Das könnte Ihnen auch gefallen
- Myofascial Pain Dysfunction Syndrome - A RevisitDokument9 SeitenMyofascial Pain Dysfunction Syndrome - A RevisitRhea RejiNoch keine Bewertungen
- Malunions of The Distal RadiusDokument14 SeitenMalunions of The Distal RadiusSivaprasath JaganathanNoch keine Bewertungen
- HSBDokument4 SeitenHSBCarlos WebsterNoch keine Bewertungen
- Tka ValgusDokument11 SeitenTka ValgusOvidiu RusuNoch keine Bewertungen
- Ankle SprainsDokument18 SeitenAnkle Sprainsnelson1313Noch keine Bewertungen
- Gastroenterology Evaluation TemplateDokument2 SeitenGastroenterology Evaluation Templatee-MedTools88% (8)
- Foot and Ankle InjuriesDokument29 SeitenFoot and Ankle InjuriesSurgicalgownNoch keine Bewertungen
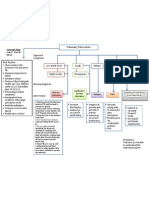
- Concept Map PTBDokument1 SeiteConcept Map PTBJoan Abardo100% (2)
- Distal Humeral Fractures-Current Concepts PDFDokument11 SeitenDistal Humeral Fractures-Current Concepts PDFRina AlvionitaNoch keine Bewertungen
- Counseling TechniquesDokument60 SeitenCounseling Techniquesdinalen0% (1)
- Aaos 2019Dokument283 SeitenAaos 2019alealer2708Noch keine Bewertungen
- Preoperative Planning For Primary Total Hip ArthroplastyDokument8 SeitenPreoperative Planning For Primary Total Hip Arthroplastyanon_683301094Noch keine Bewertungen
- Pediatric Orthopedic Trauma An Evidence-Based ApproachDokument16 SeitenPediatric Orthopedic Trauma An Evidence-Based ApproachAdam DarmawanNoch keine Bewertungen
- 2017 OITE ReviewDokument105 Seiten2017 OITE ReviewJayNoch keine Bewertungen
- Aaos TraumaDokument59 SeitenAaos Traumaidris tajouryNoch keine Bewertungen
- MPFL ReconstructionDokument16 SeitenMPFL ReconstructiondrjorgewtorresNoch keine Bewertungen
- Ortho ArticleDokument2 SeitenOrtho ArticleSamantha Dela Paz100% (1)
- Crouching Tiger Hidden Fracture - When Xray Just Ain't Enough (Comminuted Intra-Articular Fracture Distal End Humerus)Dokument5 SeitenCrouching Tiger Hidden Fracture - When Xray Just Ain't Enough (Comminuted Intra-Articular Fracture Distal End Humerus)ICNoch keine Bewertungen
- Nonoperative TreatmentDokument6 SeitenNonoperative TreatmentGorkaBuesaNoch keine Bewertungen
- Acute and Chronic Instability of The Elbow: Bernard F. Morrey, MDDokument12 SeitenAcute and Chronic Instability of The Elbow: Bernard F. Morrey, MDFadhli Aufar KasyfiNoch keine Bewertungen
- Evidence-Based Review of Distal Radius Fractures: Benjamin M. Mauck,, Colin W. SwiglerDokument12 SeitenEvidence-Based Review of Distal Radius Fractures: Benjamin M. Mauck,, Colin W. SwiglerOrtopedia HGMNoch keine Bewertungen
- Brief Resume of Intended WorkDokument7 SeitenBrief Resume of Intended WorkNavin ChandarNoch keine Bewertungen
- Tibial Eminence Fractures PDFDokument16 SeitenTibial Eminence Fractures PDFVidinikusumaNoch keine Bewertungen
- Complications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFDokument19 SeitenComplications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFSergio Tomas Cortés MoralesNoch keine Bewertungen
- Anderson and Anderson, 2011Dokument16 SeitenAnderson and Anderson, 2011Salsabila Kusuma JannatiNoch keine Bewertungen
- Handandwristinjuries: Common Problems and SolutionsDokument27 SeitenHandandwristinjuries: Common Problems and SolutionsTeja LaksanaNoch keine Bewertungen
- Ligament Balancing Medial Stabilising TechniqueDokument6 SeitenLigament Balancing Medial Stabilising TechniqueMohan DesaiNoch keine Bewertungen
- Closed Reduction and Percutaneous Kirschner Wire Fixation of Displaced Colles Fracture in AdultsDokument7 SeitenClosed Reduction and Percutaneous Kirschner Wire Fixation of Displaced Colles Fracture in AdultsnaluphmickeyNoch keine Bewertungen
- Basti As 2020Dokument17 SeitenBasti As 2020Martin MoranNoch keine Bewertungen
- Total Knee ReplacementDokument3 SeitenTotal Knee ReplacementjvshinesNoch keine Bewertungen
