Beruflich Dokumente
Kultur Dokumente
Diabetes e Hipertrigliceridemia
Hochgeladen von
Paula CardonaOriginaltitel
Copyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
Diabetes e Hipertrigliceridemia
Hochgeladen von
Paula CardonaCopyright:
Verfügbare Formate
Clinical Therapeutics/Volume 35, Number 5, 2013
Inpatient Management of Diabetes and Hyperglycemia
Magdalena Bogun, MD; and Silvio E. Inzucchi, MD
Section of Endocrinology, Yale University School of Medicine, New Haven, Connecticut
ABSTRACT tality increased progressively as mean blood glucose
Illness, particularly when severe, leads to increased concentrations increased. For example, mortality was
concentrations of counter-regulatory factors which in- 9.6% in patients whose mean ICU glucose concentra-
duce insulin resistance and predispose patients to stress tion fell between 80 and 99 mg/dL but was 4-fold
hyperglycemia. Elevated glucose concentrations are higher (42.5%) in those whose mean glucose exceeded
common in hospitalized patients, both those with as 300 mg/dL. Similarly, Kosiborod et al2 in 2008 re-
well as without recognized diabetes. Substantial data ported that in patients hospitalized for acute myocar-
has emerged over the past decade that quality glucose dial infarction (AMI), mortality increased progres-
management in these individuals actually improves sively with every 10-mg/dL glucose increase above 120
clinical outcomes. Controlling glucose in this setting is mg/dL, after controlling for a variety of important clin-
challenging, given the phenotypic variability amongst ical variables (Slide 1). This relationship was particu-
patients, with fluctuating courses of acute illnesses and larly striking in those without an antecedent history of
unpredictable nutritional schedules. We review the ev- diabetes. These data were consistent with those from
idence basis that has informed national standards and an early observational study from Umpierrez et al3 in-
glucose targets in both critically and non-critically ill volving 2030 ICU patients, which concluded that those
patients. In the intensive care setting, insulin infusions
with newly identified hyperglycemia had significantly
are now widely endorsed to quickly achieve and main-
higher mortality (31%) than did patients with known
tain glucose control. On the hospital wards, physiolog-
diabetes (11%). Notably, in the Kosiborod analysis,4
ical subcutaneous insulin therapy, incorporating both
an increase in mortality was also seen when mean
basal and nutritional components, is emerging as the
blood glucose fell below 70 mg/dL.
optimal treatment strategy. The transition to outpa-
These studies raise the possibility that controlling
tient care is another important aspect of any hospital
blood glucose in the setting of critical illness may im-
glycemic management program. (Clin Ther. 2013;35:
prove clinical outcomes but also that overly intensive
724733) 2013 Published by Elsevier HS Journals,
Inc. approaches might be counterproductive. Yet observa-
Key words: diabetes, hyperglycemia, hospital, inpa- tional data alone can be misleading and are influenced
tient, critical care, insulin infusion by confounding factors that are either not easily as-
sessed or not initially considered to be relevant by the
investigators. So, it remained unknown as to whether
INTRODUCTION hyperglycemia merely serves as a marker of poor clin-
Hyperglycemia in hospitalized patients with or with- ical outcomes or represents a true mediator of these
out overt diabetes presents complex management is- adverse events. It is well-recognized that illness by it-
sues. Questions arise about the degree of intensity to self, particularly when severe, leads to stress hyper-
which glucose levels should be maintained in the criti- glycemia through the activation of counter-regula-
cal care setting, step-down units, and general medical- tory hormones, primarily cortisol and epinephrine,
surgical wards, as well as the optimal strategies for which increase endogenous glucose production and de-
subsequent transitions to outpatient care. crease glucose uptake into peripheral tissues, while
also elevating circulating levels of free fatty acids
Glucose Control During Critical Care
There is a well-recognized relationship between glu- Accepted for publication April 19, 2013.
cose levels and adverse clinical outcomes in the criti- http://dx.doi.org/10.1016/j.clinthera.2013.04.008
cally ill. In 2003, Krinsley et al1 reported that in a 0149-2918/$ - see front matter
mixed medical-surgical intensive care unit (ICU), mor- 2013 Published by Elsevier HS Journals, Inc.
724 Volume 35 Number 5
M. Bogun and S.E. Inzucchi
Mean Glucose & In-Hospital Mortality in Patients with AMI
20
No Diabetes
All Patients
Diabetes
15
Odds Ratio
10
N = 16,871
1
0
t 70
90 to 0
10 to 90
11 to < 00
12 to 10
13 to 20
14 to 30
15 to 40
16 to 50
17 to 60
18 to < 70
19 to 80
20 to 90
21 to 00
22 to 10
23 to < 20
24 to 30
25 to < 40
26 to 50
27 to 60
28 to 70
29 to < 80
to 0
3 0
00
80 o <8
0 29
0
70 <
<
0 <1
0 1
0 <1
0 <1
0 <1
0 <1
0 <1
0 <1
0 1
0 <1
0 <2
0 <2
0 <2
0 2
0 <2
0 2
0 <2
0 <2
0 <2
<3
Mean BG (mg/dL)
(Reference: Mean BG 100110 mg/dl)
(Referance: Mean BG 100-110 mg/dl)
Slide 1. Relationship between mean glucose levels and mortality during hospitalization for nearly 17,000 acute
myocardial infarction patients. Hyperglycemia is associated with more adverse outcomes, especially in non-
diabetic individuals. Reprinted with permission from Kosiborod M et al. Circulation 2008;117:1018 1027.2
through the stimulation of lipolysis (Slide 2). Conversely, tion, 66%; P 0.01). Impressively, the annual rates of
increased glucose and fatty acids may secondarily exac- deep sternal wound infections in diabetic patients at the
erbate illness through altered tissue metabolism, oxida- end of the study had reached the rates similar to those in
tive stress, hypercoagulability, and suppressed immunity nondiabetic individuals. The nonrandomized nature of
and wound healing. this study, however, limited the conclusiveness of its
The first study to explore the notion of controlling findings.
