Das könnte Ihnen auch gefallen
- Diagnosis and Treatment of Children With Autism Spectrum DisordersVon EverandDiagnosis and Treatment of Children With Autism Spectrum DisordersBewertung: 5 von 5 Sternen5/5 (1)
- Psychological Well-Being and Coping in Mothers of Youths With Autism, Down Syndrome, or Fragile X SyndromeDokument18 SeitenPsychological Well-Being and Coping in Mothers of Youths With Autism, Down Syndrome, or Fragile X SyndromeAncuța IfteneNoch keine Bewertungen
- O'Brien 2007 (1) - 1Dokument22 SeitenO'Brien 2007 (1) - 1Bro BroNoch keine Bewertungen
- 2016 O Neill Anxiety and Depression Symptomatology in Adult Siblings of Individuals With Different Developmental Disability DiagnosesDokument10 Seiten2016 O Neill Anxiety and Depression Symptomatology in Adult Siblings of Individuals With Different Developmental Disability Diagnosesnermal93Noch keine Bewertungen
- Meta-Analysis of Comparative Studies of Depression in Mothers of Children With and Without Developmental DisabilitiesDokument15 SeitenMeta-Analysis of Comparative Studies of Depression in Mothers of Children With and Without Developmental DisabilitiesLudmila MenezesNoch keine Bewertungen
- Sibling Influences On Theory of Mind Development For Children With ASDDokument7 SeitenSibling Influences On Theory of Mind Development For Children With ASDAnonymous 75M6uB3Ow100% (1)
- Adjustment, Sibling Problems and Coping Strategies of Brothers and Sisters of Children With Autistic Spectrum DisorderDokument11 SeitenAdjustment, Sibling Problems and Coping Strategies of Brothers and Sisters of Children With Autistic Spectrum DisorderkatanitaNoch keine Bewertungen
- Content ServerDokument13 SeitenContent ServerMelindaDuciagNoch keine Bewertungen
- Parents of Adults With An Intellectual Disability: Monica CuskellyDokument6 SeitenParents of Adults With An Intellectual Disability: Monica CuskellyShirley ChavarríaNoch keine Bewertungen
- 0 RIA Parents and Professional ViewsDokument11 Seiten0 RIA Parents and Professional ViewsAncuța IfteneNoch keine Bewertungen
- Template - Artikel 1 - No Absen 1 S.D 8Dokument12 SeitenTemplate - Artikel 1 - No Absen 1 S.D 8Angelica EarlyanaNoch keine Bewertungen
- Adams - 2018 - Well-Being in Mothers of Children With Rare Genetic SyndromesDokument13 SeitenAdams - 2018 - Well-Being in Mothers of Children With Rare Genetic SyndromesPetrutaNoch keine Bewertungen
- Family Conflict Impacts Autism SymptomsDokument14 SeitenFamily Conflict Impacts Autism SymptomslboninsouzaNoch keine Bewertungen
- Down Syndrome Research Paper ThesisDokument4 SeitenDown Syndrome Research Paper Thesisfvg4mn01100% (1)
- Selective Mutism in Children: Comparison To Youths With and Without Anxiety DisordersDokument8 SeitenSelective Mutism in Children: Comparison To Youths With and Without Anxiety DisorderspaulNoch keine Bewertungen
- Experiencesof African American Mothers AutismDokument18 SeitenExperiencesof African American Mothers AutismKhafifah MadiaNoch keine Bewertungen
- Optimism, Social Support, and Well-Being in Mothers of Children With Autism Spectrum DisorderDokument11 SeitenOptimism, Social Support, and Well-Being in Mothers of Children With Autism Spectrum DisorderTThay BBrandNoch keine Bewertungen
- 1 s2.0 S0891422219300691 MainDokument9 Seiten1 s2.0 S0891422219300691 MainMudassar AzizNoch keine Bewertungen
- Journal of Anxiety Disorders: Ann E. Layne, Debra H. Bernat, Andrea M. Victor, Gail A. BernsteinDokument7 SeitenJournal of Anxiety Disorders: Ann E. Layne, Debra H. Bernat, Andrea M. Victor, Gail A. BernsteinMelina Defita SariNoch keine Bewertungen
