Das könnte Ihnen auch gefallen
- This Study Resource Was Shared Via: Sinus BradycardiaDokument3 SeitenThis Study Resource Was Shared Via: Sinus BradycardiaPascal St Peter NwaorguNoch keine Bewertungen
- ArrhythmiaDokument2 SeitenArrhythmiaChris Pritchard93% (30)
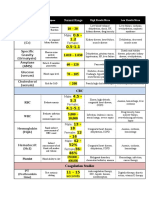
- Lab ValuesDokument3 SeitenLab Valuessurviving nursing school100% (1)
- Cardiac MedicationsDokument9 SeitenCardiac Medicationsnovikane100% (1)
- ECG Master Class-2Dokument138 SeitenECG Master Class-2Shohag ID Center100% (1)
- Common Cardiac MedicationsDokument1 SeiteCommon Cardiac MedicationsPaige HardekopfNoch keine Bewertungen
- Ecg StripsDokument39 SeitenEcg StripsNursyNurse100% (3)
- Cardiac Meds ChartDokument1 SeiteCardiac Meds ChartCharlotte Louise75% (4)
- ECG ReadingDokument11 SeitenECG ReadingSuresh Shrestha100% (1)
- Spotlight On Cardiac DrugsDokument2 SeitenSpotlight On Cardiac Drugspauerish100% (2)
- ArrhyDokument26 SeitenArrhyMouriyan AmanNoch keine Bewertungen
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsVon EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNoch keine Bewertungen
- Dysrhythmia Recognition Pocket Reference Card PDFDokument14 SeitenDysrhythmia Recognition Pocket Reference Card PDFjenn1722100% (2)
- EKG Flash Cards PDFDokument9 SeitenEKG Flash Cards PDFdiani arisandhi100% (1)
- Cardiac Dysrhythmia Chart Med Surg NUR4 PDFDokument3 SeitenCardiac Dysrhythmia Chart Med Surg NUR4 PDFlml100% (1)
- DripsDokument52 SeitenDripsjanoloNoch keine Bewertungen
- Dysrhythmias ChartDokument6 SeitenDysrhythmias Chartjkrix100% (1)
- ECG Master Class-1Dokument132 SeitenECG Master Class-1Shohag ID Center100% (1)
- Aclsrhythmtest11 PDFDokument7 SeitenAclsrhythmtest11 PDFmonir610% (1)
- EKG Cardiac Rhythm Analysis PDFDokument80 SeitenEKG Cardiac Rhythm Analysis PDFIqbal Juher100% (1)
- Cardiac Meds CompleteDokument3 SeitenCardiac Meds CompleteDanielle100% (2)
- Pet Food 2Dokument73 SeitenPet Food 2AB100% (1)
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!Von EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!Noch keine Bewertungen
- EKG Flash CardsDokument5 SeitenEKG Flash CardsRyann Sampino FreitasNoch keine Bewertungen
- Ecg Reading NotesDokument17 SeitenEcg Reading NotesMarian FloresNoch keine Bewertungen
- Chest Tube Explanation by AllnursesDokument3 SeitenChest Tube Explanation by AllnursesYemaya84Noch keine Bewertungen
- Cardiac Rhythms and DysrhythmiasDokument14 SeitenCardiac Rhythms and DysrhythmiasShawn Gaurav Jha100% (1)
- Hemodynamic Drug InfusionsDokument45 SeitenHemodynamic Drug InfusionsDawit MucheNoch keine Bewertungen
- Ekg Made EasyDokument7 SeitenEkg Made Easystring44100% (3)
- Basic EKG Dysrhythmia IdentificationDokument40 SeitenBasic EKG Dysrhythmia IdentificationIlda Dhe Devis Spaho100% (1)
- ACLS Algorithm Pulse No Yes: Stable Patient Unstable Patient Stable PatientDokument1 SeiteACLS Algorithm Pulse No Yes: Stable Patient Unstable Patient Stable PatientAhmed AlkhaqaniNoch keine Bewertungen
