Das könnte Ihnen auch gefallen
- 6th Central Pay Commission Salary CalculatorDokument15 Seiten6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Universal Free Reiki PDFDokument4 SeitenUniversal Free Reiki PDFSabiduria Pura100% (1)
- Add Maths Sba 1Dokument17 SeitenAdd Maths Sba 1annmarie0% (4)
- Next To Normal - Abridged ScriptDokument13 SeitenNext To Normal - Abridged Scriptterrify007Noch keine Bewertungen
- Discharge PlanDokument4 SeitenDischarge PlanJennyLapitanNoch keine Bewertungen
- Why Effective Communication Is Important in The Operating RoomDokument1 SeiteWhy Effective Communication Is Important in The Operating RoomMinhwa KimNoch keine Bewertungen
- Chapter 15 - Health and Physical Assessment of The Adult ClientDokument65 SeitenChapter 15 - Health and Physical Assessment of The Adult ClientKristian Jane de Jesus100% (1)
- OB-GYN - MCQ - 2012 - 5th-Year - Mu - TahDokument16 SeitenOB-GYN - MCQ - 2012 - 5th-Year - Mu - TahHalah100% (1)
- Arcipe Iccu Case 5Dokument98 SeitenArcipe Iccu Case 5Maria Charis Anne Indanan100% (1)
- Teaching Plan For HypertensionDokument5 SeitenTeaching Plan For HypertensionMaureen Mae Binohlan100% (1)
- AO 2009 0025 Essential Newborn CareDokument15 SeitenAO 2009 0025 Essential Newborn Carejulesubayubay542895% (21)
- Drug StudyDokument12 SeitenDrug StudyFiela De VillaNoch keine Bewertungen
- Challenges For Nursing Students in The Clinical Learning EnvironmDokument117 SeitenChallenges For Nursing Students in The Clinical Learning EnvironmCarla Jane Mirasol Apolinario100% (2)
- History and Physical ExaminationDokument18 SeitenHistory and Physical ExaminationadesamboraNoch keine Bewertungen
- Nursing and Patient Safety in The Operating RoomDokument10 SeitenNursing and Patient Safety in The Operating RoomJoe AbelloNoch keine Bewertungen
- Xavier University - Ateneo de Cagayan College of Nursing S.Y. 2020-2021Dokument4 SeitenXavier University - Ateneo de Cagayan College of Nursing S.Y. 2020-2021Dudil GoatNoch keine Bewertungen
- History and Physical ExaminationDokument17 SeitenHistory and Physical ExaminationNur Fatima SanaaniNoch keine Bewertungen
- Xavier University - Ateneo de Cagayan College of Nursing S.Y. 2020-2021Dokument5 SeitenXavier University - Ateneo de Cagayan College of Nursing S.Y. 2020-2021Dudil GoatNoch keine Bewertungen
- Medical Ethics More Than Hundred CasesDokument33 SeitenMedical Ethics More Than Hundred Caseskrebkreb100% (4)
- Mindray BS-120 / BS-200 / BS-300 / BS-380 / BS-400: MTD Diagnostics, SRLDokument40 SeitenMindray BS-120 / BS-200 / BS-300 / BS-380 / BS-400: MTD Diagnostics, SRLCarlos SoutoNoch keine Bewertungen
- BSN III 2 Group 3 FinalDokument55 SeitenBSN III 2 Group 3 FinalCharinaNoch keine Bewertungen
- Nursing Law R.A. 9173Dokument13 SeitenNursing Law R.A. 9173JenniiLyn Deeo ÜNoch keine Bewertungen
- Clinical Mycology 2nd Ed (PDF) (Tahir99) VRGDokument674 SeitenClinical Mycology 2nd Ed (PDF) (Tahir99) VRGbiliboiNoch keine Bewertungen
- 200 Bed Hospital Project ReportDokument59 Seiten200 Bed Hospital Project ReporttonyNoch keine Bewertungen