- International Journal of Humanities and Social Science Invention (IJHSSI)Dokument19 SeitenInternational Journal of Humanities and Social Science Invention (IJHSSI)inventionjournalsNoch keine Bewertungen
- Bartov 2018Dokument12 SeitenBartov 2018Thaís Spall ChaximNoch keine Bewertungen
- Parenting Children with Down Syndrome: Understanding Societal InfluencesDokument10 SeitenParenting Children with Down Syndrome: Understanding Societal InfluencesYulia AfresilNoch keine Bewertungen
- Hill 2009Dokument12 SeitenHill 2009Frontier JuniorNoch keine Bewertungen
- Mental DisabilitiesDokument11 SeitenMental DisabilitiesKaren IrasemaNoch keine Bewertungen
- GROWING UP WITH GRIEFDokument20 SeitenGROWING UP WITH GRIEFfernandamancilhapsiNoch keine Bewertungen
- ASD Parent Stress Article 2004Dokument12 SeitenASD Parent Stress Article 2004DhEg LieShh WowhNoch keine Bewertungen
- Emotion Knowledge in Young Neglected Children: Margaret W. SullivanDokument6 SeitenEmotion Knowledge in Young Neglected Children: Margaret W. SullivanditeABCNoch keine Bewertungen
- Issues in The Social and Emotional Adjustment of Gifted ChildrenDokument12 SeitenIssues in The Social and Emotional Adjustment of Gifted Childrenapi-301904910Noch keine Bewertungen
- Annotated BibliographyDokument3 SeitenAnnotated Bibliographyapi-469841810Noch keine Bewertungen
- 1.parental DepressionDokument17 Seiten1.parental DepressionSeby NurakNoch keine Bewertungen
- Attachment Theory in Adolescence and AdulthoodDokument6 SeitenAttachment Theory in Adolescence and AdulthoodsimuNoch keine Bewertungen
- Những tác động trong cuộc sống của việc nuôi dạy con cái khuyết tậtDokument22 SeitenNhững tác động trong cuộc sống của việc nuôi dạy con cái khuyết tậtDo ThuyNoch keine Bewertungen
- PocinhoDokument10 SeitenPocinhoriris nurhanifiyantiNoch keine Bewertungen
- Wiley Society For Research in Child DevelopmentDokument17 SeitenWiley Society For Research in Child DevelopmentXiao CiNoch keine Bewertungen
- MulliganDokument21 SeitenMulliganJG Du PlessisNoch keine Bewertungen
- Representations of The Caregiver-Child Relationship and of The Self, and Emotion Regulation in The Narratives of Young Children Whose Mothers Have BPDDokument20 SeitenRepresentations of The Caregiver-Child Relationship and of The Self, and Emotion Regulation in The Narratives of Young Children Whose Mothers Have BPDme13Noch keine Bewertungen
- Hope and Worry AutismDokument7 SeitenHope and Worry Autismapi-87092797Noch keine Bewertungen
- Maladaptive Behavior Down Syndrome PDFDokument10 SeitenMaladaptive Behavior Down Syndrome PDFsimplerain17893Noch keine Bewertungen
- Resilience in Family Members of Persons With Autism Spectrum Disorder: A Review of The LiteratureDokument8 SeitenResilience in Family Members of Persons With Autism Spectrum Disorder: A Review of The Literatureana lara SantosNoch keine Bewertungen
- Mother-Child Relationships, Family Context, and Child Characteristics As Predictors of Anxiety Symptoms in Middle ChildhoodDokument13 SeitenMother-Child Relationships, Family Context, and Child Characteristics As Predictors of Anxiety Symptoms in Middle ChildhoodNina GarfoNoch keine Bewertungen
- CORSANO-Typically Developing Adolescents' Experience of Growing Up With A Brother With An Autism Spectrum DisorderDokument12 SeitenCORSANO-Typically Developing Adolescents' Experience of Growing Up With A Brother With An Autism Spectrum DisorderwNoch keine Bewertungen
- Articole Stiintifice PsihologieDokument10 SeitenArticole Stiintifice PsihologieMircea RaduNoch keine Bewertungen
