Das könnte Ihnen auch gefallen
- Neurology Equations Made Simple: Differential Diagnosis and NeuroemergenciesVon EverandNeurology Equations Made Simple: Differential Diagnosis and NeuroemergenciesNoch keine Bewertungen
- Human diseases Research and textbook: 1Von EverandHuman diseases Research and textbook: 1Noch keine Bewertungen
- Congenital Scoliosis Causes and TreatmentsDokument24 SeitenCongenital Scoliosis Causes and TreatmentsirfanzukriNoch keine Bewertungen
- Fetal CaseDokument43 SeitenFetal Casemomina zulfeenNoch keine Bewertungen
- Paediatric OrthopaedicsDokument80 SeitenPaediatric OrthopaedicsShimmering MoonNoch keine Bewertungen
- Adolescent Idiopathic Scoliosis TreatmentDokument17 SeitenAdolescent Idiopathic Scoliosis TreatmentNam LeeNoch keine Bewertungen
- Ortho Zusammenfassung 2020Dokument258 SeitenOrtho Zusammenfassung 2020Aastha SethNoch keine Bewertungen
- Turners Syndrome: Sonika Shimon Prasad S160232Dokument20 SeitenTurners Syndrome: Sonika Shimon Prasad S160232Ivy DanNoch keine Bewertungen
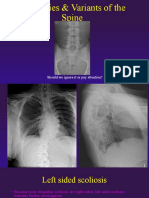
- Anomalies Variants of The SpineDokument41 SeitenAnomalies Variants of The SpinekinexNoch keine Bewertungen
- Scoliosis: An OverviewDokument99 SeitenScoliosis: An Overviewmarjan dronjakNoch keine Bewertungen
- Developmental Hip Dysplasia: Viorel RaducanDokument4 SeitenDevelopmental Hip Dysplasia: Viorel RaducanIvan Roy Fernandez BautistaNoch keine Bewertungen
- Pathologies of The HipDokument57 SeitenPathologies of The HipFreeburn SimunchembuNoch keine Bewertungen
- Transient Hip SynovitisDokument43 SeitenTransient Hip SynovitisnurulNoch keine Bewertungen
- Turner Syndrome, Klinefelter Syndrome, Down SyndromeDokument78 SeitenTurner Syndrome, Klinefelter Syndrome, Down SyndromeTasya100% (3)
- Congenital Brain Anomalies: Dr. Dev LakheraDokument61 SeitenCongenital Brain Anomalies: Dr. Dev LakheraNinaNoch keine Bewertungen
- Approach To AtaxiaDokument6 SeitenApproach To AtaxiaVivek KumarNoch keine Bewertungen
- Genetic Disorders, Skeletal Dysplasias, and Malformations: Appley's Reading Achmad Fachroni, DRDokument38 SeitenGenetic Disorders, Skeletal Dysplasias, and Malformations: Appley's Reading Achmad Fachroni, DRAchmad FachroniNoch keine Bewertungen
- The Approach To Dysmorphic ChildDokument14 SeitenThe Approach To Dysmorphic ChildBelinderjit KaurNoch keine Bewertungen
- Deteksi Dini Kelainan Pada JaninDokument108 SeitenDeteksi Dini Kelainan Pada JaninYuyunNoch keine Bewertungen
- Naskah PublikasiDokument76 SeitenNaskah PublikasiAnonymous B5bm6wL1UwNoch keine Bewertungen
- Developmental Anomalies: Dr. Mark Louie M. LantingDokument64 SeitenDevelopmental Anomalies: Dr. Mark Louie M. Lantinglouie10279098Noch keine Bewertungen
- SurgeryspecimensDokument81 SeitenSurgeryspecimensHimanshu BadjatyaNoch keine Bewertungen
- AchondroplasiaDokument25 SeitenAchondroplasiaAkashGhoshNoch keine Bewertungen
- Legg Calve PerthesDokument93 SeitenLegg Calve PerthesAkshay LakraNoch keine Bewertungen
- Radiographic Diagnosis For Canine Hip Dysplasia: 18 August 2021Dokument85 SeitenRadiographic Diagnosis For Canine Hip Dysplasia: 18 August 2021Thirada sosawangNoch keine Bewertungen
- Genetic disorders of the skeletonDokument51 SeitenGenetic disorders of the skeletonElisabeth Permatasari SidabutarNoch keine Bewertungen
- ISMT12 - Day 230 - Ravanno - Disorder of The Skull and Vertebral ColumnDokument34 SeitenISMT12 - Day 230 - Ravanno - Disorder of The Skull and Vertebral ColumnRavanno Fanizza HarahapNoch keine Bewertungen