glucose in the ICU to improve patient outcomes was The DIGAMI (Diabetes Insulin-Glucose Infusion in
conducted by cardiothoracic surgeons, led by Fu- Acute Myocardial Infarction) study6 examined the
nary.5 In this nonrandomized trial, patients under- short- and long-term effects of intensive insulin treat-
going cardiac surgery were placed on an insulin-in- ment in patients with diabetes during and soon after
fusion regimen for 3 days postoperatively, targeting AMI. A total of 360 patients were randomly assigned
a glucose level of 151 to 200 mg/dL. Their outcomes within 24 hours of admission to receive an intravenous
were compared to those from a historical control infusion of insulin (and glucose) for 48 hours, with a
group who were mainly managed conventionally with target blood glucose level of 126 to 196 mg/dL, fol-
subcutaneous regular human insulin (every 4 hours on a lowed by multidose subcutaneous insulin injections for
sliding scale with a target of 200 mg/dL). Deep sternal 3 months. A total of 314 patients in the control group
wound infections occurred in 0.8% of the study group received conventional diabetes care. An 11% absolute
and in 2.0% of the controls (relative risk [RR] reduc- and a 28% relative mortality risk reduction was dem-
May 2013 725
Clinical Therapeutics
cemic range (80 110 mg/dL) by intravenous insulin infu-
Illness leads to stress hyperglycemia sion. The conventional-treatment group were targeted
Illness between 180 and 200 mg/dL, with IV insulin being ad-
ministered only if glucose exceeded 215 mg/dL; other-
wise, intermittent subcutaneous injections of regular hu-
Stress hormones Glucose Hemodynamic insult
cortisol, epinephrine Production Electrolyte losses man insulin were used. At the conclusion of the trial,
Oxidative stress those in the intensive-treatment group had significantly
+ Myocardial injury
Glucose FFAs Hypercoagulability fewer deaths in the ICU compared with the conventional-
Fatty Acids Altered immunity
treatment group (63/783 vs 35/765; P 0.04), a RR
Wound healing
Inflammation reduction of 42% (P 0.04). Intensive glycemic manage-
Endothelial function
ment was also associated with a 34% reduction in total
Glucose Uptake
in-hospital mortality (55/764 vs 85/783; P 0.01) in
Lipolysis
FFAs total in-hospital patients (Slide 3). This widely publicized
Stress hyperglycemia may also exacerbate illness.
study has been credited with leading to a major change in
Slide 2. Schematic overview of the relationship be- practice in ICUs across the United States, with many in-
tween stress hyperglycemia and illness. stitutions implementing similar intensive glucose-man-
Through counter-regulatory hormones, ill- agement protocols. Notably, however, in a follow-up
ness promotes increased circulating glucose study11 from this group involving their medical ICU, no
and free fatty acid concentrations. These, in mortality benefit could be demonstrated with intensive
turn, theoretically, could exacerbate illness insulin therapy, although in a predetermined group of
through the intermediary effects listed. patients with longer ICU stays (5 days), mortality was
reduced from 26.3% to 16.8% (P 0.01).
Subsequent to the Leuven investigations, several other
onstrated after 5 years in the intensive insulin therapy studies published from a variety of critical care settings
group, with a predetermined low-risk subgroup (based could not confirm the initial encouraging findings.12,13
on severity of AMI presentation and no history of in- The largest of these, NICE-SUGAR (Normoglycaemia in
sulin use) showing even greater effects (15% and 51%, Intensive Care Evaluation and Survival Using Glucose
respectively). Most of the benefit was apparent in the Algorithm Regulation),12 suggested that intensive glu-
first month of treatment, suggesting some influence cose control with intravenous insulin (target, 81108 mg/
from the immediate infusion of insulin. The survival dL) might increase mortality compared with maintaining
curves tended to separate further over time, implying glycemia in the more moderate range of 140 to 180
an ongoing benefit from intensive treatment. The in- mg/dL through conventional methods (Slide 4). The rea-
vestigators concluded that intensive insulin therapy son for the higher mortality in the active-treatment group
might be an appropriate treatment for diabetic patients in NICE-SUGAR has never been fully elucidated. One
at the time of acute cardiovascular events. However, theory relates to the much higher rate of severely high
subsequent studies (HI-5 [Hyperglycemia: Intensive glucose levels (40 mg/dL) in the intensive-treatment
Insulin Infusion in Infarction],7 DIGAMI-2 [diabe- group (6.8% vs 0.5%), although a cause-and-effect rela-
tes mellitus and acute myocardial infarction],8 and tionship could not be confirmed. It should be noted, how-
CREATE-ECLA [Clinical Trial of Metabolic Modula- ever, that a larger number of patients assigned to inten-
tion in Acute Myocardial Infarction Treatment Evalu- sive treatment withdrew early from the study and did not
ation]9) did not replicate these findings, although these receive insulin infusion. Because a per-protocol (or com-
latter investigations were marred by methodologic pleters) analysis of the data has never been published, it
flaws and/or low patient recruitment. remains unclear as to whether those who received inten-
A prospective, randomized, controlled study from sive insulin therapy experienced greater mortality.
