Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Fluid Electrolyte TherapyDokument15 SeitenFluid Electrolyte Therapyaarm1990Noch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- 1 SM 1Dokument7 Seiten1 SM 1Rivanli PoliiNoch keine Bewertungen
- Tekanan Darah Sebelum Senam Jantung: Bab Iv HasilDokument3 SeitenTekanan Darah Sebelum Senam Jantung: Bab Iv HasilAllium AdiNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- OkeDokument1 SeiteOkeAllium AdiNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Edema Brain Tumor JICM PDFDokument11 SeitenEdema Brain Tumor JICM PDFAllium AdiNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Coding HiperDokument17 SeitenCoding HiperAllium AdiNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Keratin-Based Products For Effective Wound Care Management in Superficial and Partial Thickness Burns InjuriesDokument7 SeitenKeratin-Based Products For Effective Wound Care Management in Superficial and Partial Thickness Burns InjuriesAllium AdiNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Esque Nazi 2015Dokument10 SeitenEsque Nazi 2015Felicia LinardiNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Edema Brain Tumor JICM PDFDokument11 SeitenEdema Brain Tumor JICM PDFAllium AdiNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Pot G Ieter 2017Dokument7 SeitenPot G Ieter 2017Allium AdiNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Edema Brain Tumor JICM PDFDokument11 SeitenEdema Brain Tumor JICM PDFAllium AdiNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Visual Auditory Kinaesthetic PDFDokument10 SeitenVisual Auditory Kinaesthetic PDFSelvi TamaraNoch keine Bewertungen
- Using Double Gloves in Surgical Procedures: A Literature ReviewDokument6 SeitenUsing Double Gloves in Surgical Procedures: A Literature ReviewAllium AdiNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- 1 s2.0 S0883944109001786 Main PDFDokument6 Seiten1 s2.0 S0883944109001786 Main PDFAllium AdiNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Important Role of Positioning in Nasogastric Tube Insertion in Unconscious Patients: A Prospective, Randomized, Double-Blind StudyDokument12 SeitenThe Important Role of Positioning in Nasogastric Tube Insertion in Unconscious Patients: A Prospective, Randomized, Double-Blind StudyAllium AdiNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Sukhotin Sky 2007Dokument20 SeitenSukhotin Sky 2007Allium AdiNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Respcare 02397 FullDokument17 SeitenRespcare 02397 FullAllium AdiNoch keine Bewertungen
- Jurnal KDKDokument7 SeitenJurnal KDKridhoillahidaredmiNoch keine Bewertungen
- The Application of Clinical Nursing Pathway in The Classification Diagnosis and Treatment of Patients With Emergency DyspneaDokument3 SeitenThe Application of Clinical Nursing Pathway in The Classification Diagnosis and Treatment of Patients With Emergency DyspneaAllium AdiNoch keine Bewertungen
- The Important Role of Positioning in Nasogastric Tube Insertion in Unconscious Patients: A Prospective, Randomized, Double-Blind StudyDokument12 SeitenThe Important Role of Positioning in Nasogastric Tube Insertion in Unconscious Patients: A Prospective, Randomized, Double-Blind StudyAllium AdiNoch keine Bewertungen
- Peserta Semnas 2015 REGISDokument28 SeitenPeserta Semnas 2015 REGISAllium AdiNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Roleplay SeminarnyaDokument8 SeitenRoleplay SeminarnyaAllium AdiNoch keine Bewertungen
- Musicmaker BrochureDokument32 SeitenMusicmaker BrochureNguyễn Vũ Minh Anh100% (1)