- Paul Krebaum Skunk Odor Removal RecipeDokument2 SeitenPaul Krebaum Skunk Odor Removal Recipeozzaib100% (1)
- Cefoxitin and Ketorolac Edited!!Dokument3 SeitenCefoxitin and Ketorolac Edited!!Bryan Cruz VisarraNoch keine Bewertungen
- Course in The Ward Date, Doctor'S Order AnalysisDokument8 SeitenCourse in The Ward Date, Doctor'S Order AnalysisbillyktoubattsNoch keine Bewertungen
- Drug StudyDokument23 SeitenDrug StudyampalNoch keine Bewertungen
- Unang Yakap FlyerDokument2 SeitenUnang Yakap FlyerKeith Giomeer Petrola83% (6)
- Drug Study: Davao Doctors College General Malvar ST., Davao City Nursing ProgramDokument3 SeitenDrug Study: Davao Doctors College General Malvar ST., Davao City Nursing ProgramJear RomeroNoch keine Bewertungen
- Journal ReadingDokument2 SeitenJournal ReadingMark Ianne AngNoch keine Bewertungen
- Discharge Planning PaperDokument5 SeitenDischarge Planning Paperapi-283173905Noch keine Bewertungen
- Geriatric For JustineDokument28 SeitenGeriatric For JustineJaylord VerazonNoch keine Bewertungen
- Kardex, Drug Study and CheckDokument12 SeitenKardex, Drug Study and CheckJemina Rafanan RacadioNoch keine Bewertungen
- Job Application Letter For NurseDokument2 SeitenJob Application Letter For Nursenur aisyahNoch keine Bewertungen
- VentolinDokument4 SeitenVentolinArlan AbraganNoch keine Bewertungen
- Cesarean Delivery: A Reading OnDokument4 SeitenCesarean Delivery: A Reading OnAnge MinguitoNoch keine Bewertungen
- LevofloxacinDokument2 SeitenLevofloxacinKatie McPeek100% (3)
- DRUGSTUDY RANITIDINE, METRONIDAZOLE, CEFUROXIME, KEtorolac NUBainDokument7 SeitenDRUGSTUDY RANITIDINE, METRONIDAZOLE, CEFUROXIME, KEtorolac NUBainKyle Cholo CholoNoch keine Bewertungen
- Weekly Requirement OB WardDokument12 SeitenWeekly Requirement OB WardXerxes DejitoNoch keine Bewertungen
- Drug StudyDokument9 SeitenDrug StudyShane Arroyo100% (1)
- Benicar Drug StudyDokument2 SeitenBenicar Drug StudyCheezy BreadNoch keine Bewertungen
- Drug StudyDokument2 SeitenDrug StudyemmanuelmyagokayeNoch keine Bewertungen
- NCLFNP - Mr. Robert McClelland CaseDokument4 SeitenNCLFNP - Mr. Robert McClelland CaseAiresh Lamao50% (2)
- What Is TAHbsoDokument2 SeitenWhat Is TAHbsomiskidd100% (2)
- Emergency Room Nursing Care Plan: Saint Louis University Baguio City School of Nursing S.Y. 2019-2020Dokument5 SeitenEmergency Room Nursing Care Plan: Saint Louis University Baguio City School of Nursing S.Y. 2019-2020Wyen CabatbatNoch keine Bewertungen
- GAT NCP Surgery WardDokument4 SeitenGAT NCP Surgery WardDon Richard0% (1)
- Surgical Ward JournalDokument6 SeitenSurgical Ward JournalMa Genille Samporna SabalNoch keine Bewertungen
- NURSING CARE PLAN FOR CROHN'sDokument2 SeitenNURSING CARE PLAN FOR CROHN'sMuhyeeSalaIdjadNoch keine Bewertungen
- Lived Experiences of Nurses On Nursing Shortage: Basis in Strengthening Nurses' Protection Advocacies and EducationDokument20 SeitenLived Experiences of Nurses On Nursing Shortage: Basis in Strengthening Nurses' Protection Advocacies and EducationPsychology and Education: A Multidisciplinary JournalNoch keine Bewertungen
- Drug StudyDokument4 SeitenDrug StudyHennah ReblandoNoch keine Bewertungen