Leuven, Belgium, involved 1548 patients who received Griesdale et al13 have since published a meta-anal-
standard or intensive antihyperglycemic treatment after ysis including 26 randomized control trials that as-
admission to a surgical ICU with a preponderance of car- sessed the effects of intensive glucose management, in-
diac surgery patients.10 In the intensive-treatment group, volving a total of 13,567 critically ill patients. Here,
the blood glucose levels were maintained in a strict eugly- the RR (95% CI) for death with more intensive insu-
726 Volume 35 Number 5
M. Bogun and S.E. Inzucchi
Intensive Insulin Therapy in the Surgical ICU: The Leuven Study
A 100 B 100
96 96
Intensive treatment
In-Hospital Survival (%)
Intensive treatment
Survival in ICU (%)
92 92
Conventional treatment
88 88 Conventional treatment
MORTALITY 42% MORTALITY 34%
84 84
P < 0.04 P < 0.01
80 80
0 0
0 20 40 60 80 100 120 140 160 0 50 100 150 200 250
Days After Admission Days After Admission
Slide 3. KaplanMeier survival curves from the Leuven SICU study. More intensive glucose control with IV insulin resulted in
lower ICU and in-hospital mortality among the 1548 patients studied. From N Engl J Med, van den Berghe G,
Wouters P, Weekers R, et al, Intensive insulin therapy in critically ill patients, 3459, 13591367. Copyright 2001
Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.10
NICE-SUGAR Trial: Outcomes
180 1.0
160
Conventional 0.9
Probability of Survival
140
BG, mg/dL
0.8 Conventional
120 Intensive
108 Intensive
0.7
100
P = 0.03
80 0.6
0 0
Base- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 0 10 20 30 40 50 60 70 80 90
line Days After Randomization Days After Randomization
3054 received IIT goal: 81108 mg/dL 90-day mortality: IIT: 829 patients (27.5%), CIT: 751
(time weighted BG = 118 mg/dL) (24.9%)
3050 received CIT goal: <180 mg/dL Absolute mortality difference: 2.6%
(time-weighted BG = 145 mg/dL) (95% CI, 0.44.8)
Odds ratio for death with IIT:
1.14 (95% CI, 1.021.28; P = 0.02)
Slide 4. Glycemic control and KaplanMeier survival curve from the NICE-SUGAR study. Despite lower glucose
levels in the intensive group, mortality was increased. The explanation for this finding has remained
elusive. From N Engl J Med, Finfer S, Chittock DR, Su SY, et al, for the NICE-SUGAR Study Investigators,
Intensive versus conventional glucose control in critically ill patients, 3603, 12831297. Copyright
2009 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.12
May 2013 727
Clinical Therapeutics
New AACE-ADA Consensus
Statement on Inpatient Glycemic Control
ICU Setting NonICU Setting
Insulin infusion preferred Most patients:
Starting threshold not higher than pre-meal BG <140 mg/dL
180 mg/dl random BG <180 mg/dL
Maintain BG 140180 mg/dl More stringent targets may be
(greater benefit likely at lower end of appropriate in stable patients
this range) Less stringent targets may be
Lower targets (not evidence-based) appropriate in patients with severe
may be appropriate in selected comorbidities
patients if already being successfully Scheduled SQ insulin with basal-
achieved nutritional-correction preferred; avoid
<110 NOT recommended prolonged therapy RISS alone
(not safe)
AACE, American Association of Clinical Endocrinologists; ADA, American Diabetes Association;
SQ, subcutaneous; RISS, regular insulin sliding scale.
Slide 5. Major recommendations from the AACE-ADA Consensus Statement on inpatient glycemic control.
Moghissi ES, Korytkowski MT, Di-Nardo M, et al. American Association of Clinical Endocrinologists and
American Diabetes Association consensus statement on inpatient glycemic control. Diabetes Care. 2009;
32:1119 1131.15 and Moghissi ES, Korytkowski MT, Di-Nardo M, et al. American Association of
Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glyce-
mic control. Endocr Pract. 2009;15:353369.26
lin therapy was statistically indistinguishable com- sensus recommendations concerning the management
pared to that with conventional approaches (0.93 of hyperglycemia in the hospital15 (Slide 5). According
[0.831.04]). The RR, however, varied according to to this AACE-ADA statement, which was more mod-
the type of unit, with intensive insulin showing appar- erate in tone than were prior guidelines, intensive glu-
ent benefit in the surgical ICU setting (0.63 [0.44 cose control with insulin infusion should be under-
0.91]) but not in mixed ICUs (0.99 [0.871.12]) or taken in those ICU patients (regardless of prior
medical ICUs (1.00 [0.78 1.28]). Fourteen of those diabetes history) with blood glucose 180 mg/dL, and
trials reported hypoglycemia, and not surprisingly the maintained between 140 and 180 mg/dL, with greater
RR for severe hypoglycemia in the intensive insulin benefit believed to be likely at the lower end of this
therapy group was 6.0 (4.5 8.0). Although earlier tri- range. The consensus panel went on to note that some-
als have linked hypoglycemia to increased mortality, what lower targets (110 140 mg/dL) might be appro-
its cause-and-effect relationship is not clear. Kosiborod priate in select patients but that blood glucose targets
et al14 reported that hypoglycemia is more likely to be a 110 mg/dL could no longer recommended.