- Scfe PDFDokument39 SeitenScfe PDFMuhammad Tabish SaleemNoch keine Bewertungen
- Surgical Management of Cerebral PalsyDokument72 SeitenSurgical Management of Cerebral PalsySamNoch keine Bewertungen
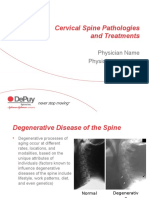
- Cervical Pathologies TreatmentsDokument27 SeitenCervical Pathologies TreatmentssepthyaniNoch keine Bewertungen
- Acute Aortic Syndromes: Diagnosis and Imaging TechniquesDokument17 SeitenAcute Aortic Syndromes: Diagnosis and Imaging TechniquesHARBENNoch keine Bewertungen
- MSK Congenital DisordersDokument49 SeitenMSK Congenital DisordersFarah Balqis BaragbahNoch keine Bewertungen
- DDHDokument174 SeitenDDHVikas RaiNoch keine Bewertungen
- CraniosynostosisDokument54 SeitenCraniosynostosistameemNoch keine Bewertungen
- Common Paediatric Genetic Disorders - CUHK - Paed - 2018Dokument21 SeitenCommon Paediatric Genetic Disorders - CUHK - Paed - 2018B AuNoch keine Bewertungen
- 2 Af 5 VERTIGODokument35 Seiten2 Af 5 VERTIGOmuneceNoch keine Bewertungen
- Alteration in Number: Autosomal DisordersDokument6 SeitenAlteration in Number: Autosomal DisordersnkivcNoch keine Bewertungen
- Developmental Hip Dysplasia Diagnosis and TreatmentDokument12 SeitenDevelopmental Hip Dysplasia Diagnosis and TreatmentFifi Chi Keluarga PrajaNoch keine Bewertungen
- Spina Bifida: by DR - Zakir Uk DPT, MSPT MSK (Kmu)Dokument19 SeitenSpina Bifida: by DR - Zakir Uk DPT, MSPT MSK (Kmu)syge zwvuNoch keine Bewertungen
- Anesthetic Considerations for Pediatric Scoliosis RepairDokument34 SeitenAnesthetic Considerations for Pediatric Scoliosis RepairMorad SatariNoch keine Bewertungen
- Understanding Kyphosis and its ClassificationDokument36 SeitenUnderstanding Kyphosis and its ClassificationSoare Elena-CosminaNoch keine Bewertungen
- SurgeryspecimensDokument81 SeitenSurgeryspecimensHimanshu BadjatyaNoch keine Bewertungen
- Cervical SpineDokument51 SeitenCervical SpineEvandiar IzwardyNoch keine Bewertungen
- Cerebral Palsy: MBBS YEAR 3, Batch 8, 2019 DR - Swe Zin Aye Zinaye - Swe@qiup - Edu.myDokument37 SeitenCerebral Palsy: MBBS YEAR 3, Batch 8, 2019 DR - Swe Zin Aye Zinaye - Swe@qiup - Edu.myVishalli KalaiwananNoch keine Bewertungen
- Whiplash and Spine Injuries GuideDokument58 SeitenWhiplash and Spine Injuries GuidetoobaNoch keine Bewertungen
- 25 Congenital DR Fazl Karam)Dokument45 Seiten25 Congenital DR Fazl Karam)Himanshu NarangNoch keine Bewertungen
- Balance Disorders and Vestibular Function Testing - 230602 - 081139Dokument55 SeitenBalance Disorders and Vestibular Function Testing - 230602 - 081139diana mistraNoch keine Bewertungen
- Trisomy 21-Down Syndrome: Payal DhakappaDokument35 SeitenTrisomy 21-Down Syndrome: Payal DhakappaPayal AmarnathNoch keine Bewertungen
- 0127「小兒遺傳及代謝」講師陳燕彰醫師Dokument114 Seiten0127「小兒遺傳及代謝」講師陳燕彰醫師許懷朔Noch keine Bewertungen
- Radio-Ulnar SynostosisDokument16 SeitenRadio-Ulnar SynostosisVenkatanarasimhan BNoch keine Bewertungen
- MRI 2011 Presentation ScoliosisDokument9 SeitenMRI 2011 Presentation ScoliosisElizabeth-Anne AddisonNoch keine Bewertungen
- DR - Rieva Kuliah 7 November - 2018Dokument38 SeitenDR - Rieva Kuliah 7 November - 2018Nisrina100% (1)
- Edwards Syndrome: Presented by Amrutha Ramakrishnan NairDokument37 SeitenEdwards Syndrome: Presented by Amrutha Ramakrishnan Nairअंकित सिंह सिंधड़Noch keine Bewertungen
- Birth InjuriesDokument30 SeitenBirth InjuriesMarini Rachma GhaisaniNoch keine Bewertungen
- DO FinalDokument38 SeitenDO FinalAminah KhanNoch keine Bewertungen