- Tare de TotDokument25 SeitenTare de TotantohebogdanalexNoch keine Bewertungen
- Marcheggianimuccioli 2019Dokument12 SeitenMarcheggianimuccioli 2019Ghusun MadaniNoch keine Bewertungen
- V67N1 4 PDFDokument8 SeitenV67N1 4 PDFAndrésOlivaRossiNoch keine Bewertungen
- Core Decompression in Foot and AnkleDokument9 SeitenCore Decompression in Foot and AnkleAnonymous kdBDppigENoch keine Bewertungen
- Articular Fractures of The Distal HumerusDokument9 SeitenArticular Fractures of The Distal HumerusJoha DavilaNoch keine Bewertungen
- 2002 Scarf FundaDokument9 Seiten2002 Scarf FundaRuth Aydeé SoláNoch keine Bewertungen
- Cartilage Repair of The Talus: Dirk B. Scha Fer, MDDokument11 SeitenCartilage Repair of The Talus: Dirk B. Scha Fer, MDAnonymous kdBDppigENoch keine Bewertungen
- Realignment Surgery For Malunited Ankle Fracture: Clinical ArticleDokument5 SeitenRealignment Surgery For Malunited Ankle Fracture: Clinical ArticleGio VandaNoch keine Bewertungen
- Foot Ankle Clin - 2021 Jun - 26 (2) - 391-405.Dokument15 SeitenFoot Ankle Clin - 2021 Jun - 26 (2) - 391-405.Biblioteca Centro Médico De Mar del PlataNoch keine Bewertungen
- Reversetotalshoulder Arthroplasty: Early Results of Forty-One Cases and A Review of The LiteratureDokument11 SeitenReversetotalshoulder Arthroplasty: Early Results of Forty-One Cases and A Review of The LiteratureBruno FellipeNoch keine Bewertungen
- Intertrochanteric FractureDokument9 SeitenIntertrochanteric FractureYovita Devi Kornelin100% (1)
- Intertrochanteric MEDSCAPEDokument5 SeitenIntertrochanteric MEDSCAPESpica AdharaNoch keine Bewertungen
- Scaphoid Excision and Four Corner Fusion in Treatment of Scapholunate DissociationDokument11 SeitenScaphoid Excision and Four Corner Fusion in Treatment of Scapholunate DissociationIJAR JOURNALNoch keine Bewertungen
- Distal Femoral Locking Plates For Tibiotalocalcaneal Fusions in The Charcot Ankle: A Retrospective StudyDokument6 SeitenDistal Femoral Locking Plates For Tibiotalocalcaneal Fusions in The Charcot Ankle: A Retrospective StudybaoNoch keine Bewertungen
- Thesis Umesh A2z.doc Final Thesis CorrectionDokument79 SeitenThesis Umesh A2z.doc Final Thesis CorrectionRakesh JhaNoch keine Bewertungen
- MX - Stiff ElbowDokument8 SeitenMX - Stiff ElbowPrabath ChinthakaNoch keine Bewertungen
- Hand and WristDokument85 SeitenHand and WristMohamed Abdulgader MorganNoch keine Bewertungen
- Pfirrmann VariantsPitfallsWristImaging EJR 56 2005Dokument10 SeitenPfirrmann VariantsPitfallsWristImaging EJR 56 2005Pankaj NarekarNoch keine Bewertungen
- Use of Allograft in Skeletally Immature Patients For Calcaneal Neck Lengthening OsteotomyDokument5 SeitenUse of Allograft in Skeletally Immature Patients For Calcaneal Neck Lengthening OsteotomyMonem ShakeerNoch keine Bewertungen
- Surgical Treatment of Habitual Patella Dislocation With Genu ValgumDokument3 SeitenSurgical Treatment of Habitual Patella Dislocation With Genu ValgumfitrianiNoch keine Bewertungen
- Avascular Necrosis and Related Complications Following Healed Osteoporotic Intertrochanteric FracturesDokument4 SeitenAvascular Necrosis and Related Complications Following Healed Osteoporotic Intertrochanteric FracturesNasrull BinHzNoch keine Bewertungen
- Manejo Inicial Trauma EspinalDokument7 SeitenManejo Inicial Trauma EspinalJuan MVNoch keine Bewertungen
- Intertrochanteric Hip Fractures PDFDokument9 SeitenIntertrochanteric Hip Fractures PDFSivaneasan KandiahNoch keine Bewertungen
- Minimally Invasive Transforaminal Lumbar Interbody Fusion (MI-TLIF) - A Review of Indications, Technique, Results and Complications - PMCDokument15 SeitenMinimally Invasive Transforaminal Lumbar Interbody Fusion (MI-TLIF) - A Review of Indications, Technique, Results and Complications - PMCchhabraanNoch keine Bewertungen
- Subtrochanteric Femoral Fractures:: Is A Nail or Plate Better?Dokument4 SeitenSubtrochanteric Femoral Fractures:: Is A Nail or Plate Better?luisNoch keine Bewertungen