predictor of the severity of illness than a direct cause of
mortality. In his study involving hyperglycemic patients Insulin Infusions
during AMI, hypoglycemia was associated with higher A successful intravenous insulin protocol consis-
mortality only in those patients not treated with insulin tently reaches and maintains blood glucose success-
(odds ratio [OR] 2.32 [95% CI, 1.31 4.12]). Those fully within a specified target range while minimizing
who developed hypoglycemia and were being treated hypoglycemia (and providing specific directions for the
with insulin had mortality similar to those who experi- treatment of hypoglycemia if it does occur). The pro-
enced no hypoglycemia (OR 0.92 [0.58 1.45]). tocol should have a clear, nurse-driven algorithm for
These often-conflicting sets of data led the American making temporary corrective changes in the insulin rate
Association of Clinical Endocrinology (AACE) and the as a patients glucose levels and degree of insulin sensitiv-
American Diabetes Association (ADA) to develop con- ity change. The most successful protocols incorporate not
728 Volume 35 Number 5
M. Bogun and S.E. Inzucchi
Yale Adult ICU Insulin Infusion Protocol (IIP)
Slide 6. The Yale Insulin Infusion Protocol. Reprinted with permission from Shetty S, Inzucchi SE, Goldberg PA,
et al. Adapting to the new consensus guidelines for managing hyperglycemia during critical illness: the
updated Yale insulin infusion protocol. Endocr Pract. 2012;18:363370.17
only the absolute blood glucose level but also its rate of glucose is then checked every hour; the subsequent fre-
change from prior values, as well as the current insulin quency of monitoring can be decreased if 3 consecutive
infusion rate. Ideally, the delineation of specific measures findings are within target. In our published initial co-
for the transition to subcutaneous insulin that will ulti- hort of 90 patients, the protocol achieved a median
mately be required in most patients should be incorpo- blood glucose of 150 mg/dL (range, 127180 mg/dL),
rated. These instructions would necessarily include the with a low rate of severe hypoglycemia (0.01% of glu-
initial doses and types and timing of insulin injections. cose measurements and 1.7% of patients). Notably,
Wilson et al16 compared 12 published protocols in a these results compare favorably with those in the stan-
sample patient and reported great variability in target dard-therapy groups in the largest randomized trials of
ranges, thresholds for insulin infusion initiation, initial intensive insulin therapy (mean of 2.1% from refer-
infusion rates, and the frequency and intensity of ad- ences 10 12 and 18 20).
justments, with markedly different glycemic outcomes
predicted. The insulin-infusion protocol in use at our Glucose Control on General Medical-Surgical
institution (Slide 6).17 in adult ICU patients recom- Wards
mends starting the insulin infusion when 2 consecutive Much less is known about the impact of acute gly-
blood glucose readings exceed 180 mg/dL (the target cemic control in the non critical care settingwhich
range is 120 160 mg/dL). This target was chosen to be encompasses the majority of all hospitalized patients.
slightly lower than the AACE-ADA target because ex- As in the ICU, many observational studies have linked
perience with older versions of our protocol resulted in hyperglycemia to adverse clinical outcomes,21,22 but
mean blood glucose levels in the upper end of the target the same concerns regarding glucose being a marker as
ranges. We therefore believed that mean blood glucose opposed to a mediator of complications remain. For
closer to 140 to 150 mg/dL (as intimated by the guide- example, Baker et al21 studied 433 patients with
lines) was more desirable than one closer to 170 to 180 acute exacerbations of chronic obstructive pulmo-
mg/dL. The infusion is adjusted in increments of 0.5 nary disease and found that the absolute risk for
U/h. The initial infusion rate is preceded by a bolus, adverse outcomes (death or prolonged stay) was in-
with both calculated by dividing the baseline glucose creased by 15% per 18-mg/dL increase in glucose
level by 100, rounded to the nearest 0.5 U. The blood level. In the perioperative setting, Pomposelli et al22
May 2013 729
Clinical Therapeutics
Postoperative Complications in Insulin Glargine + Insulin Glulisine vs SSI
30
P = 0.003 Insulin Glargine + Insulin Glulisine SSI
25
Outcome Frequency, %
24.3
20
15 P = 0.05 P = 0.10
10
10.3 10.3
8.6
5 P = NS P = 0.24
1.0 1.0 2.9 0.0 2.8 3.8
0
Composite Mortality Wound Pneumonia Acute Renal
Infection Failure
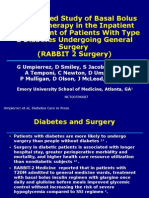
Slide 7. Results of the RABBIT 2-Surgery study. Overall decrease in post-operative complications was associated
with more intensive glucose control using a scheduled basal-bolus-correction insulin strategy. Reprinted
with permission from Umpierrez GE, Smiley D, Jacobs S, et al. Randomized study of basalbolus insulin
therapy in the inpatient management of patients with type 2 diabetes undergoing general surgery
(RABBIT 2 Surgery). Diabetes Care. 2011;34:256 261.25
reported that in postoperative diabetic patients tients (P 0.86). The difference in the rate of hypo-
whose glucose levels were 220 mg/dL, the infection glycemic episodes was not significantly different (33%
rate was 2.7-fold increased (exclusive of urinary vs 25%; P 0.34). Taken together, these studies sug-
tract infections), with the risk for more serious in- gest that tighter glycemic control can be achieved in
fections increased by 5.7-fold. hospitalized patients with scheduled insulin ap-
The only randomized studies in this area come from proaches as opposed to sliding scales but that the types
Umpierrezs group.23 The RABBIT 2 study explored of insulin used may not be crucial.
