ADADUNoch keine Bewertungen
- Schedule of Liabilities (SBA Form 2202)Dokument1 SeiteSchedule of Liabilities (SBA Form 2202)Vaé Ribera100% (1)
- Benefit Verification LetterDokument2 SeitenBenefit Verification Letteroh lampNoch keine Bewertungen
- 1 5136803172601299942 PDFDokument3 Seiten1 5136803172601299942 PDFnurulamin00023Noch keine Bewertungen
- Printing H - FORMFLOW - SF3107.FRPDokument10 SeitenPrinting H - FORMFLOW - SF3107.FRPKeller Brown JnrNoch keine Bewertungen
- Jaleica Coding and Billing LLC.: 437 Melissa Circle Romeoville IL.60446Dokument8 SeitenJaleica Coding and Billing LLC.: 437 Melissa Circle Romeoville IL.60446Julius MasiganNoch keine Bewertungen
- Employee Paystub EditedDokument1 SeiteEmployee Paystub EditedSandra ChrisNoch keine Bewertungen
- Computerised Payroll Practice Set Using MYOB AccountRight: Australian EditionVon EverandComputerised Payroll Practice Set Using MYOB AccountRight: Australian EditionNoch keine Bewertungen
- Methods to Overcome the Financial and Money Transfer Blockade against Palestine and any Country Suffering from Financial BlockadeVon EverandMethods to Overcome the Financial and Money Transfer Blockade against Palestine and any Country Suffering from Financial BlockadeNoch keine Bewertungen
- Etl Ab Initio PDFDokument2 SeitenEtl Ab Initio PDFDustin0% (1)
- Abelton EMP Course Workbook Updated August 2017 PDFDokument147 SeitenAbelton EMP Course Workbook Updated August 2017 PDFMongezi MceluNoch keine Bewertungen
- NFL 101 Breaking Down The Basics of 2-Man CoverageDokument10 SeitenNFL 101 Breaking Down The Basics of 2-Man Coveragecoachmark285Noch keine Bewertungen
- Flexi Wcdma BtsDokument25 SeitenFlexi Wcdma BtsSyed Ashfaq HussainNoch keine Bewertungen
- Hydrostatic Test ReportsDokument3 SeitenHydrostatic Test ReportsHanuman RaoNoch keine Bewertungen
- Stare DecisisDokument7 SeitenStare DecisisBirolal Jamatia100% (1)
- Material Safety Data Sheet "Cut Back Bitumen": Section 1: Product and Company IdentificationDokument4 SeitenMaterial Safety Data Sheet "Cut Back Bitumen": Section 1: Product and Company IdentificationPecel LeleNoch keine Bewertungen
- LeadershipDokument5 SeitenLeadershipapi-3850643Noch keine Bewertungen
- Resume of Thomas Qiao SAP FICO (5yrs Version 4.7) : ProfileDokument3 SeitenResume of Thomas Qiao SAP FICO (5yrs Version 4.7) : ProfileVenkata AraveetiNoch keine Bewertungen
- OBURE Understanding How Reits Market WorksDokument3 SeitenOBURE Understanding How Reits Market WorksJohn evansNoch keine Bewertungen
- 06 Traffic Flow Fundamentals PDFDokument27 Seiten06 Traffic Flow Fundamentals PDFDaryl ChanNoch keine Bewertungen
- Eskom Tariff Book - 2018-19Dokument54 SeitenEskom Tariff Book - 2018-19Sandro MasakiNoch keine Bewertungen
- Alternative Investments TestDokument18 SeitenAlternative Investments TestkoosNoch keine Bewertungen
- An Internship Report on Customer Service of Prabhu BankDokument48 SeitenAn Internship Report on Customer Service of Prabhu BankKaran PandeyNoch keine Bewertungen
- Facebook Declaration 1Dokument69 SeitenFacebook Declaration 1wanderlust823Noch keine Bewertungen
- Oracle Database Performance: Vmware Cloud On AwsDokument14 SeitenOracle Database Performance: Vmware Cloud On Awscatelor419Noch keine Bewertungen
- Course 1 Introduction To SIMS: Student Information Management System (SIMS) Office of The RegistrarDokument28 SeitenCourse 1 Introduction To SIMS: Student Information Management System (SIMS) Office of The RegistrarWeijia WangNoch keine Bewertungen
- GETT Breen Records - RedactedDokument1.141 SeitenGETT Breen Records - RedactedRobert LeeNoch keine Bewertungen
- Comparator: Differential VoltageDokument8 SeitenComparator: Differential VoltageTanvir Ahmed MunnaNoch keine Bewertungen
- Gamalama Desain - Jurnal Khusus - Hanifah Hilyah SyahDokument3 SeitenGamalama Desain - Jurnal Khusus - Hanifah Hilyah Syahreza hariansyahNoch keine Bewertungen
- INTERNSHIP DIARY - SESSION 2019-2020Dokument28 SeitenINTERNSHIP DIARY - SESSION 2019-2020Nilotpal RaiNoch keine Bewertungen
- Political Science Class 12TH Project Work 2022-23Dokument2 SeitenPolitical Science Class 12TH Project Work 2022-23Hariom Yadav100% (1)
- Data Exfiltration Using Linux BinariesDokument22 SeitenData Exfiltration Using Linux Binarieseve johnsonNoch keine Bewertungen
- Module Combustion Engineering-1-2Dokument13 SeitenModule Combustion Engineering-1-2Julie Ann D. GaboNoch keine Bewertungen
- Knowledge Mgmt in BPO: Capturing & Sharing Valuable InsightsDokument3 SeitenKnowledge Mgmt in BPO: Capturing & Sharing Valuable InsightsameetdegreatNoch keine Bewertungen
- Zkihel Ilaye Efera: EducationDokument3 SeitenZkihel Ilaye Efera: EducationezkihelNoch keine Bewertungen
- Lec4 WWW Cs Sjtu Edu CNDokument134 SeitenLec4 WWW Cs Sjtu Edu CNAUSTIN ALTONNoch keine Bewertungen
- Infrared Spectroscopy of FAME in Biodiesel Following DIN 14078 PDFDokument2 SeitenInfrared Spectroscopy of FAME in Biodiesel Following DIN 14078 PDFPedro AluaNoch keine Bewertungen
- Creativity & Innovation Notes - IV - Sem - 2016 PDFDokument31 SeitenCreativity & Innovation Notes - IV - Sem - 2016 PDFPreityTripathi79% (14)
- Crack Detection & RepairDokument5 SeitenCrack Detection & RepairHaftay100% (1)