Das könnte Ihnen auch gefallen
- 4.4 Emerging and Re-Emerging Infectious DiseaseDokument75 Seiten4.4 Emerging and Re-Emerging Infectious DiseasenorazlienaNoch keine Bewertungen
- Intrauterine Growth RestrictionDokument4 SeitenIntrauterine Growth RestrictionFate ZephyrNoch keine Bewertungen
- Pregnancy Induced Hypertension PihDokument17 SeitenPregnancy Induced Hypertension PihRose DeymNoch keine Bewertungen
- New Born Care: Catheter SuctioningDokument17 SeitenNew Born Care: Catheter SuctioningRaffy100% (1)
- RX Protocol by DR - Anwarul Azim PDFDokument120 SeitenRX Protocol by DR - Anwarul Azim PDFGB Majumder100% (1)
- Analgesics in ObstetricsDokument33 SeitenAnalgesics in ObstetricsVeena KaNoch keine Bewertungen
- Prolonged PregnancyDokument40 SeitenProlonged Pregnancyjan caraNoch keine Bewertungen
- Immunisation ScheduleDokument3 SeitenImmunisation SchedulejegathesmsjsNoch keine Bewertungen
- Immunitization and VaccinationDokument46 SeitenImmunitization and VaccinationMazhar RehmanNoch keine Bewertungen
- Principles of Medical Technology Practice 1Dokument6 SeitenPrinciples of Medical Technology Practice 1Em-em Cantos88% (17)
- Immunization LectureDokument32 SeitenImmunization LectureMekdes ZewdeNoch keine Bewertungen
- Drug Study (Amiodarone)Dokument8 SeitenDrug Study (Amiodarone)Justine Conui100% (1)
- Comparative Study For Efficacy of Termination in First Trimester Pregnancy Using Misoprostol and MifepristoneDokument9 SeitenComparative Study For Efficacy of Termination in First Trimester Pregnancy Using Misoprostol and MifepristonePeertechz Publications Inc.Noch keine Bewertungen
- Immunization Division at Mohfw Universal Immunization Program (Uip)Dokument21 SeitenImmunization Division at Mohfw Universal Immunization Program (Uip)Shekhar MishraNoch keine Bewertungen
- Introduction of MidwiferyDokument7 SeitenIntroduction of MidwiferyNirmala PokharelNoch keine Bewertungen
- KMCDokument23 SeitenKMCStefanie Pramudita JayaNoch keine Bewertungen
- Estimation of Fetal WeightDokument38 SeitenEstimation of Fetal Weightkennedy14344Noch keine Bewertungen
- Universal Immunization ProgramDokument15 SeitenUniversal Immunization Programsmruti ranjanNoch keine Bewertungen
- Abortion India Lit ReviewDokument48 SeitenAbortion India Lit ReviewPrathibha GuruguriNoch keine Bewertungen
- A Prospective Comparative Study of 3 Different Regimens Involving Mifepristone and Oral/ Vaginalmisoprostol Combination in Medical Termination of Pregnancy at Less Than 9 Weeks GestationDokument6 SeitenA Prospective Comparative Study of 3 Different Regimens Involving Mifepristone and Oral/ Vaginalmisoprostol Combination in Medical Termination of Pregnancy at Less Than 9 Weeks Gestationstudy obg with me surbhiNoch keine Bewertungen
- Fetal Biophysical Profile PDFDokument2 SeitenFetal Biophysical Profile PDFVickiNoch keine Bewertungen
- Antenatal Care Guidelines: Doctors of The WorldDokument16 SeitenAntenatal Care Guidelines: Doctors of The WorldNadiah FtrNoch keine Bewertungen
- LBW, Care & FeedingDokument34 SeitenLBW, Care & FeedingManju KumariNoch keine Bewertungen
- Postnatal CareDokument62 SeitenPostnatal CareKonstantinos Papadakis100% (1)
- Antenatal CareDokument25 SeitenAntenatal CareDrBhagyashree BhatNoch keine Bewertungen
- Acute Respiratory InfectionsDokument26 SeitenAcute Respiratory InfectionsSuneel SagareNoch keine Bewertungen
- PoliomyelitisDokument46 SeitenPoliomyelitisBareera Nudrat100% (1)
- National Rural Health MissionDokument17 SeitenNational Rural Health MissionShubham DwivediNoch keine Bewertungen
- PolioDokument64 SeitenPoliodeean faqihNoch keine Bewertungen
- Vaccinations in PregnancyDokument137 SeitenVaccinations in PregnancyAmine YounisNoch keine Bewertungen
- Mandibular Nerve Block (Other Techniques)Dokument24 SeitenMandibular Nerve Block (Other Techniques)daw022100% (2)
- Immunization For New-Born ChildDokument19 SeitenImmunization For New-Born ChildyashNoch keine Bewertungen
- (MMUNISATIONDokument54 Seiten(MMUNISATIONatharva sawantNoch keine Bewertungen