the glycemic effects of scheduled long-acting and pre- Finally, in RABBIT 2-Surgery (Randomized Study
meal rapid-acting insulin (basal-bolus) versus con- of Basal-Bolus Insulin Therapy in the Inpatient Man-
ventional sliding scales. In 130 insulin-naive patients agement of Patients with Type 2 Diabetes Undergoing
with a mean (SD) blood glucose level of 229 (6) mg/dL, General Surgery),25 the basal-bolus program, again us-
basal-bolus therapy (using the insulin analogues glargine ing glargine and glulisine, was compared to regular
and glulisine) was more effective than was the sliding- insulin sliding scale in 211 patients undergoing general
scale regimen.23 About two thirds of the patients treated surgery. There was an overall mean blood glucose ad-
with glargine-glulisine achieved the blood glucose target vantage of 27 mg/dL in the basal-bolus group. A
(140 mg/dL) versus about one third of patients in the variety of postoperative complications were tracked,
sliding-scale group. More insulin, however, was ulti- including wound infections, pneumonia, respiratory
mately used in the former (40 vs 15 total daily units) The failure, acute renal failure, and bacteremia. The pres-
rate of hypoglycemia (defined as a blood glucose level ence of wound infections was significantly lower with
60 mg/dL) was similar between groups, and no blood basal-bolus (2.9% of patients) than with sliding scale
glucose levels 40 mg/dL were reported. (10.3%) (P 0.05), whereas differences in other compli-
In the DEAN (Insulin Detemir Versus NPH Insulin cations between the 2 groups did not reach statistical
In Hospitalized Patients With Diabetes) study,24 the significance. However, when all of the complications
insulin analogues detemir (basal) and aspart (prandial) were assembled into a composite, a clear advantage to the
were compared with the more conventional human in- more intensive strategy was reported (8.6% vs 24.3% of
sulins, neutral protamine Hagedorn (NPH) and regu- patients) (Slide 7).
lar human insulin. Here, the overall blood glucose tar- The AACE-ADA15,26 inpatient consensus statement
get was achieved in 45% of the analogue-treated also addressed the management of hyperglycemia out-
patients and 48% of the human insulintreated pa- side of the ICU setting (Slide 5). The panel advised
730 Volume 35 Number 5
M. Bogun and S.E. Inzucchi
Management of hyperglycemia in hospitalized patients
Non-ICU Patient with Hyperglycemia
T1DM, insulin-requiring T2DM, or new hyperglycemia T2DM on diet therapy or oral agents
NPO Eating NPO Eating
Basal insulin Basal insulin
May continue oral agents ONLY if no
(home dose or start 0.20.4 4 units/kg /day) (home dose or start 0.20.4 units/kg /day) D/C oral agents
NPH Q12 h or NPH Q12 h or contraindications & well controlled.
Correction insulin for BG>150 mg /dl
Detemir Q1224 h or Detemir Q1224 h or (graded scale of 14 units for each 50 mg /dl, If hyperglycemic or evidence of poor
Glargine Q24 h Glargine Q24 h based on weight & degree of control as outpatient, D/C oral agents
+ + insulin resistance) (sensitizers can be continued) and
Correction insulin for BG>150 mg /dl Bolus (prandial) insulin Begin basal insulin
(graded scale of 14 units for each Regular Q6 h
(home dose or start 0.050.1 units/kg /meal) (start 0.20.4 units/kg /day)
50 mg/dl, based on insulin sensitivity) Lispro, Aspart, Glulisine or
Regular NPH AM & PM (or HS) or
Regular Q6 h Detemir Q1224 h or
+ Glargine Q24 h
Correction insulin for BG>150 mg /dl +
(graded scale of 14 units for each 50 mg /dl, Bolus (prandial) insulin
based on insulin sensitivity) (start 0.050.1 units/kg /day)
Same type as & added to bolus insulin Lispro, Aspart, Glulisine or
Regular
+
Correction insulin for BG>150 mg /dl
(graded scale of 14 units for each
50 mg /dl, based on insulin sensitivity)
Same type as & added to bolus insulin
BLOOD GLUCOSE NOT CONTROLLED (consistently >140 mg /dl fasting, >180 mg /dl random)
Adjust basal insulin by ~1020% Adjust basal insulin by ~1020% Add basal insulin Adjust basal insulin by ~1020%
Q12 days to achieve glucose target Q12 days to achieve glucose target (start 0.20.4 units/kg /day: adjust by Q12 days to achieve BG target
Adjust correction insulin scale by 12 Adjust bolus insulin by 12 units per ~1020% Q12 days to achieve BG target) Adjust bolus insulin by 12 units per
units per dose Q12 days if response dose Q12 days to achieve target NPH Q12 h or dose Q12 days to achieve target
Adjust correction insulin scale by Detemir Q1224 h or Adjust correction insulin scale by
inadequate Glargine Q24 h
12 units per dose if response 12 units per dose if response
Adjust correction insulin scale by
inadequate inadequate
12 units per dose if response
inadequate
Slide 8. Proposed strategy for managing hyperglycemia in non-critically ill hospitalized patients. Adapted with
permission from Inzucchi SE. Clinical practice. Management of hyperglycemia in the hospital setting.