- To PPO-2014 ProviderManualDokument96 SeitenTo PPO-2014 ProviderManualHariadi WidodoNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Preoperative Education: Preoperative Preparation Allows Patients ToDokument6 SeitenPreoperative Education: Preoperative Preparation Allows Patients ToLorenn AdarnaNoch keine Bewertungen
- Medical Billing Questions 1Dokument7 SeitenMedical Billing Questions 1framar572112100% (1)
- 100 Cau Hoi Trac Nghiem Chuyen de Phrasal VerbsDokument10 Seiten100 Cau Hoi Trac Nghiem Chuyen de Phrasal VerbsThien le DangNoch keine Bewertungen
- Successful Implementation of A Pediatric Sedation Protocol For Mechanically Ventilated PatientsDokument6 SeitenSuccessful Implementation of A Pediatric Sedation Protocol For Mechanically Ventilated PatientsSantosa TandiNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Nursing Care PlanDokument4 SeitenNursing Care Planjopearl1889% (9)
- Closing Report - Tsotetsi - Steve Biko HospitalDokument57 SeitenClosing Report - Tsotetsi - Steve Biko HospitalDaily MaverickNoch keine Bewertungen
- Global Cancer Technology, Inc. Signs Licensing Agreement With The University of California San DiegoDokument2 SeitenGlobal Cancer Technology, Inc. Signs Licensing Agreement With The University of California San DiegoPR.comNoch keine Bewertungen
- Dha 123 AbcDokument264 SeitenDha 123 AbcilieoniciucNoch keine Bewertungen
- CT Icu Cover Letter - Kalyn MorimotoDokument1 SeiteCT Icu Cover Letter - Kalyn Morimotoapi-510593518Noch keine Bewertungen
- Health MaxhxchxhnagementDokument448 SeitenHealth MaxhxchxhnagementAlexandr TrotskyNoch keine Bewertungen
- Govt - MC Dental and Private MC Dental College 2Dokument4 SeitenGovt - MC Dental and Private MC Dental College 2Aslam HossainNoch keine Bewertungen
- FCP Network ListDokument150 SeitenFCP Network ListAjay KrishnanNoch keine Bewertungen
- Eleonor Mateo LopezDokument4 SeitenEleonor Mateo LopezmikomapaulenNoch keine Bewertungen
- CMHNDokument48 SeitenCMHNvikaNoch keine Bewertungen
- Pediatric Disaster PreparednessDokument196 SeitenPediatric Disaster Preparednessccbrown7100% (1)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Cot 2 - TleDokument11 SeitenCot 2 - TleBETHUEL P. ALQUIROZNoch keine Bewertungen
- Chapter 1 The Practice of Medicine Harrisons Internal MedicineDokument11 SeitenChapter 1 The Practice of Medicine Harrisons Internal Medicinenescafe1983Noch keine Bewertungen
- Poster Burkholderia + Reference FixDokument7 SeitenPoster Burkholderia + Reference Fixchew tiarsondangNoch keine Bewertungen
- Radiology Request Forms ResearchDokument8 SeitenRadiology Request Forms Researchtruevine_ministryNoch keine Bewertungen
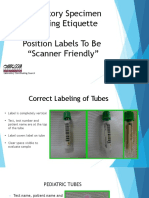
- Laboratory Specimen Labeling EtiquetteDokument42 SeitenLaboratory Specimen Labeling EtiquettefaizNoch keine Bewertungen
- Residency Program Pass Rates 2018 - 2020: What Data Are Reported?Dokument31 SeitenResidency Program Pass Rates 2018 - 2020: What Data Are Reported?yogitha dadiNoch keine Bewertungen
- Management of CareDokument3 SeitenManagement of CareKristen NateNoch keine Bewertungen
- History Comprehension Florance NightingaleDokument16 SeitenHistory Comprehension Florance NightingaleShalu 0214Noch keine Bewertungen
- BSC Staff NurseDokument4 SeitenBSC Staff NurseAnonymous gvy3mmadQNoch keine Bewertungen
- Copy of Lexico phần 2 - keyDokument73 SeitenCopy of Lexico phần 2 - keyNguyễn MyNoch keine Bewertungen
- Topik 6. Tenses ReviewDokument4 SeitenTopik 6. Tenses ReviewioakasNoch keine Bewertungen
- 1st Year Sample Paper PDFDokument4 Seiten1st Year Sample Paper PDFumar khanNoch keine Bewertungen
- Simon Decker and The Secret Formula-Jenny DooleyDokument30 SeitenSimon Decker and The Secret Formula-Jenny DooleyJorge AndrésNoch keine Bewertungen
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)