Das könnte Ihnen auch gefallen
- MATERNAL AND CHILD HEALTH NURSING (8th Edition) - 1-3732-1820-1867Dokument48 SeitenMATERNAL AND CHILD HEALTH NURSING (8th Edition) - 1-3732-1820-1867RON PEARL ANGELIE CADORNANoch keine Bewertungen
- Ntcp-Mop TB CPG 2015Dokument192 SeitenNtcp-Mop TB CPG 2015Val Constantine Say CuaNoch keine Bewertungen
- Pros and Cons About AbortionDokument3 SeitenPros and Cons About AbortionHeru PamitanMinggatt AssalamualaikumNoch keine Bewertungen
- Angelina Alphonce JohoDokument80 SeitenAngelina Alphonce JohoMerlina WijayawatiNoch keine Bewertungen
- 57 74Dokument5 Seiten57 74Lisa Puspadewi SusantoNoch keine Bewertungen
- Obstetric HistoryDokument38 SeitenObstetric HistoryHannah LeianNoch keine Bewertungen
- Chronic Hepatitis BDokument9 SeitenChronic Hepatitis Bmits98Noch keine Bewertungen
- Philippine College of Health Science IncDokument23 SeitenPhilippine College of Health Science Incpeter bruceNoch keine Bewertungen
- An Insight On Poverty Reduction and Health Inequalities in The Philippines: Social Determinants, Constraints, and OpportunitiesDokument84 SeitenAn Insight On Poverty Reduction and Health Inequalities in The Philippines: Social Determinants, Constraints, and OpportunitiesJohn Vincent Pagaddu100% (1)
- AUB Case DiscussionDokument42 SeitenAUB Case DiscussionHafsah G.100% (1)
- JFP 1978 06 v6 I6 The Family Apgar A Proposal For A FamilyDokument9 SeitenJFP 1978 06 v6 I6 The Family Apgar A Proposal For A FamilyMicahNoch keine Bewertungen
- Mcsi Description 1Dokument2 SeitenMcsi Description 1esbat07100% (1)
- FNCP Notes - StudentsDokument9 SeitenFNCP Notes - StudentsAmiel Francisco Reyes100% (1)
- Case 6Dokument7 SeitenCase 6Angel MayNoch keine Bewertungen
- (FCM) 1.1 Tools in Family AssesmentDokument7 Seiten(FCM) 1.1 Tools in Family AssesmentAC BCNoch keine Bewertungen
- Stevens Johnson DiseaseDokument5 SeitenStevens Johnson DiseaseShammy RNNoch keine Bewertungen
- Schistosomiasis Control Program - Department of Health WebsiteDokument2 SeitenSchistosomiasis Control Program - Department of Health WebsiteDud AccNoch keine Bewertungen
- Stem Cells EssayDokument4 SeitenStem Cells EssayalskjdhhNoch keine Bewertungen
- Community-Oriented Primary Care: Historical PerspectiveDokument10 SeitenCommunity-Oriented Primary Care: Historical PerspectiveJemie Talosig Narag-ManzanoNoch keine Bewertungen
- Family-Oriented Primary CareDokument3 SeitenFamily-Oriented Primary Careأحمد خيري التميمي0% (1)
- Case Study - Incomplete Abortion Related To APSDokument8 SeitenCase Study - Incomplete Abortion Related To APSRomeo ReyesNoch keine Bewertungen
- The Problem and Its BackgroundDokument46 SeitenThe Problem and Its Backgroundharoldpaulo100% (1)
- Family Medicine Family CaseDokument17 SeitenFamily Medicine Family Casecorina_oliverNoch keine Bewertungen
- Spinal Cord Injury Case Study (Physical Assessment)Dokument3 SeitenSpinal Cord Injury Case Study (Physical Assessment)TobiDaNoch keine Bewertungen
- The PFC Matrix: ED Marie T. Cruz MD DFMDokument47 SeitenThe PFC Matrix: ED Marie T. Cruz MD DFMEd Marie CruzNoch keine Bewertungen
- Tirado-BSN 4D-Journal Reading Summary and ReflectionDokument4 SeitenTirado-BSN 4D-Journal Reading Summary and ReflectionJeniper Marie Cute29Noch keine Bewertungen
- 10 Community Oriented Primary CareDokument3 Seiten10 Community Oriented Primary CareIrene Veron Bernardo ChicoNoch keine Bewertungen
- PAFP Clinical Pathway For The Diagnosis and Management of Patients With COVID 19 in Family Practice PDFDokument35 SeitenPAFP Clinical Pathway For The Diagnosis and Management of Patients With COVID 19 in Family Practice PDFZaqueo Gutierrez FajardoNoch keine Bewertungen