- Lesson Plan of Conference PDFDokument44 SeitenLesson Plan of Conference PDFRahul DamorNoch keine Bewertungen
- Advantages of Breast FeedingDokument4 SeitenAdvantages of Breast FeedingRollan MaulasNoch keine Bewertungen
- Polio VirusDokument12 SeitenPolio VirusNovianaHartikasariNoch keine Bewertungen
- Nature, Types, Causes and Methods of Abortion: ChapterDokument38 SeitenNature, Types, Causes and Methods of Abortion: ChapterBHUKYA USHARANINoch keine Bewertungen
- Poliomyelitis: By: Reema I. DabbasDokument35 SeitenPoliomyelitis: By: Reema I. DabbasReema DabbasNoch keine Bewertungen
- Preventive ObstetricsDokument8 SeitenPreventive ObstetricsMahima LalNoch keine Bewertungen
- Medical Termination of PregnencyDokument19 SeitenMedical Termination of PregnencyTijilNoch keine Bewertungen
- Prenatal Care by Connie Sussan AustenDokument31 SeitenPrenatal Care by Connie Sussan AustenNoraNoch keine Bewertungen
- Breast FeedingDokument3 SeitenBreast FeedingArla Donissa-Donique Castillon AlviorNoch keine Bewertungen
- Artificial Respiration FDokument30 SeitenArtificial Respiration FKousalyaNoch keine Bewertungen
- 84 Vaccine Preventable Diseases and Immunization Programs FINAL 0 PDFDokument91 Seiten84 Vaccine Preventable Diseases and Immunization Programs FINAL 0 PDFhassanNoch keine Bewertungen
- Promoting Nutritional Health During Pregnancy 19-20Dokument25 SeitenPromoting Nutritional Health During Pregnancy 19-20Tony KhattarNoch keine Bewertungen
- AbortionDokument92 SeitenAbortionniraj_sdNoch keine Bewertungen
- RMNCH + A: (Reproductive, Maternal, Newborn, Child and Adolescent Health Strategy)Dokument11 SeitenRMNCH + A: (Reproductive, Maternal, Newborn, Child and Adolescent Health Strategy)Monica FreedaNoch keine Bewertungen
- Anatomy and Physiology: Functions of The UterusDokument6 SeitenAnatomy and Physiology: Functions of The UterusAnthony jesusNoch keine Bewertungen
- East FeedingDokument5 SeitenEast FeedingJeya vanithaNoch keine Bewertungen
- 7 VaccinesDokument21 Seiten7 VaccinesaqwsedrftghyujikolpNoch keine Bewertungen
- AnthopometryDokument44 SeitenAnthopometryghifari2007Noch keine Bewertungen
- Contraceptive Options For Women and Couples With HIV: Intrauterine Device (Iud or Iucd)Dokument23 SeitenContraceptive Options For Women and Couples With HIV: Intrauterine Device (Iud or Iucd)Claudio UdjajaNoch keine Bewertungen
- PPIUCD Training Module 2013 (MO & SN)Dokument188 SeitenPPIUCD Training Module 2013 (MO & SN)Nachiket DeshpandeNoch keine Bewertungen
- Unit 5 Normal Puerperium and Nursing Management: 5.0 ObjectivesDokument14 SeitenUnit 5 Normal Puerperium and Nursing Management: 5.0 ObjectivesJissa Daison100% (1)
- Oxygen Therapy and Oxygen Delivery (Pediatric) - CEDokument8 SeitenOxygen Therapy and Oxygen Delivery (Pediatric) - CEViviana AltamiranoNoch keine Bewertungen
- Second Stage of Labor: Cervancia, Eunice Dator, Angelica F. Endaya, KryshaDokument11 SeitenSecond Stage of Labor: Cervancia, Eunice Dator, Angelica F. Endaya, KryshaAprilene Angel Balaque ZunegaNoch keine Bewertungen
- PMTCTDokument26 SeitenPMTCTMaxwell C Jay KafwaniNoch keine Bewertungen
- Icds-Integrated Child Development ServiceDokument12 SeitenIcds-Integrated Child Development ServiceAngel AngelNoch keine Bewertungen
- High Risk PregnancyDokument33 SeitenHigh Risk PregnancyDakshayini MbNoch keine Bewertungen
- GarbhaKaal - A Happy JourneyDokument23 SeitenGarbhaKaal - A Happy Journeyआदित्य मोदीNoch keine Bewertungen
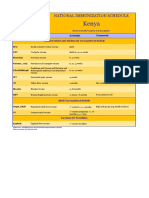
- Kenya Immunization ScheduleDokument1 SeiteKenya Immunization ScheduleDani AnyikaNoch keine Bewertungen
- Pediatric PoisoningsDokument45 SeitenPediatric PoisoningsErwin Jake Taguba100% (1)
- Health Related SchemesDokument7 SeitenHealth Related SchemesPriyam MhashilkarNoch keine Bewertungen
- Fetal SkullDokument11 SeitenFetal SkullRinkish DalliahNoch keine Bewertungen
- Glimepiride Prescribing InformationDokument16 SeitenGlimepiride Prescribing InformationMohammed Shamiul ShahidNoch keine Bewertungen
