Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- RTC Seattle 2018 ScriptDokument52 SeitenRTC Seattle 2018 Script「MคQบi」Noch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Fruit and Vegetable Canning Business PlanDokument67 SeitenFruit and Vegetable Canning Business Plankyaq001100% (1)
- Microbiology Lecture NotesDokument116 SeitenMicrobiology Lecture NotesDodge StuffNoch keine Bewertungen
- Final Exam 10-CookeryDokument2 SeitenFinal Exam 10-CookeryMARY JOY VILLARUEL100% (5)
- Vampire Cheat SheetDokument4 SeitenVampire Cheat SheetAntónio Estêvão Alves FreitasNoch keine Bewertungen
- Hostel Prospectus 2017-18Dokument14 SeitenHostel Prospectus 2017-18Swapan BhowmickNoch keine Bewertungen
- Production Constraints and Marketing of Cut Flower (Gerbera) Under Poly-House Cultivation in Satara Region (Maharashtra)Dokument64 SeitenProduction Constraints and Marketing of Cut Flower (Gerbera) Under Poly-House Cultivation in Satara Region (Maharashtra)tanya sharmaNoch keine Bewertungen
- Lección Número 05 de Pimsleur English For Spanish Speakers Nivel 2Dokument5 SeitenLección Número 05 de Pimsleur English For Spanish Speakers Nivel 2William Gallego100% (1)
- Nathus FOCO PresentationDokument11 SeitenNathus FOCO Presentationa.dea.a.day3Noch keine Bewertungen
- Tài Liệu Thpt Quốc Gia Môn Tiếng Anh 2016Dokument155 SeitenTài Liệu Thpt Quốc Gia Môn Tiếng Anh 2016Lê Trung KiênNoch keine Bewertungen
- Bus620 Final Project - Team - White Collars Final SubmissionDokument23 SeitenBus620 Final Project - Team - White Collars Final SubmissionNusrat Sayeeda ChowdhuryNoch keine Bewertungen
- Coca Cola ProjectDokument96 SeitenCoca Cola ProjectAjay KumarNoch keine Bewertungen
- Pilgrimage of The El RocioDokument3 SeitenPilgrimage of The El RociopasferacosNoch keine Bewertungen
- Lista de Verbos Regulares e Irregulares 2021-22Dokument8 SeitenLista de Verbos Regulares e Irregulares 2021-22daniel salazarNoch keine Bewertungen
- Lesson 3 English Transcription CourseDokument15 SeitenLesson 3 English Transcription CourseLily Muñoz OrozcoNoch keine Bewertungen
- Basic DialoguesDokument131 SeitenBasic DialoguesElizabeth Simão MiguensNoch keine Bewertungen
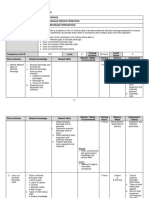
- HT CoCU E1 Alcoholic Beverage PreparationDokument10 SeitenHT CoCU E1 Alcoholic Beverage PreparationAnien Margaret FranklingNoch keine Bewertungen
- A Detailed Study On Frito LaysDokument12 SeitenA Detailed Study On Frito Laysajithjayan199050% (2)
- Food Processing IndustryDokument202 SeitenFood Processing IndustryAun GoveasNoch keine Bewertungen
- Brew Beer Like A Yeti - Chapter Three: GrainDokument22 SeitenBrew Beer Like A Yeti - Chapter Three: GrainChelsea Green PublishingNoch keine Bewertungen
- Parle Hide & Seek - SDM ReportDokument10 SeitenParle Hide & Seek - SDM ReportSai SurajNoch keine Bewertungen
- Introduction To Livestock Production and ManagementDokument3 SeitenIntroduction To Livestock Production and ManagementManoj KarkiNoch keine Bewertungen
- Kira Pearce - HL English Y2 - Senior Exit Project - Integrity EssayDokument3 SeitenKira Pearce - HL English Y2 - Senior Exit Project - Integrity Essayapi-462209151Noch keine Bewertungen
- Tallow SculpatureDokument15 SeitenTallow SculpatureDeepak KumarNoch keine Bewertungen
- 100 Resep Kue & Cake Populer Ny. Liem - Chendawati PDFDokument212 Seiten100 Resep Kue & Cake Populer Ny. Liem - Chendawati PDFRafaela Rosi100% (4)
- Brand (Pizza Hut) FinalDokument23 SeitenBrand (Pizza Hut) FinalcoolfahadNoch keine Bewertungen
- Ejercicios de Presente Continuo InglesDokument5 SeitenEjercicios de Presente Continuo InglestxikienaNoch keine Bewertungen
- FNCP FinaaaalDokument10 SeitenFNCP FinaaaalSoniaMarieBalanayNoch keine Bewertungen
- Fermentation: Cpi ReportDokument14 SeitenFermentation: Cpi ReportGlobal PMCNoch keine Bewertungen
- Recruitment and Selection Process of Nestle Tahliwal: Mrs. ShurabhiDokument31 SeitenRecruitment and Selection Process of Nestle Tahliwal: Mrs. Shurabhiellakkiya mn100% (1)