- Barriers To Physical Activity in Older Adult PDFDokument26 SeitenBarriers To Physical Activity in Older Adult PDFJhoana Rose Joaquin SantosNoch keine Bewertungen
- FCM1 - S01-T01-Introduction To FCM and The Five Star Doctor PDFDokument6 SeitenFCM1 - S01-T01-Introduction To FCM and The Five Star Doctor PDFGianne OgacoNoch keine Bewertungen
- Philippines TB CP Guidelines 2006Dokument151 SeitenPhilippines TB CP Guidelines 2006wiltechworksNoch keine Bewertungen
- A Case Study of Polycystic Ovarian SyndromeDokument42 SeitenA Case Study of Polycystic Ovarian SyndromeDORINNE KINDAONoch keine Bewertungen
- Chronic Suppurative Otitis Media in AdultsDokument10 SeitenChronic Suppurative Otitis Media in AdultsRstadam TagalogNoch keine Bewertungen
- Health Promotion and Health EducationDokument4 SeitenHealth Promotion and Health EducationMaria Christina SalazarNoch keine Bewertungen
- DOH ProgramsDokument6 SeitenDOH ProgramsMichael VillavertNoch keine Bewertungen
- Knowledge and Practices of Pregnant Women RegardinDokument13 SeitenKnowledge and Practices of Pregnant Women RegardinDrPreeti Thakur ChouhanNoch keine Bewertungen
- 02 Family Oriented Medical RecordDokument4 Seiten02 Family Oriented Medical RecordFernandez-De Ala NicaNoch keine Bewertungen
- CDx-Brgy-704-Final - PDF Version 1Dokument103 SeitenCDx-Brgy-704-Final - PDF Version 1Reymart FernandezNoch keine Bewertungen
- Pain ManagementDokument20 SeitenPain ManagementLis SyuwaibatulNoch keine Bewertungen
- Telenursing and Remote Access Telehealth: CompanyDokument38 SeitenTelenursing and Remote Access Telehealth: Companybeer_ettaa100% (1)
- Cga - 1Dokument19 SeitenCga - 1Kenji Tolero100% (1)
- Spiritual Needs in The Aftermath of A DisasterDokument2 SeitenSpiritual Needs in The Aftermath of A DisasterAnthony BorjaNoch keine Bewertungen
- Approach To Pleural EffusionDokument46 SeitenApproach To Pleural EffusionBaskoro Tri LaksonoNoch keine Bewertungen
- Case StudyDokument49 SeitenCase StudyJang Abd MutalibNoch keine Bewertungen
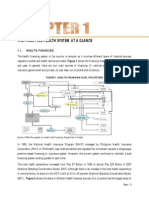
- The Philippine Health System at A GlanceDokument15 SeitenThe Philippine Health System at A GlanceYL LYNoch keine Bewertungen
- Medicine I: Medical History and Physical Examination Grading SheetDokument3 SeitenMedicine I: Medical History and Physical Examination Grading Sheetnanobots37Noch keine Bewertungen
- Antenatal Care Services: by DR - Chinedu Ibeh Thursday, 16 APRIL 2015Dokument81 SeitenAntenatal Care Services: by DR - Chinedu Ibeh Thursday, 16 APRIL 2015SehaRizaNoch keine Bewertungen
- A Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutVon EverandA Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutBewertung: 5 von 5 Sternen5/5 (1)
- Family Life CycleDokument34 SeitenFamily Life CycleKathrina AbastarNoch keine Bewertungen
- Partial CHN211 Week 7Dokument16 SeitenPartial CHN211 Week 7Via Kristel ZapantaNoch keine Bewertungen
- COMMED 0503C Leptospirosis PDFDokument4 SeitenCOMMED 0503C Leptospirosis PDFGabby ElardoNoch keine Bewertungen
- St. Paul University Philippines: School of Nursing and Allied Health Sciences College of NursingDokument5 SeitenSt. Paul University Philippines: School of Nursing and Allied Health Sciences College of NursingChristian UmosoNoch keine Bewertungen
- Family Circle and EcomapDokument15 SeitenFamily Circle and EcomapJam Knows Right100% (1)
- Ebp Synthesis PaperDokument8 SeitenEbp Synthesis Paperapi-404285262Noch keine Bewertungen
- C H N 2:levels of Clientele in CHN: IndividualDokument5 SeitenC H N 2:levels of Clientele in CHN: IndividualFlorence NightingaleNoch keine Bewertungen
- Obstetric Maneuvers For Shoulder Dystocia and Associated Fetal MorbidityDokument5 SeitenObstetric Maneuvers For Shoulder Dystocia and Associated Fetal MorbidityBill HarmanNoch keine Bewertungen