N Engl J Med. 2006;355:19031911.
trying to maintain all glucose levels 180 mg/dL and this risk (renal failure, dehydration, severe heart fail-
premeal glucose 140 mg/dL. The preferred approach ure, acidosis), it would appear best to avoid this
was that employing scheduled basal-nutritional (bo- medication. Thiazolidinediones can be continued if
lus)-correction insulin instead of the still widely used there are no concerns of heart failure, although an
regular insulin sliding scales. At our institution, we en- interruption in therapy of a few days should not
courage the routine use of such a strategy in those patients appreciably alter glucose levels. Incretin-based ther-
who appear to require insulin therapy for 12 days. In apies (DPP-4 inhibitors and GLP-1 receptor ago-
contrast, in short-term patients, the temporary use of cor- nists) are ideally used in patients who are eating
rection insulin only is reasonable, especially if for those because they target mainly postprandial glucose and
with NPO status or if nutritional intake is tenuous. so should probably be avoided when nutritional intake
We tend to avoid the use of oral antihyperglyce- is forbidden or tentative. GLP-1 receptor agonists may
mic agents. Sulfonylureas may lead to hypoglycemia also result in nausea so are best avoided in this setting.
if nutrition is interrupted. There is no inherent rea- Some experts have proposed that, because these drug
son that metformin could not be used, but given its classes are not associated with hypoglycemia and because
risk for lactic acidosis and the frequent complicating their activity appears to be in part related to the degree of
features of hospitalized patients that might increase hyperglycemia, they may have a role in acutely ill pa-
May 2013 731
Clinical Therapeutics
ICU setting has led to improved outcomes in some sin-
Discharge Planning gle-center studies, not all of which were randomized.
Be proactive! Start early (23 days before) Yet other trials have questioned this benefit, and one
What can this patient handle at home? even suggested a mortality risk associated with inten-
Consider side effects, drug intolerances,
sive insulin therapy. A rational synthesis of these data
comorbidities, costs.
Rxs, supplies, appointments
would suggest that good (mid-100 mg/dL range) but
Survival Skills not necessarily stringent (110 mg/dL) glucose control
Outpatient follow-up is key. is the preferred approach in the ICU setting and is most
easily achieved through a validated intravenous insu-
Slide 9. Overview of hospital discharge planning lin-infusion protocol. On medical-surgical wards, a
for patients with diabetes. premeal blood glucose target of 140 mg/dL is reason-
able and achievable in most patients. Physiologic, pro-
active insulin-replacement therapy (ie, the basal-bolus
tients. Adequately powered, randomized clinical trials correction approach) to prevent hyperglycemia is pre-
will be needed. ferred to more conventional, retroactive approaches,
See (Slide 8). for our general approach to managing such as regular insulin sliding scales. Lastly, the dis-
glucose in hospitalized but not non-critically ill diabetic charge planning should always ensure a smooth tran-
patients. sition to outpatient care.
Transitioning to Outpatient Care ACKNOWLEDGMENTS
Discharge planning is an important part of in-hos- Dr. Bogun drafted the manuscript, collected and inter-
pital diabetes management, especially in newly diag- preted the data. Dr. Inzucchi was responsible for the
nosed patients or in those whose antihyperglycemic critical review of the manuscript, collected and inter-
regimen has been altered during the admission. Ideally, preted data and created the slides.
this planning should begin several days before the an-
ticipated discharge and should carefully take into ac-
CONFLICTS OF INTEREST
count whether the patient can successfully implement
Dr. Bogun has no conflicts of interest with regard to the
the prescribed regimen and any accompanying comor-
content of this article. Dr. Inzucchi has served as a
bidities, prevalent contraindications, and anticipated
consultant/advisor to Merck, Boehringer Ingelheim,
side effects. If the diagnosis of diabetes has already
Bristol Myers Squibb, and Novo Nordisk.
been established, the level of control should be assessed
with adjustment of therapy, if necessary. If the disease
was newly identified during the hospitalization, the di- REFERENCES
agnosis should be confirmed. Here, the hospitalization 1. Krinsley JS. Association between hyperglycemia and in-
becomes an opportunity to educate and implement an creased hospital mortality in a heterogeneous population
initial therapeutic plan. Finally, if stress hyperglycemia of critically ill patients. Mayo Clin Proc. 2003;782:1471
resolves in-hospital or soon after discharge, then no 1478.
further action would be required other than routine 2. Kosiborod M, Inzucchi SE, Krumholz HM, et al. Glucomet-
follow-up. Good communication with the patients rics in patients hospitalized with acute myocardial infarc-
primary care clinician or endocrinologist is key to en- tion: defining the optimal outcomes-based measure of risk.
sure a smooth transition postdischarge (Slide 9). Circulation. 2008;117:1018 1027.
3. Umpierrez GE, Isaacs SD, Bazargan N, et al. Hyperglyce-
mia: an independent marker of in-hospital mortality in
CONCLUSIONS
patients with undiagnosed diabetes. J Clin Endocrinol Metab.