- Cardiovascular I: CAD: Coronary Artery Disease (Most Common in US) Risk FactorsDokument4 SeitenCardiovascular I: CAD: Coronary Artery Disease (Most Common in US) Risk FactorsJessica100% (1)
- Anti-Arrhythmic Agents For Pharmacy PDFDokument41 SeitenAnti-Arrhythmic Agents For Pharmacy PDFKelvinTMaikanaNoch keine Bewertungen
- Classification of Psychiatric DisordersDokument64 SeitenClassification of Psychiatric Disordersdrkadiyala2100% (1)
- Basic Ecg Interpretation Practice Test V 1Dokument7 SeitenBasic Ecg Interpretation Practice Test V 1emmaaziz100% (1)
- ECG Dysrhthmias IIIDokument31 SeitenECG Dysrhthmias IIIAmani KayedNoch keine Bewertungen
- ECG StripsDokument5 SeitenECG StripsNursingSchoolNotes100% (1)
- RhythmDokument8 SeitenRhythmparkmickyboo100% (1)
- Module 1 Case StudyDokument5 SeitenModule 1 Case Studyapi-564432337100% (1)
- CardiopathophysiologyDokument63 SeitenCardiopathophysiologyapplesncoreNoch keine Bewertungen
- Cardiac MedsDokument7 SeitenCardiac MedsMary Fair DelcidNoch keine Bewertungen
- Cardiac Rhythms - ECG ReadingsDokument15 SeitenCardiac Rhythms - ECG Readingsal-obinay shereenNoch keine Bewertungen
- Dimensional Analysis For Nursing StudentsVon EverandDimensional Analysis For Nursing StudentsNoch keine Bewertungen
- EKG RhythmsDokument10 SeitenEKG RhythmsQueenNoch keine Bewertungen
- Nursing School EKGDokument43 SeitenNursing School EKGRob Dickerson100% (1)
- BASIC ECG READING For Nle NOVEMBER 2018Dokument63 SeitenBASIC ECG READING For Nle NOVEMBER 2018Sharmaine KimmayongNoch keine Bewertungen
- Practice ECGStripsDokument300 SeitenPractice ECGStripsFarid RodríguezNoch keine Bewertungen
- Module 2 Case Study StudentfDokument4 SeitenModule 2 Case Study Studentfapi-675875543Noch keine Bewertungen
- Critical Care - Hemodynamic Monitoring TableDokument7 SeitenCritical Care - Hemodynamic Monitoring TableVictoria Romero100% (2)
- Food Safety Officer and Technical Officer FSSAI Guide 2019 PDFDokument15 SeitenFood Safety Officer and Technical Officer FSSAI Guide 2019 PDFChinmoy Das0% (5)
- Healing PowersDokument9 SeitenHealing PowersJack Key Chan AntigNoch keine Bewertungen
- Cardiac DysrhythmiasDokument9 SeitenCardiac DysrhythmiasMandy JameroNoch keine Bewertungen
- Cardiac DysrhythmiasDokument3 SeitenCardiac DysrhythmiasWilbert GuerreroNoch keine Bewertungen
- DYSRHYTHMIASDokument15 SeitenDYSRHYTHMIASKristine CastilloNoch keine Bewertungen
- Clinical Log Term II PDFDokument9 SeitenClinical Log Term II PDFPriscilla S100% (1)
- Fitness Calculator Python ProjectDokument12 SeitenFitness Calculator Python ProjectNishitha NeelamNoch keine Bewertungen
- ACS AMI FacilitatorDokument21 SeitenACS AMI FacilitatorPaul Zantua57% (7)
- DYSRHYTHMIAS (A.k.a. Arrhythmias) Disorders in TheDokument3 SeitenDYSRHYTHMIAS (A.k.a. Arrhythmias) Disorders in TheDarell M. Book100% (1)
- Practice StripsDokument9 SeitenPractice StripsErica Yamamoto50% (4)
- Dysrhythmia Interpretation Modules 1-6 June 2012Dokument126 SeitenDysrhythmia Interpretation Modules 1-6 June 2012Jess Varose100% (3)
- Neonatal HyperglycemiaDokument18 SeitenNeonatal HyperglycemiayumicheongNoch keine Bewertungen
