Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- BCLC Staging System: Stage 0 PST 0, Child-Pugh A, Okuda 1Dokument1 SeiteBCLC Staging System: Stage 0 PST 0, Child-Pugh A, Okuda 1Syifa MustikaNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Gut Microbiome and Aging Physiological and MechaniDokument20 SeitenGut Microbiome and Aging Physiological and MechaniSyifa MustikaNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Cpe 15 097Dokument4 SeitenCpe 15 097Syifa MustikaNoch keine Bewertungen
- Mucosal Immune System, & The Role of Iga in The Mucosal ImmunityDokument6 SeitenMucosal Immune System, & The Role of Iga in The Mucosal ImmunitySyifa MustikaNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
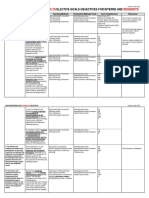
- Consults Residents: Gastroenterology /elective Goals-Objectives For Interns andDokument2 SeitenConsults Residents: Gastroenterology /elective Goals-Objectives For Interns andSyifa MustikaNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Gastroenterology2 CONFERENCESDokument1 SeiteGastroenterology2 CONFERENCESSyifa MustikaNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- UEG Week Vienna 2014 - Abstract Issue PDFDokument661 SeitenUEG Week Vienna 2014 - Abstract Issue PDFSyifa MustikaNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Energy Requirements For AdultsDokument3 SeitenEnergy Requirements For AdultsSyifa MustikaNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Poison 1Dokument24 SeitenPoison 1Scott LarsonNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Mna Mini EnglishDokument1 SeiteMna Mini EnglishSyifa MustikaNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Nutritional AssessmentDokument27 SeitenNutritional AssessmentSyifa MustikaNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Universal PrecautionDokument39 SeitenUniversal PrecautionSyifa MustikaNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Pharmakokinetic Protein TherpeuticsDokument29 SeitenPharmakokinetic Protein TherpeuticsSyifa MustikaNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Intrferon 2bDokument9 SeitenIntrferon 2bSyifa MustikaNoch keine Bewertungen
- Code of Conduct Farmasi PDFDokument38 SeitenCode of Conduct Farmasi PDFSyifa MustikaNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Argon Plasma Coagulation PDFDokument4 SeitenArgon Plasma Coagulation PDFSyifa MustikaNoch keine Bewertungen
- Case Pres ZandiOrstDokument17 SeitenCase Pres ZandiOrstNajeeb UllahNoch keine Bewertungen
- Approach To Common Respiratory DiseaseDokument57 SeitenApproach To Common Respiratory DiseaseRajhmuniran KandasamyNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Emory IMDokument29 SeitenEmory IMBeká BakhtadzeNoch keine Bewertungen
- Geriatric Index of Comorbidity: Validation and Comparison With Other Measures of ComorbidityDokument9 SeitenGeriatric Index of Comorbidity: Validation and Comparison With Other Measures of ComorbidityDesya EspriliaNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Code of Ethics For Nurses (ICN.2006)Dokument4 SeitenCode of Ethics For Nurses (ICN.2006)Bianx BoseNoch keine Bewertungen
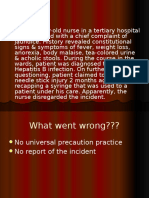
- Ional (Sir, Even Though I Know You Don't Like This Format But I Can't Help To Do So.)Dokument3 SeitenIonal (Sir, Even Though I Know You Don't Like This Format But I Can't Help To Do So.)Princess Joy CubangbangNoch keine Bewertungen
- Policy Brief:: South Africa and The Hiv/Aids Question: Will The Government Ever Find A Solution?Dokument13 SeitenPolicy Brief:: South Africa and The Hiv/Aids Question: Will The Government Ever Find A Solution?Ipeleng BosilongNoch keine Bewertungen
- Mcinnes2005 Mutismo SelectivoDokument10 SeitenMcinnes2005 Mutismo SelectivoCamila SiebzehnerNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- USGS BudgetDokument330 SeitenUSGS BudgetSummitVoiceNoch keine Bewertungen
- Liver MCQDokument14 SeitenLiver MCQMohammad Ra'fat Rostom86% (7)
- Bi Support Groups1Dokument6 SeitenBi Support Groups1api-301357752Noch keine Bewertungen
- Preface ReprintDokument19 SeitenPreface ReprintMusfiraNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Inclusive Classroom-Challenges With Special Reference To Child inDokument13 SeitenInclusive Classroom-Challenges With Special Reference To Child inRehna FathimaNoch keine Bewertungen
- Persuasive Essay PDFDokument5 SeitenPersuasive Essay PDFapi-603689898Noch keine Bewertungen
- History of Spinal Disorders: Philipp Gruber, Thomas BoeniDokument2 SeitenHistory of Spinal Disorders: Philipp Gruber, Thomas BoeniVictor CristianNoch keine Bewertungen
- Коспект лекційDokument51 SeitenКоспект лекційМарія МайорчакNoch keine Bewertungen
- 20190813033948amassgn. 12 Physical Edu.Dokument4 Seiten20190813033948amassgn. 12 Physical Edu.Sonica GuptaNoch keine Bewertungen
- Historical Development of Social Case Work Unit - 1Dokument10 SeitenHistorical Development of Social Case Work Unit - 1आई सी एस इंस्टीट्यूट60% (5)
- Medical Sociology 3rd Main Ppts 1Dokument193 SeitenMedical Sociology 3rd Main Ppts 1Pankaj Patil100% (1)
- MCQ AnswersDokument7 SeitenMCQ AnswersJeyarajasekar TtrNoch keine Bewertungen
- Swasthya Samaj Sahbhagita FoundationDokument95 SeitenSwasthya Samaj Sahbhagita FoundationSA DIGITAL SOLUTIONSNoch keine Bewertungen
- Jurnal AntibiotikDokument5 SeitenJurnal AntibiotikSela PutrianaNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Kirtika Chopra ResumeDokument1 SeiteKirtika Chopra ResumekirtikaNoch keine Bewertungen
- A Risk and ResilienceDokument20 SeitenA Risk and ResilienceFlaviu Alexandru MoraruNoch keine Bewertungen
- Lesson 3 How A Clinical Psychologist ThinksDokument7 SeitenLesson 3 How A Clinical Psychologist Thinksjericho anchetaNoch keine Bewertungen
- Psition Paper - Salupare - Ervin - DDokument2 SeitenPsition Paper - Salupare - Ervin - DErvin SalupareNoch keine Bewertungen
- IB Psychology - Abnormal Psychology Revision GuideDokument46 SeitenIB Psychology - Abnormal Psychology Revision GuideDhyan Valle97% (31)
- Bloodborne Pathogen Training PDFDokument22 SeitenBloodborne Pathogen Training PDFapi-282330630Noch keine Bewertungen
- Bronchial ObstructionDokument137 SeitenBronchial ObstructionGrajdianu Natalia100% (1)
- Risk Assessment Template - HouseDokument3 SeitenRisk Assessment Template - HouseSean SpencerNoch keine Bewertungen
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (3)