- Assignment 10 χ²-test (B. V. Sc. & A.H. 2017 batch) Type A: χ² - Test of goodness of fitDokument7 SeitenAssignment 10 χ²-test (B. V. Sc. & A.H. 2017 batch) Type A: χ² - Test of goodness of fitK0% (1)
- Assessment of Knowledge, Attitude and Awareness Regarding Cone Beam Computed Tomography Among Dental Graduates in Pune City, IndiaDokument5 SeitenAssessment of Knowledge, Attitude and Awareness Regarding Cone Beam Computed Tomography Among Dental Graduates in Pune City, IndiaSakina JigarNoch keine Bewertungen
- A Special Interview With Dr. Meryl Nass by Dr. Joseph MercolaDokument9 SeitenA Special Interview With Dr. Meryl Nass by Dr. Joseph MercolaJonathan Robert Kraus (OutofMudProductions)Noch keine Bewertungen
- Home-Made HBsAgDokument1 SeiteHome-Made HBsAgsomchaisNoch keine Bewertungen
- Wu (2009) Treatment of ChordomasDokument4 SeitenWu (2009) Treatment of ChordomasIvo Baaron ZarkovNoch keine Bewertungen
- The Proportion of Diploid 46 XX CellsDokument6 SeitenThe Proportion of Diploid 46 XX CellsAntonio Lazo De La VegaNoch keine Bewertungen
- MCN 2Dokument11 SeitenMCN 2karenkaren09Noch keine Bewertungen
- S.N. System ID Name Speciality Guide: School of Nursing and ResearchDokument6 SeitenS.N. System ID Name Speciality Guide: School of Nursing and ResearchBhawna JoshiNoch keine Bewertungen
- Problem 1 Emergency Medicine Block: Agustina Cynthia Cesari S 405140066 Group 1Dokument90 SeitenProblem 1 Emergency Medicine Block: Agustina Cynthia Cesari S 405140066 Group 1Astri GunardiNoch keine Bewertungen
- Probiotic Allergic RhinitsDokument7 SeitenProbiotic Allergic Rhinitscharoline gracetiani nataliaNoch keine Bewertungen
- A Review of The New GLP-1 Receptor Agonist/basal Insulin Fixed-Ratio Combination ProductsDokument11 SeitenA Review of The New GLP-1 Receptor Agonist/basal Insulin Fixed-Ratio Combination Productsarief hakikiNoch keine Bewertungen
- Abatacept Hervey2006Dokument9 SeitenAbatacept Hervey2006Calvin Tanuwijaya Stick BolaNoch keine Bewertungen
- Normal Spontaneous DeliveryDokument4 SeitenNormal Spontaneous Deliveryvivian magnoNoch keine Bewertungen
- A Silent KillerDokument3 SeitenA Silent KillerLinhNguyeNoch keine Bewertungen
- M. J. L. Alexander, MSC, PHD: Med Sci Sports Exerc 37:1814-1819, 2005Dokument2 SeitenM. J. L. Alexander, MSC, PHD: Med Sci Sports Exerc 37:1814-1819, 2005steNoch keine Bewertungen
- PHARMACOTHERAPEUTICS - II CASE PRESENTATION ON PSORIASIS by SRIRAM ADokument21 SeitenPHARMACOTHERAPEUTICS - II CASE PRESENTATION ON PSORIASIS by SRIRAM ASriram Surya100% (1)
- Multi-Frequency and Multi-Component TympanometryDokument8 SeitenMulti-Frequency and Multi-Component TympanometryEstudiantede FonoaudiologíaNoch keine Bewertungen
- Fenotipos Bioquímicos y Fagotipos de Cepas de Salmonella Enteritidis Aisladas en Antofagasta, 1997-2000Dokument9 SeitenFenotipos Bioquímicos y Fagotipos de Cepas de Salmonella Enteritidis Aisladas en Antofagasta, 1997-2000axel vargasNoch keine Bewertungen
- AsplDokument9 SeitenAsplCristinaNoch keine Bewertungen
- Marc A. Levitt: AuthorDokument16 SeitenMarc A. Levitt: AuthorAlonso Rodriguez EscobedoNoch keine Bewertungen
- Growth Faltering, Puberty and Growth ChartsDokument4 SeitenGrowth Faltering, Puberty and Growth ChartsCaine ReganNoch keine Bewertungen
- Iowa Neonatology HandbookDokument11 SeitenIowa Neonatology HandbookLowelly napitupuluNoch keine Bewertungen
- Summary and Conclusions: Urinary Biomarkers in Experimental DiabetesDokument1 SeiteSummary and Conclusions: Urinary Biomarkers in Experimental DiabetesNikesh DoshiNoch keine Bewertungen
- A Pharmacology-Based Comprehensive Review On Medicinal PlantsDokument14 SeitenA Pharmacology-Based Comprehensive Review On Medicinal PlantsissamebenNoch keine Bewertungen
- Percutaneous Nephrolithotomy Made Easier: A Practical Guide, Tips and TricksDokument5 SeitenPercutaneous Nephrolithotomy Made Easier: A Practical Guide, Tips and TricksJihad AnadNoch keine Bewertungen