- Predictors of Parental Stress in Mothers of Young Children With Hearing LossDokument17 SeitenPredictors of Parental Stress in Mothers of Young Children With Hearing LossPija RamliNoch keine Bewertungen
- Families of Children With Down Syndrome What We KNDokument10 SeitenFamilies of Children With Down Syndrome What We KNroneldayo62Noch keine Bewertungen
- Mental Health of Transgender ChildrenDokument10 SeitenMental Health of Transgender ChildrenMarian Mario SpagnuoloNoch keine Bewertungen
- Rogers 2003Dokument12 SeitenRogers 2003dimasprastiiaNoch keine Bewertungen
- Poverty and BrainDokument24 SeitenPoverty and BrainManuel Guerrero GómezNoch keine Bewertungen
- Falsas DenunciasDokument22 SeitenFalsas DenunciasmayeNoch keine Bewertungen
- Children in Foster Care: A Vulnerable Population at Risk: Delilah Bruskas, RN, MNDokument8 SeitenChildren in Foster Care: A Vulnerable Population at Risk: Delilah Bruskas, RN, MNMohamed AbdulqadirNoch keine Bewertungen
- Anxiety Levels in Children With Autism Spectrum Disorder A Meta AnalysisDokument15 SeitenAnxiety Levels in Children With Autism Spectrum Disorder A Meta AnalysisvaishnaviNoch keine Bewertungen
- Content ServerDokument18 SeitenContent ServerMelindaDuciagNoch keine Bewertungen
- The Adjustment of Nondisabled Adolescent Siblings of Individuals With Autism Spectrum Disorder in The HomeDokument18 SeitenThe Adjustment of Nondisabled Adolescent Siblings of Individuals With Autism Spectrum Disorder in The HomeAutism Society Philippines100% (4)
- Families of Children With Rett Syndrome PDFDokument17 SeitenFamilies of Children With Rett Syndrome PDFOtono ExtranoNoch keine Bewertungen
- 2004 Psychosocial Determinants of Behaviour ProblemsDokument10 Seiten2004 Psychosocial Determinants of Behaviour ProblemsMariajosé CaroNoch keine Bewertungen
- Joint Attention and Disorganized Attachment Status in Infants at RiskDokument14 SeitenJoint Attention and Disorganized Attachment Status in Infants at RiskCarolina Saavedra MellaNoch keine Bewertungen
- Workings of The Lit ReviewDokument24 SeitenWorkings of The Lit Reviewapi-299743021Noch keine Bewertungen
- Responses To The Negative Emotions of Others by Autistic, Mentally Retarded, and Normal ChildrenDokument13 SeitenResponses To The Negative Emotions of Others by Autistic, Mentally Retarded, and Normal ChildrenBIANA-MARIA MACOVEINoch keine Bewertungen
- NIH Public Access: Author ManuscriptDokument9 SeitenNIH Public Access: Author ManuscriptDanielaLealNoch keine Bewertungen
- nuttall2018Dokument11 Seitennuttall2018Réka SnakóczkiNoch keine Bewertungen
- Support, Communication, and Hardiness in Families With Children With DisabilitiesDokument17 SeitenSupport, Communication, and Hardiness in Families With Children With DisabilitiesAnnisa Dwi NoviantyNoch keine Bewertungen
- Edtpa 2nd Lesson PlanDokument5 SeitenEdtpa 2nd Lesson Planapi-297045693Noch keine Bewertungen
- Ward Security Application Form Nov 2011Dokument14 SeitenWard Security Application Form Nov 2011Wajid Iqbal100% (1)
- Educating Learners Chapter 9Dokument50 SeitenEducating Learners Chapter 9Allyssa Lorraine PrudencioNoch keine Bewertungen
- Roles Functions Advice NoteDokument27 SeitenRoles Functions Advice NoteCristina Lorena Grasu100% (1)
- Cesc 12 - Q1 - M17Dokument14 SeitenCesc 12 - Q1 - M17jayson babaranNoch keine Bewertungen
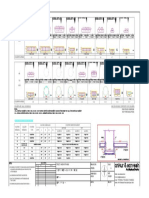
- M30 Reinforced Concrete Column Design DetailsDokument1 SeiteM30 Reinforced Concrete Column Design DetailsCMM INFRAPROJECTS LTDNoch keine Bewertungen