- Birth TraumaDokument57 SeitenBirth TraumaAbu HajerahNoch keine Bewertungen
- Ataxic Disorder: Presenter Krishna Ghimire InternDokument29 SeitenAtaxic Disorder: Presenter Krishna Ghimire InternPrag GK SubediNoch keine Bewertungen
- NEUROBLASTOMA Treatment and PrognosisDokument49 SeitenNEUROBLASTOMA Treatment and PrognosisEretare OdjugoNoch keine Bewertungen
- Anorectal Malformation Diagnosis and TreatmentDokument10 SeitenAnorectal Malformation Diagnosis and TreatmentUtari RahardjoNoch keine Bewertungen
- Birth Trauma IN Newborns: DR Vanessa Lee Wan Mun Paediatrician Hospital Melaka 23 OCTOBER 2018Dokument28 SeitenBirth Trauma IN Newborns: DR Vanessa Lee Wan Mun Paediatrician Hospital Melaka 23 OCTOBER 2018Cupin DeNoch keine Bewertungen
- Tag Ug/U Seicoleg Rhwydwaith Athrawon Medi 2018Dokument3 SeitenTag Ug/U Seicoleg Rhwydwaith Athrawon Medi 2018Virtues GracesNoch keine Bewertungen
- Layers of The Plantar FootDokument2 SeitenLayers of The Plantar FootVirtues GracesNoch keine Bewertungen
- 2018 Cultural PavilionDokument5 Seiten2018 Cultural PavilionVirtues GracesNoch keine Bewertungen
- Gems Oct 2017 Menu BDokument4 SeitenGems Oct 2017 Menu BVirtues GracesNoch keine Bewertungen
- Necrotizing Fasciitis: Early Biopsy Key for Aggressive TreatmentDokument6 SeitenNecrotizing Fasciitis: Early Biopsy Key for Aggressive TreatmentVirtues GracesNoch keine Bewertungen
- How Church Becomes CatholicDokument16 SeitenHow Church Becomes CatholicVirtues GracesNoch keine Bewertungen
- Faithfulness LyricsDokument6 SeitenFaithfulness LyricsVirtues GracesNoch keine Bewertungen
- Weddiing LyricsDokument8 SeitenWeddiing LyricsVirtues GracesNoch keine Bewertungen
- Kienbock's DiseaseDokument12 SeitenKienbock's DiseaseVirtues GracesNoch keine Bewertungen
- W Hat Can We Do?: What Specific Partners Can Bring To The T AbleDokument1 SeiteW Hat Can We Do?: What Specific Partners Can Bring To The T AbleVirtues GracesNoch keine Bewertungen
- God Has The Final WordDokument3 SeitenGod Has The Final WordVirtues GracesNoch keine Bewertungen
- Olecranon FracturesDokument5 SeitenOlecranon FracturesVirtues GracesNoch keine Bewertungen
- Jersey FingerDokument4 SeitenJersey FingerVirtues GracesNoch keine Bewertungen
- Mercy Forgives.Dokument1 SeiteMercy Forgives.Virtues GracesNoch keine Bewertungen
- Life With Jesus... : ... The High's The Lows and The RideDokument1 SeiteLife With Jesus... : ... The High's The Lows and The RideVirtues GracesNoch keine Bewertungen
- Tscherne Classification PDFDokument1 SeiteTscherne Classification PDFVirtues GracesNoch keine Bewertungen
- Resource Contemplation Action Ringma PDFDokument10 SeitenResource Contemplation Action Ringma PDFVirtues GracesNoch keine Bewertungen
- Accomplishment Report 2021-2022Dokument45 SeitenAccomplishment Report 2021-2022Emmanuel Ivan GarganeraNoch keine Bewertungen
- HenyaDokument6 SeitenHenyaKunnithi Sameunjai100% (1)
- CAS-GEC04 Module11 Food-SecurityDokument6 SeitenCAS-GEC04 Module11 Food-SecurityPermalino Borja Rose AnneNoch keine Bewertungen
- Attributes and DialogsDokument29 SeitenAttributes and DialogsErdenegombo MunkhbaatarNoch keine Bewertungen
- Theory of Linear Programming: Standard Form and HistoryDokument42 SeitenTheory of Linear Programming: Standard Form and HistoryJayakumarNoch keine Bewertungen
- Cold Rolled Steel Sections - Specification: Kenya StandardDokument21 SeitenCold Rolled Steel Sections - Specification: Kenya StandardPEng. Tech. Alvince KoreroNoch keine Bewertungen