- Atlas de AcupunturaDokument258 SeitenAtlas de AcupunturaPatricia Barrera100% (2)
- NCM 106 - Case Analysis - Nursing Care Plan of Heart FailureDokument2 SeitenNCM 106 - Case Analysis - Nursing Care Plan of Heart FailureMarisol Jane JomayaNoch keine Bewertungen
- Cardiac Dysrhythmias For Heart PatientsDokument3 SeitenCardiac Dysrhythmias For Heart PatientsAlaa OmarNoch keine Bewertungen
- NCM 112 MSN Prelim Topic 4 Cardiac Rhythm DisordersDokument5 SeitenNCM 112 MSN Prelim Topic 4 Cardiac Rhythm DisordersKim Erida QuezonNoch keine Bewertungen
- Lec 4-Toxicity and Identification TestDokument46 SeitenLec 4-Toxicity and Identification TestShoaib MuhammadNoch keine Bewertungen
- Lecture 5 - Facial Pain and TMJ DiseaseDokument6 SeitenLecture 5 - Facial Pain and TMJ DiseaseJeff ChadwickNoch keine Bewertungen
- OB TriageDokument36 SeitenOB TriagerelinNoch keine Bewertungen
- Endocrine: QuestionsDokument14 SeitenEndocrine: QuestionsMuhammad Abubakar100% (1)
- Amla As A Health FoodDokument14 SeitenAmla As A Health FoodKUNAL MITTALNoch keine Bewertungen
- Pat An AnewDokument126 SeitenPat An AnewgshchurovskiyNoch keine Bewertungen
- Oregon Trail DiaryDokument4 SeitenOregon Trail Diaryapi-262078158Noch keine Bewertungen
- Cystic HygromaDokument2 SeitenCystic HygromaAmal AlahmariNoch keine Bewertungen
- PletizmografijaDokument29 SeitenPletizmografijaJelenaJankovNoch keine Bewertungen
- 2020 Article 773Dokument10 Seiten2020 Article 773bagas umam alwiNoch keine Bewertungen
- SaveBooklet BookletDokument120 SeitenSaveBooklet BookletRoscelie KhoNoch keine Bewertungen
- Entrez Digital Tools and UtilitiesDokument80 SeitenEntrez Digital Tools and UtilitiesGeorge Sebastian AntonyNoch keine Bewertungen
- Drug StudyDokument14 SeitenDrug StudyCj LowryNoch keine Bewertungen
- Drugs-1.ppt 0Dokument22 SeitenDrugs-1.ppt 0Esraa BahaaNoch keine Bewertungen
- One Health ConceptDokument2 SeitenOne Health ConceptYume AkamaiNoch keine Bewertungen
- US SchubertDokument21 SeitenUS SchubertNirmayi HomkarNoch keine Bewertungen
- Literature Review On Vegetable OilDokument8 SeitenLiterature Review On Vegetable Oilbteubwbnd100% (1)
- IFDEA Dental Anatomy Educational Teaching ResourceDokument38 SeitenIFDEA Dental Anatomy Educational Teaching ResourcelienhuongahNoch keine Bewertungen
- Plasmodium Infection (Malaria) : Medical ParasitologyDokument7 SeitenPlasmodium Infection (Malaria) : Medical ParasitologyBalisi Manuel FranciscoNoch keine Bewertungen
- Experience of Dental Caries in Mother/child Pairs: Association Between Risk Indicators and Dental CariesDokument8 SeitenExperience of Dental Caries in Mother/child Pairs: Association Between Risk Indicators and Dental CariesRisky Anita OktavianiNoch keine Bewertungen
- Bakar CD RobiwijayaDokument60 SeitenBakar CD RobiwijayaAsep Ribbat MNoch keine Bewertungen
- Recent Advances in The Management of Hypoxic-Ischemic Encephalopathy-IJPPDokument6 SeitenRecent Advances in The Management of Hypoxic-Ischemic Encephalopathy-IJPPdrtgodeNoch keine Bewertungen