- GESP FORMS With Suggested Movs For DRRMDokument64 SeitenGESP FORMS With Suggested Movs For DRRMEnen DagumampanNoch keine Bewertungen
- Mental Health Care and Human Rights - NHRC IndiaDokument472 SeitenMental Health Care and Human Rights - NHRC IndiaVaishnavi JayakumarNoch keine Bewertungen
- Sexuality Re MasturbationDokument17 SeitenSexuality Re MasturbationMaria AlvanouNoch keine Bewertungen
- Demons of The Body and MindDokument245 SeitenDemons of The Body and MindPerekatypole100% (5)
- Final ProjectDokument27 SeitenFinal Projectapi-284802869Noch keine Bewertungen
- PTSDDokument30 SeitenPTSDVohn Andrae SarmientoNoch keine Bewertungen
- Work History Report SSA-3369-BKDokument10 SeitenWork History Report SSA-3369-BKLevine BenjaminNoch keine Bewertungen
- Task 3 - Special EducationDokument3 SeitenTask 3 - Special EducationShainna BaloteNoch keine Bewertungen
- Assignment - Inclusive EducationDokument13 SeitenAssignment - Inclusive Educationapi-357686594Noch keine Bewertungen
- Thesis ReportDokument11 SeitenThesis ReportPooja Sharma100% (2)
- Physical Disabilities Reflection No. 8Dokument3 SeitenPhysical Disabilities Reflection No. 8Carlo TunongNoch keine Bewertungen
- Teacher Efficacy Managing Preschool Behavior ChallengesDokument12 SeitenTeacher Efficacy Managing Preschool Behavior ChallengesAnonymous TLQn9SoRRbNoch keine Bewertungen
- Bipolar Disorder: Causes, Symptoms and Famous FiguresDokument54 SeitenBipolar Disorder: Causes, Symptoms and Famous Figuresleanne yangNoch keine Bewertungen
- 3 Schizophrenia AssessmentDokument36 Seiten3 Schizophrenia AssessmentArvindhanNoch keine Bewertungen
- Case Studies in Social Enterprise: Counterpart International's ExperienceDokument59 SeitenCase Studies in Social Enterprise: Counterpart International's ExperienceRozina ImtiazNoch keine Bewertungen
- 1 - 50 Ways Bias Fundamentals - English - v1 CompressedDokument67 Seiten1 - 50 Ways Bias Fundamentals - English - v1 CompressedMaryReyesNoch keine Bewertungen
- Accessibility For Disabled in Public TransportatioDokument9 SeitenAccessibility For Disabled in Public TransportatioIrfan Nurfauzan IskandarNoch keine Bewertungen
- Crtique On Finland SPEDDokument10 SeitenCrtique On Finland SPEDErvin SalupareNoch keine Bewertungen
- Developmental Disabilities and Their Management / Orthodontic Courses by Indian Dental AcademyDokument71 SeitenDevelopmental Disabilities and Their Management / Orthodontic Courses by Indian Dental Academyindian dental academyNoch keine Bewertungen
- The Brain: Understanding Psychological Disorders Through NeuroimagingDokument14 SeitenThe Brain: Understanding Psychological Disorders Through NeuroimagingSiti SarahNoch keine Bewertungen
- Disability World 25Dokument264 SeitenDisability World 25Ezekiel T. MostieroNoch keine Bewertungen
- Schizophrenia in Old AgeDokument21 SeitenSchizophrenia in Old AgeAyedh TalhaNoch keine Bewertungen
- ICF-Curriculum Modules v1 Approved FINAL 1Dokument12 SeitenICF-Curriculum Modules v1 Approved FINAL 1HariNoch keine Bewertungen
- Fabric Cutter Amh q1510 v1.0Dokument31 SeitenFabric Cutter Amh q1510 v1.0Puneet KaurNoch keine Bewertungen
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesVon EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesBewertung: 5 von 5 Sternen5/5 (70)
- The Somatic Psychotherapy Toolbox: A Comprehensive Guide to Healing Trauma and StressVon EverandThe Somatic Psychotherapy Toolbox: A Comprehensive Guide to Healing Trauma and StressNoch keine Bewertungen
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryVon EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryBewertung: 4.5 von 5 Sternen4.5/5 (157)