Hyperglycemia occurs frequently in the hospital, both 2002;87:978 982.
in patients with and without diabetes; its implications 4. Kosiborod M. Blood glucose and its prognostic implica-
may be more serious in the former. Inpatient hypergly- tions in patients hospitalised with acute myocardial infarc-
cemia is a predictor of adverse outcomes including tion. Diab Vasc Dis Res. 2008;5:269 275.
mortality and is associated with increased length of 5. Furnary AP, Wu Y, Bookin SO. Effect of hyperglycemia and
stay and costs. Intensive glucose management in the continuous intravenous insulin infusions on outcomes of
732 Volume 35 Number 5
M. Bogun and S.E. Inzucchi
cardiac surgical procedures: the Port- 14. Kosiborod M, Inzucchi SE, Goyal A, 21. Baker EH, Janaway CH, Philips BJ, et
land Diabetic Project. Endocr Pract. et al. Relationship between sponta- al. Hyperglycaemia is associated
2004;10 Suppl 2:2133. neous and iatrogenic hypoglycemia with poor outcomes in patients ad-
6. Malmberg K, for the DIGAMI (Diabe- and mortality in patients hospital- mitted to hospital with acute exacer-
tes Mellitus, Insulin Glucose Infu- ized with acute myocardial infarc- bations of chronic obstructive pul-
sion in Acute Myocardial Infarction) tion. JAMA. 2009;3015:1556 1564. monary disease. Thorax. 2006;61:
Study Group. Prospective ran- 15. Moghissi ES, Korytkowski MT, Di- 284 289.
domised study of intensive insulin Nardo M, et al. American Associa- 22. Pomposelli JJ, Baxter JK 3rd, Babi-
treatment on long term survival after tion of Clinical Endocrinologists and
neau TJ, et al. Early postoperative
acute myocardial infarction in pa- American Diabetes Association con-
glucose control predicts nosoco-
tients with diabetes mellitus. BMJ. sensus statement on inpatient glyce-
mial infection rate in diabetic pa-
1997;314:15121515. mic control. Diabetes Care. 2009;32:
tients. JPEN J Parenter Enteral Nutr.
7. Cheung NW, Wong VW, McLean M. 1119 1131.
1998;22:77 81.
16. Wilson M, Weinreb J, Hoo GW.
The Hyperglycemia: Intensive Insulin 23. Umpierrez GE, Smiley D, Zisman A,
Intensive insulin therapy in critical
Infusion in Infarction (HI-5) study: a et al. Randomized study of basal-
care: a review of 12 protocols. Diabe-
randomized controlled trial of insulin bolus insulin therapy in the inpa-
tes Care. 2007;30:10051011.
infusion therapy for myocardial infarc- tient management of patients with
17. Shetty S, Inzucchi SE, Goldberg PA,
tion. Diabetes Care. 2006;29:765770. type 2 diabetes (RABBIT 2 Trial).
et al. Adapting to the new consensus
8. Malmberg K, Ryden L, Wedel H, et Diabetes Care. 2007;30:21812186.
guidelines for managing hyperglyce-
al. Intense metabolic control by
mia during critical illness: the up- 24. Umpierrez GE, Hor T, Smiley D, et
means of insulin in patients with
dated Yale insulin infusion protocol. al. Comparison of inpatient insulin
diabetes mellitus and acute myocar- Endocr Pract. 2012;18:363370. regimens with detemir plus aspart
dial infarction (DIGAMI 2): effects 18. Arabi YM, Dabbagh OC, Tamim versus neutral protamine Hagedorn
on mortality and morbidity. Eur HM, et al. Intensive versus conven- plus regular in medical patients with
Heart J. 2005;26:650 661. tional insulin therapy: a randomized type 2 diabetes. J Clin Endocrinol
9. Mehta SR, Yusuf S, Diaz R, et al. controlled trial in medical and surgi- Metab. 2009;94:564 569.
Effect of glucose-insulin-potassium cal critically ill patients. Crit Care
25. Umpierrez GE, Smiley D, Jacobs S, et
infusion on mortality in patients Med. 2008;362:3190 3197.
al. Randomized study of basal-
with acute ST-segment elevation 19. Preiser JC, Devos P, Ruiz-Santana S,
bolus insulin therapy in the inpa-
myocardial infarction: the CREATE- et al. A prospective randomised
tient management of patients with
ECLA randomized controlled trial. multi-centre controlled trial on tight
JAMA. 2005;293:437 446. type 2 diabetes undergoing general
glucose control by intensive insulin
10. van den Berghe G, Wouters P, Week- surgery (RABBIT 2 Surgery). Diabetes
therapy in adult intensive care units:
ers F, et al. Intensive insulin therapy the Glucontrol Study. Intensive Care Care. 2011;34:256 261.
in critically ill patients. N Engl J Med. Med. 2009;35:1738 1748. 26. Moghissi ES, Korytkowski MT, Di-
2001;3459:1359 1367. 20. De La Rosa Gdel C, Donado JH, Nardo M, et al. American Associa-
11. van den Berghe G, Wilmer A, Her- Restrepo AH, et al. Strict glycaemic tion of Clinical Endocrinologists and
mans G, et al. Intensive insulin control in patients hospitalised in a American Diabetes Association con-
therapy in the medical ICU. N Engl mixed medical and surgical intensive sensus statement on inpatient glyce-
J Med. 2006;354:449 461. care unit: a randomised clinical trial. mic control. Endocr Pract. 2009;15:
12. Finfer S, Chittock DR, Su SY, et al, Crit Care. 2008;12:R120. 353369.
for the NICE-SUGAR Study Investi-
gators. Intensive versus conventional
glucose control in critically ill pa-
tients. N Engl J Med. 2009;3603:
12831297.