- Malignant Mixed Mullerian Tumor Arising From The UDokument5 SeitenMalignant Mixed Mullerian Tumor Arising From The UAmin IsmailNoch keine Bewertungen
- SCREEMDokument2 SeitenSCREEMDranreb Berylle MasangkayNoch keine Bewertungen
- Turf Toe, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandTurf Toe, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Monstrous HeroesDokument28 SeitenMonstrous HeroesᏩᏕ ᎦᎵᏍᎨᏫ100% (1)
- GYMNASTICShandoutDokument4 SeitenGYMNASTICShandoutRene Jay-ar Morante SegundoNoch keine Bewertungen
- Hyd 04 07 SM T40140 T40170Dokument8 SeitenHyd 04 07 SM T40140 T40170Mohamed Mabrouk100% (1)
- Tournament Rules ManualDokument40 SeitenTournament Rules Manualluis rodriguezNoch keine Bewertungen
- Data Base Crush Gear NitroDokument10 SeitenData Base Crush Gear NitroarieNoch keine Bewertungen
- Session Zero Discussion 4Dokument2 SeitenSession Zero Discussion 4zairellemiguelNoch keine Bewertungen
- Top 5 Strumming Patterns OK PDFDokument6 SeitenTop 5 Strumming Patterns OK PDFjumpin_aroundNoch keine Bewertungen
- Pei and 03 Ab Unit5Dokument6 SeitenPei and 03 Ab Unit5Bene HispalisNoch keine Bewertungen
- Chess For KidsDokument183 SeitenChess For KidsAdail Junior86% (7)
- The Constitution of The League of Hard KnoxDokument3 SeitenThe Constitution of The League of Hard KnoxAndrea LucasNoch keine Bewertungen
- Inuyasha After Final ActDokument18 SeitenInuyasha After Final ActKsesshumaru DemonNoch keine Bewertungen
- Hero Academia: Watched Anime Romcom Status HOT! Anime StatusDokument3 SeitenHero Academia: Watched Anime Romcom Status HOT! Anime StatusJeric GeronaNoch keine Bewertungen
- Yx 160Dokument42 SeitenYx 160Ahzar AhzarNoch keine Bewertungen
- Dragonlanec DLQ1 Knight's SwordDokument38 SeitenDragonlanec DLQ1 Knight's SwordSebastien DumontNoch keine Bewertungen
- UGD-gearbox DatasheetDokument3 SeitenUGD-gearbox DatasheetPrem YadavNoch keine Bewertungen
- Wordle - The New York Times 3Dokument1 SeiteWordle - The New York Times 3espinosakristienssiNoch keine Bewertungen
- Fingerstyle Guitar - Fingerpicking Patterns and ExercisesDokument42 SeitenFingerstyle Guitar - Fingerpicking Patterns and ExercisesSeminario Lipa100% (6)
- UNIT - 6: Test & Measurement in Sports..!! Along-With Important QuestionsDokument68 SeitenUNIT - 6: Test & Measurement in Sports..!! Along-With Important QuestionsMahima Famous100% (1)
- Breaking Muscle-Special Forces Workouts Cycle 2Dokument35 SeitenBreaking Muscle-Special Forces Workouts Cycle 2John Long100% (2)
- Worksheet - Projectile Motion 2 Solution-2Dokument5 SeitenWorksheet - Projectile Motion 2 Solution-2mjdaihmohammedNoch keine Bewertungen
- 1000 PDFDokument34 Seiten1000 PDFMykola TitovNoch keine Bewertungen
- Masks - Harbinger PlaybookDokument2 SeitenMasks - Harbinger PlaybookJavierEtcheverry100% (2)
- Brembo CatalogDokument54 SeitenBrembo CatalogHandrito YudoNoch keine Bewertungen
- Mahabaratha Tatparya Nirnaya: - Introduction by Prof.K.T.PandurangiDokument2 SeitenMahabaratha Tatparya Nirnaya: - Introduction by Prof.K.T.PandurangiindianNoch keine Bewertungen
- Chord Always Be My BabyDokument3 SeitenChord Always Be My BabyAbbhe DevillNoch keine Bewertungen
- Parts PDFDokument823 SeitenParts PDFCesar Antonio AntillancaNoch keine Bewertungen
- Sonic The Hedgehog Unofficial RPGDokument13 SeitenSonic The Hedgehog Unofficial RPGDustin McAlister0% (2)
- Ford 1998 4.0 Intake Gasket ReplacementDokument10 SeitenFord 1998 4.0 Intake Gasket Replacementmarvstewart100% (1)
- New Text DocumentDokument26 SeitenNew Text DocumentMArkoNoch keine Bewertungen
- VBF 21Dokument6 SeitenVBF 21harishupretiNoch keine Bewertungen