- Ertapenem (Invanz)Dokument1 SeiteErtapenem (Invanz)Adrianne BazoNoch keine Bewertungen
- Common Fears Related To Childbirth and Coping Mechanisms Among Primigravida MothersDokument42 SeitenCommon Fears Related To Childbirth and Coping Mechanisms Among Primigravida MothersSmile Tambanillo100% (1)
- The Problem and Its BackgroundDokument44 SeitenThe Problem and Its Backgroundmhaychelle_24100% (1)
- Fdar-Pedia WardDokument1 SeiteFdar-Pedia WardSyrelle GomezNoch keine Bewertungen
- Sample 3Dokument42 SeitenSample 3VeniceNoch keine Bewertungen
- NCP HemorrhoidsDokument2 SeitenNCP Hemorrhoidsnurse_yramenaj0% (1)
- Benign Prostatic Hyperplasia (NCP)Dokument4 SeitenBenign Prostatic Hyperplasia (NCP)24 PAULINO ALDRIN MUJARNoch keine Bewertungen
- Burn - Daily Physical AssessmentDokument8 SeitenBurn - Daily Physical AssessmentkrishcelNoch keine Bewertungen
- COURSE OBJECTIVES or NursingDokument5 SeitenCOURSE OBJECTIVES or NursingFil AquinoNoch keine Bewertungen
- Case Presentation CsDokument18 SeitenCase Presentation CsgenzpogiiNoch keine Bewertungen
- Xiii. Discharge Planning: Carbohydrates NutrientsDokument4 SeitenXiii. Discharge Planning: Carbohydrates Nutrientsgroupbsection1Noch keine Bewertungen
- Diagnostics - Nursing ResponsibilitiesDokument9 SeitenDiagnostics - Nursing ResponsibilitiesCarmellaDawn100% (3)
- Drugs BipolarDokument4 SeitenDrugs BipolarSheana TmplNoch keine Bewertungen
- Journal DengueDokument3 SeitenJournal DengueCee SanchezNoch keine Bewertungen
- Health Teaching of Patients With Tuberculosis TreatmentDokument34 SeitenHealth Teaching of Patients With Tuberculosis TreatmentFarhanaRahimNoch keine Bewertungen
- Losartan Plus HydrochlorothiazideDokument18 SeitenLosartan Plus Hydrochlorothiazidegmsanto7Noch keine Bewertungen
- Impaired Tissue Perfusion Related To The Weakening / Decreased Blood Flow To The Area of Gangrene Due To Obstruction of Blood VesselsDokument3 SeitenImpaired Tissue Perfusion Related To The Weakening / Decreased Blood Flow To The Area of Gangrene Due To Obstruction of Blood VesselsKat AlaNoch keine Bewertungen
- Burn - Concept MapDokument1 SeiteBurn - Concept MapAaron RafaelNoch keine Bewertungen
- Tahbso ArticleDokument4 SeitenTahbso ArticleAlianna Kristine OhNoch keine Bewertungen
- Quiz LeukemiaDokument4 SeitenQuiz LeukemiaHanna La MadridNoch keine Bewertungen
- Valoración Geriátrica IntegralDokument13 SeitenValoración Geriátrica IntegralBlackthestralNoch keine Bewertungen
- MD Assessment KFRDokument30 SeitenMD Assessment KFRHasna Diyani Salamah100% (1)
- Chap.10 Health PsychologyDokument29 SeitenChap.10 Health PsychologymariaNoch keine Bewertungen
- List of Successful Examinees Who Garnered The Ten (10) Highest PlacesDokument2 SeitenList of Successful Examinees Who Garnered The Ten (10) Highest PlacesKeith Giomeer PetrolaNoch keine Bewertungen
- Republic of The Philippines Professional Regulation Commission ManilaDokument20 SeitenRepublic of The Philippines Professional Regulation Commission Manilawallyboy_casugaNoch keine Bewertungen