13. Griesdale DE, de Souza RJ, van Dam
RM, et al. Intensive insulin therapy
and mortality among critically ill
patients: a meta-analysis including Address correspondence to: Silvio Inzucchi, MD, Section of Endocrinology,
NICE-SUGAR study data. CMAJ. Yale Diabetes Center, Yale University School of Medicine, PO Box 208020,
2009;180:821 827. 333 Cedar Street, New Haven, CT 06520-8056. E-mail: xxxx
May 2013 733
Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Abasaglar Patient Information Leaflet Updated Dec 17Dokument2 SeitenAbasaglar Patient Information Leaflet Updated Dec 17zafemarakiNoch keine Bewertungen
- Practical Guide To Inpatient Glycaemic Care - V2 2020Dokument115 SeitenPractical Guide To Inpatient Glycaemic Care - V2 2020shahirahNoch keine Bewertungen
- A GDM ProformaDokument3 SeitenA GDM Proformarasnamj009Noch keine Bewertungen
- 1237-Article Text-4113-4-10-20220716Dokument5 Seiten1237-Article Text-4113-4-10-20220716Delvi BudimanNoch keine Bewertungen
- 162 319 1 SMDokument8 Seiten162 319 1 SMAsniar RNoch keine Bewertungen
- Penerapan Asuhan Keperawatan Pada Pasien Ny. N Dengan DM Tipe Ii Dalam Pemenuhan Kebutuhan Nutrisi Di Rsud Labuang Baji MakassarDokument19 SeitenPenerapan Asuhan Keperawatan Pada Pasien Ny. N Dengan DM Tipe Ii Dalam Pemenuhan Kebutuhan Nutrisi Di Rsud Labuang Baji MakassarHerman HermanNoch keine Bewertungen
- Endocrine - Insulin Management PDFDokument1 SeiteEndocrine - Insulin Management PDFPshtiwan MahmoodNoch keine Bewertungen
- Lecture No:10 Diabetes Mellitus: - at The End of This Lecture, Student Will Be Able To ExplainDokument33 SeitenLecture No:10 Diabetes Mellitus: - at The End of This Lecture, Student Will Be Able To ExplainAntoNoch keine Bewertungen
- RABBIT-2 Surgery - (12 - 2010)Dokument32 SeitenRABBIT-2 Surgery - (12 - 2010)aromerozNoch keine Bewertungen
- Glucose Tolerance Test ResultsDokument1 SeiteGlucose Tolerance Test ResultsZeeshan KhanNoch keine Bewertungen
- Blood Glucose Monitoring ChartDokument3 SeitenBlood Glucose Monitoring Chartfazal_f1Noch keine Bewertungen
- Pharmacotherapy in Diabetes MellitusDokument23 SeitenPharmacotherapy in Diabetes MellitussalinaNoch keine Bewertungen
- Winter Gerst 2006Dokument9 SeitenWinter Gerst 2006Dr XNoch keine Bewertungen
- Self-Monitoring of Blood Glucose in Type 2 Diabetes Recent StudiesDokument11 SeitenSelf-Monitoring of Blood Glucose in Type 2 Diabetes Recent StudiesSelaNoch keine Bewertungen
- Insulin TherapyDokument76 SeitenInsulin TherapyDk YadavNoch keine Bewertungen
- Accu-Chek 360 View ToolDokument2 SeitenAccu-Chek 360 View Toolsayang12155100% (1)
- Eye Exam Rates Among Chilean DiabeticsDokument9 SeitenEye Exam Rates Among Chilean DiabeticsUlises GilNoch keine Bewertungen
- Treatment Based On: Pathophysiology of HyperglycemiaDokument38 SeitenTreatment Based On: Pathophysiology of HyperglycemiaRoby KieranNoch keine Bewertungen
- Insulinoma in A Patient With Type 2 Diabetes: Case Report Nama: Iqbal Putra Amirullah NIM: 030.14.098Dokument11 SeitenInsulinoma in A Patient With Type 2 Diabetes: Case Report Nama: Iqbal Putra Amirullah NIM: 030.14.098desmawitaNoch keine Bewertungen
- Managing Gestational Diabetes and MacrosomiaDokument30 SeitenManaging Gestational Diabetes and MacrosomiaCharlz ZipaganNoch keine Bewertungen
- ADS ADEA ANZCA NZSSD - DKA - SGLT2i - Alert - Ver July 2022Dokument3 SeitenADS ADEA ANZCA NZSSD - DKA - SGLT2i - Alert - Ver July 2022tom.condon.02Noch keine Bewertungen
- Clinical Practice Guidelines PDFDokument315 SeitenClinical Practice Guidelines PDFDian Sulistya EkaputriNoch keine Bewertungen
- Diabetes MelitusDokument44 SeitenDiabetes MelitusDwi Novianti SugihartiNoch keine Bewertungen
- Neonatal Hypoglycemia (Infant of Diabetic Mother)Dokument15 SeitenNeonatal Hypoglycemia (Infant of Diabetic Mother)diana rossNoch keine Bewertungen
- Plasma Glucose, Insulin, and DMDokument4 SeitenPlasma Glucose, Insulin, and DMVina Zavira NizarNoch keine Bewertungen
- Aga Khan Medical Centre Fasting Glucose Test ReportDokument1 SeiteAga Khan Medical Centre Fasting Glucose Test ReportTâÿÿàbá ĮkrâmNoch keine Bewertungen
- 306 1164 1 PB PDFDokument6 Seiten306 1164 1 PB PDFDini RizkyNoch keine Bewertungen
- Ketosis-Prone Diabetes (Flatbush Diabetes)Dokument8 SeitenKetosis-Prone Diabetes (Flatbush Diabetes)davideNoch keine Bewertungen
- Basal Insulin Versus Premixed Insulin For The Treatment of T2DmDokument98 SeitenBasal Insulin Versus Premixed Insulin For The Treatment of T2DmMaya SwariNoch keine Bewertungen
- Bomba MedtronicDokument40 SeitenBomba MedtronicrafaelplNoch keine Bewertungen