- The Happiness Trap: How to Stop Struggling and Start LivingVon EverandThe Happiness Trap: How to Stop Struggling and Start LivingBewertung: 4 von 5 Sternen4/5 (1)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveVon EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveBewertung: 4 von 5 Sternen4/5 (249)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsVon EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsBewertung: 4.5 von 5 Sternen4.5/5 (38)
- The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk: Key Takeaways, Summary & AnalysisVon EverandThe Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (2)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeVon EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeBewertung: 4.5 von 5 Sternen4.5/5 (140)
- An Autobiography of Trauma: A Healing JourneyVon EverandAn Autobiography of Trauma: A Healing JourneyBewertung: 5 von 5 Sternen5/5 (1)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDVon EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDBewertung: 4.5 von 5 Sternen4.5/5 (167)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreVon EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreBewertung: 5 von 5 Sternen5/5 (17)
- Fighting Words Devotional: 100 Days of Speaking Truth into the DarknessVon EverandFighting Words Devotional: 100 Days of Speaking Truth into the DarknessBewertung: 5 von 5 Sternen5/5 (6)
- BORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONVon EverandBORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONBewertung: 4.5 von 5 Sternen4.5/5 (24)
- Winning the War in Your Mind: Change Your Thinking, Change Your LifeVon EverandWinning the War in Your Mind: Change Your Thinking, Change Your LifeBewertung: 5 von 5 Sternen5/5 (553)
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaVon EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaBewertung: 4.5 von 5 Sternen4.5/5 (56)
- Overcoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsVon EverandOvercoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsBewertung: 4.5 von 5 Sternen4.5/5 (48)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisVon EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (9)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionVon EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNoch keine Bewertungen
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouVon EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouNoch keine Bewertungen
- Insecure in Love: How Anxious Attachment Can Make You Feel Jealous, Needy, and Worried and What You Can Do About ItVon EverandInsecure in Love: How Anxious Attachment Can Make You Feel Jealous, Needy, and Worried and What You Can Do About ItBewertung: 4.5 von 5 Sternen4.5/5 (84)
- Emotional Detox for Anxiety: 7 Steps to Release Anxiety and Energize JoyVon EverandEmotional Detox for Anxiety: 7 Steps to Release Anxiety and Energize JoyBewertung: 5 von 5 Sternen5/5 (6)
- Smart Phone Dumb Phone: Free Yourself from Digital AddictionVon EverandSmart Phone Dumb Phone: Free Yourself from Digital AddictionBewertung: 5 von 5 Sternen5/5 (11)
- Triggers: How We Can Stop Reacting and Start HealingVon EverandTriggers: How We Can Stop Reacting and Start HealingBewertung: 5 von 5 Sternen5/5 (57)
- The Anxiety Healer's Guide: Coping Strategies and Mindfulness Techniques to Calm the Mind and BodyVon EverandThe Anxiety Healer's Guide: Coping Strategies and Mindfulness Techniques to Calm the Mind and BodyNoch keine Bewertungen