- Antibiotic Therapeutics in Laboratory AnimalsDokument21 SeitenAntibiotic Therapeutics in Laboratory AnimalsKeith Giomeer PetrolaNoch keine Bewertungen
- Can Your LinkedIn Profile Truly Increase Your Chances of Getting Hired?Dokument3 SeitenCan Your LinkedIn Profile Truly Increase Your Chances of Getting Hired?Keith Giomeer PetrolaNoch keine Bewertungen
- NLE2011 SchoolsDokument20 SeitenNLE2011 SchoolsHarby Ongbay AbellanosaNoch keine Bewertungen
- June 2012 Nle Passers Complete ListDokument557 SeitenJune 2012 Nle Passers Complete ListEli Benjamin Nava TaclinoNoch keine Bewertungen
- Invitation SampleDokument2 SeitenInvitation SampleKeith Giomeer PetrolaNoch keine Bewertungen
- July 2011 Nursing Board Exam Top 10 Successful ExamineesDokument2 SeitenJuly 2011 Nursing Board Exam Top 10 Successful ExamineesPhilippineNursingDirectory.comNoch keine Bewertungen
- Dec NleDokument456 SeitenDec Nleniel_oroNoch keine Bewertungen
- Performance of School July 2011 Nursing Board Exam ResultsDokument20 SeitenPerformance of School July 2011 Nursing Board Exam ResultsjuancristoNoch keine Bewertungen
- List of PassersDokument751 SeitenList of PassersJeanhel AuditorNoch keine Bewertungen
- ICT Transforming Healthcare Education PhilippinesDokument5 SeitenICT Transforming Healthcare Education PhilippinesCherielyn MercadoNoch keine Bewertungen
- Full Text of The Official Result of December 2011 Nurse Licensure ExaminationDokument19 SeitenFull Text of The Official Result of December 2011 Nurse Licensure ExaminationRay Andrew del RosarioNoch keine Bewertungen
- PINOYBSNJuly 2011 Nursing Board Exam Result Top Performing SchoolsDokument19 SeitenPINOYBSNJuly 2011 Nursing Board Exam Result Top Performing Schoolspinoybsn1192Noch keine Bewertungen
- December 2010 NLE RESULTS (A-I)Dokument383 SeitenDecember 2010 NLE RESULTS (A-I)Keith Giomeer PetrolaNoch keine Bewertungen
- Foundations of Nursing PracticeDokument10 SeitenFoundations of Nursing PracticeRomeo Casiano Jr.Noch keine Bewertungen
- Schools Ratings - December 2010 Nurse Licensure ExaminationDokument19 SeitenSchools Ratings - December 2010 Nurse Licensure ExaminationLyle Santos0% (1)
- December 2010 Nursing Board Exam Results (P-Z)Dokument233 SeitenDecember 2010 Nursing Board Exam Results (P-Z)Keith Giomeer PetrolaNoch keine Bewertungen
- (FINAL) Clinical Rotation - First PageDokument1 Seite(FINAL) Clinical Rotation - First PageKeith Giomeer PetrolaNoch keine Bewertungen
- December 2010 NLE RESULTS (J-O)Dokument166 SeitenDecember 2010 NLE RESULTS (J-O)Keith Giomeer PetrolaNoch keine Bewertungen
- Old Caseload FormsDokument5 SeitenOld Caseload FormskimmieeyNoch keine Bewertungen
- Upcnso-Tn App FormDokument3 SeitenUpcnso-Tn App FormKeith Giomeer PetrolaNoch keine Bewertungen
- University of Pangasinan PHINMA Education Network College of Nursing QUESTION ON COMPETENCY (CHED Published On Manila Today and Manila BulletinDokument7 SeitenUniversity of Pangasinan PHINMA Education Network College of Nursing QUESTION ON COMPETENCY (CHED Published On Manila Today and Manila BulletinKeith Giomeer PetrolaNoch keine Bewertungen