- SEO-Optimized Title for Python Code Output QuestionsDokument2 SeitenSEO-Optimized Title for Python Code Output QuestionsTaru GoelNoch keine Bewertungen
- Additional Help With OSCOLA Style GuidelinesDokument26 SeitenAdditional Help With OSCOLA Style GuidelinesThabooNoch keine Bewertungen
- Archlinux 之 之 之 之 Lmap 攻 略 ( 攻 略 ( 攻 略 ( 攻 略 ( 1 、 环 境 准 备 ) 、 环 境 准 备 ) 、 环 境 准 备 ) 、 环 境 准 备 )Dokument16 SeitenArchlinux 之 之 之 之 Lmap 攻 略 ( 攻 略 ( 攻 略 ( 攻 略 ( 1 、 环 境 准 备 ) 、 环 境 准 备 ) 、 环 境 准 备 ) 、 环 境 准 备 )Goh Ka WeeNoch keine Bewertungen
- DELcraFT Works CleanEra ProjectDokument31 SeitenDELcraFT Works CleanEra Projectenrico_britaiNoch keine Bewertungen
- Annamalai International Journal of Business Studies and Research AijbsrDokument2 SeitenAnnamalai International Journal of Business Studies and Research AijbsrNisha NishaNoch keine Bewertungen
- Analytical Approach To Estimate Feeder AccommodatiDokument16 SeitenAnalytical Approach To Estimate Feeder AccommodatiCleberton ReizNoch keine Bewertungen
- Onan Service Manual MDJA MDJB MDJC MDJE MDJF Marine Diesel Genset Engines 974-0750Dokument92 SeitenOnan Service Manual MDJA MDJB MDJC MDJE MDJF Marine Diesel Genset Engines 974-0750GreenMountainGenerators80% (10)
- DC Motor Dynamics Data Acquisition, Parameters Estimation and Implementation of Cascade ControlDokument5 SeitenDC Motor Dynamics Data Acquisition, Parameters Estimation and Implementation of Cascade ControlAlisson Magalhães Silva MagalhãesNoch keine Bewertungen
- Axe Case Study - Call Me NowDokument6 SeitenAxe Case Study - Call Me NowvirgoashishNoch keine Bewertungen
- House Rules For Jforce: Penalties (First Offence/Minor Offense) Penalties (First Offence/Major Offence)Dokument4 SeitenHouse Rules For Jforce: Penalties (First Offence/Minor Offense) Penalties (First Offence/Major Offence)Raphael Eyitayor TyNoch keine Bewertungen
- Difference Between Mark Up and MarginDokument2 SeitenDifference Between Mark Up and MarginIan VinoyaNoch keine Bewertungen
- Radio Frequency Transmitter Type 1: System OperationDokument2 SeitenRadio Frequency Transmitter Type 1: System OperationAnonymous qjoKrp0oNoch keine Bewertungen
- Chapter 3 of David CrystalDokument3 SeitenChapter 3 of David CrystalKritika RamchurnNoch keine Bewertungen
- ERP Complete Cycle of ERP From Order To DispatchDokument316 SeitenERP Complete Cycle of ERP From Order To DispatchgynxNoch keine Bewertungen
- Modified Syllabus of Control SystemDokument2 SeitenModified Syllabus of Control SystemDigambar PatilNoch keine Bewertungen
- Yellowstone Food WebDokument4 SeitenYellowstone Food WebAmsyidi AsmidaNoch keine Bewertungen
- Unit 1 TQM NotesDokument26 SeitenUnit 1 TQM NotesHarishNoch keine Bewertungen
- India Today 11-02-2019 PDFDokument85 SeitenIndia Today 11-02-2019 PDFGNoch keine Bewertungen
- 2nd Pornhub Awards - WikipediaaDokument13 Seiten2nd Pornhub Awards - WikipediaaParam SinghNoch keine Bewertungen
- Striedter - 2015 - Evolution of The Hippocampus in Reptiles and BirdsDokument22 SeitenStriedter - 2015 - Evolution of The Hippocampus in Reptiles and BirdsOsny SillasNoch keine Bewertungen
- Why Genentech Is 1Dokument7 SeitenWhy Genentech Is 1panmongolsNoch keine Bewertungen
- Maverick Brochure SMLDokument16 SeitenMaverick Brochure SMLmalaoui44Noch keine Bewertungen
- Google Dorks For PentestingDokument11 SeitenGoogle Dorks For PentestingClara Elizabeth Ochoa VicenteNoch keine Bewertungen
- BPL Millipacs 2mm Hardmetrics RarDokument3 SeitenBPL Millipacs 2mm Hardmetrics RarGunter BragaNoch keine Bewertungen