- TheDose Election Watch - Region 1 - MANGALDAN An Official Tally RESULTSDokument13 SeitenTheDose Election Watch - Region 1 - MANGALDAN An Official Tally RESULTSKeith Giomeer PetrolaNoch keine Bewertungen
- TheDose Election Watch - Region 1 - Pangasinan NATIONAL Level RESULTSDokument11 SeitenTheDose Election Watch - Region 1 - Pangasinan NATIONAL Level RESULTSKeith Giomeer PetrolaNoch keine Bewertungen
- WebinabsDokument336 SeitenWebinabssacin99999Noch keine Bewertungen
- EnVisorA1 User' SGuide enDokument366 SeitenEnVisorA1 User' SGuide enFrank QuitianNoch keine Bewertungen
- 2010 TFN Module Unit 06 Nursing Paradigm - NursingDokument43 Seiten2010 TFN Module Unit 06 Nursing Paradigm - NursingCamille Denise Nucum100% (1)
- FY10 ICD-9-CM Procedure Codes Linked To NHSN Operative Procedure CategoriesDokument22 SeitenFY10 ICD-9-CM Procedure Codes Linked To NHSN Operative Procedure CategoriesYohan Julian Mega NandaNoch keine Bewertungen
- DR Kshitij ResumeDokument3 SeitenDR Kshitij ResumeBarney StinsonNoch keine Bewertungen
- INTRODUCTION of Tuberculosis Final NewDokument2 SeitenINTRODUCTION of Tuberculosis Final Newbatch1Noch keine Bewertungen
- Urinary Incontinence Following Gynaecological SurgeryDokument6 SeitenUrinary Incontinence Following Gynaecological SurgeryDwickyNoch keine Bewertungen
- Platinum Gazette 11 JuneDokument16 SeitenPlatinum Gazette 11 JuneAnonymous w8NEyXNoch keine Bewertungen
- 2021 American College of Rheumatology Guideline For The Treatment of Rheumatoid ArthritisDokument30 Seiten2021 American College of Rheumatology Guideline For The Treatment of Rheumatoid Arthritisjose pablo quero reyesNoch keine Bewertungen
- InflammationDokument41 SeitenInflammationbharath goNoch keine Bewertungen
- 41ch44circulatory12008 RevisedDokument33 Seiten41ch44circulatory12008 RevisedJosh TejadaNoch keine Bewertungen
- Tetracyclines: Dr. Md. Rageeb Md. Usman Associate Professor Department of PharmacognosyDokument21 SeitenTetracyclines: Dr. Md. Rageeb Md. Usman Associate Professor Department of PharmacognosyAnonymous TCbZigVqNoch keine Bewertungen
- Acute Abdomen in Pediatric Patients Admitted To PDFDokument9 SeitenAcute Abdomen in Pediatric Patients Admitted To PDFiwanNoch keine Bewertungen
- Bone Marrow BiopsyDokument2 SeitenBone Marrow BiopsySatinder SinghNoch keine Bewertungen
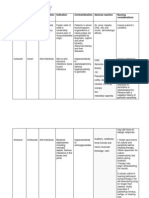
- Drug Name Dosage, Route, Frequency Mechanism of Action Indication Contraindication Adverse Effect Nursing ResponsibilitiesDokument1 SeiteDrug Name Dosage, Route, Frequency Mechanism of Action Indication Contraindication Adverse Effect Nursing ResponsibilitiesJonna Mae TurquezaNoch keine Bewertungen
- Sprain and DislocationDokument9 SeitenSprain and Dislocationbhavesh jain100% (1)
- Synthesis PaperDokument19 SeitenSynthesis Paperapi-330084238Noch keine Bewertungen
- Herb-Drug Int 2008Dokument58 SeitenHerb-Drug Int 2008Pauline OctavianiNoch keine Bewertungen
- 128 Salicylic Rohdia MSDSDokument13 Seiten128 Salicylic Rohdia MSDSWike Wingtias ArnesaNoch keine Bewertungen
- OFLOXACINDokument3 SeitenOFLOXACINfayrouz fathiNoch keine Bewertungen