- 6 - Injuries To The Ulnar Collateral Ligament o - 2018 - Clinical Orthopaedic Re PDFDokument4 Seiten6 - Injuries To The Ulnar Collateral Ligament o - 2018 - Clinical Orthopaedic Re PDFTolo CantallopsNoch keine Bewertungen
- Cuadricepsplastia MipiDokument5 SeitenCuadricepsplastia MipiVictor HernandezNoch keine Bewertungen
- Wagner 2021Dokument17 SeitenWagner 2021Biblioteca Centro Médico De Mar del PlataNoch keine Bewertungen
- Acl IvanDokument10 SeitenAcl IvanDINANoch keine Bewertungen
- Use of External Fixation in The Reconstruction of The Charcot Foot and AnkleDokument21 SeitenUse of External Fixation in The Reconstruction of The Charcot Foot and AnkleAnonymous kdBDppigENoch keine Bewertungen
- Artigo ClamshellDokument15 SeitenArtigo ClamshellbritocirurgiadamaoNoch keine Bewertungen
- Fingertip Injury 19Dokument5 SeitenFingertip Injury 19Mukhamad Arif MunandarNoch keine Bewertungen
- GaleazziDokument11 SeitenGaleazzijuanitiusNoch keine Bewertungen
- Anatomic Posterolateral Corner ReconstructionDokument10 SeitenAnatomic Posterolateral Corner Reconstructionethan.dumontNoch keine Bewertungen
- Cartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesVon EverandCartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesAaron J. KrychNoch keine Bewertungen
- Case ReportDokument11 SeitenCase ReportBerhanu DigamoNoch keine Bewertungen
- Internal Medicine: Dr. Nindyasari Diajeng Larasati Tim UKMPPD FKU MalahayatiDokument209 SeitenInternal Medicine: Dr. Nindyasari Diajeng Larasati Tim UKMPPD FKU MalahayatiSilvi Qiro'atul AiniNoch keine Bewertungen
- Exercise #1 10Dokument10 SeitenExercise #1 10John Paul FloresNoch keine Bewertungen
- Bioengineering Transla Med - 2022 - Chopade - Alzheimer S and Parkinson S Disease Therapies in The ClinicDokument23 SeitenBioengineering Transla Med - 2022 - Chopade - Alzheimer S and Parkinson S Disease Therapies in The ClinicurosNoch keine Bewertungen
- Skull Fracture Vs SuturesDokument6 SeitenSkull Fracture Vs Suturesmohit372Noch keine Bewertungen
- Hydatidiform MoleDokument2 SeitenHydatidiform MoleIrfan HardiNoch keine Bewertungen
- Abnormal Vaginal Bleeding Policar 051611Dokument69 SeitenAbnormal Vaginal Bleeding Policar 051611bidan22Noch keine Bewertungen
- Mandibulasr Truma ManagementDokument18 SeitenMandibulasr Truma Managementjoal510Noch keine Bewertungen
- The Apolinario Mabini Syphilis Rumors and Late 19th Century Philippine Power PlayDokument15 SeitenThe Apolinario Mabini Syphilis Rumors and Late 19th Century Philippine Power PlayHaneul KImNoch keine Bewertungen
- Energy Drinks Are Bad RealDokument4 SeitenEnergy Drinks Are Bad RealMadihi NorhadiNoch keine Bewertungen
- Tolak Angin TranslatedDokument3 SeitenTolak Angin TranslatedWadz MuharNoch keine Bewertungen
- Aneurysm: Symptoms of An AneurysmDokument3 SeitenAneurysm: Symptoms of An AneurysmArun MuralidharanNoch keine Bewertungen
- Pukpuklo A Wealth in The SeaDokument2 SeitenPukpuklo A Wealth in The SeaKrizha Angela NicolasNoch keine Bewertungen
- TORCHDokument32 SeitenTORCHJafar NoryNoch keine Bewertungen
- Systemic Diseases and The EyeDokument17 SeitenSystemic Diseases and The Eyeapi-337689057Noch keine Bewertungen
- Unit 0000 Topik 9. Word Formation: Nouns: Bold) To Nouns. Do Not Change TheDokument5 SeitenUnit 0000 Topik 9. Word Formation: Nouns: Bold) To Nouns. Do Not Change TheioakasNoch keine Bewertungen
- CortisolDokument27 SeitenCortisolCao YunNoch keine Bewertungen
- ApendikDokument4 SeitenApendikSepti AyaNoch keine Bewertungen
- HIV Drug Chart (2021)Dokument1 SeiteHIV Drug Chart (2021)savNoch keine Bewertungen
- Presentation (Final)Dokument32 SeitenPresentation (Final)Sarah Rose FeccoNoch keine Bewertungen
- Understanding The RelapseDokument12 SeitenUnderstanding The RelapseruziyanaNoch keine Bewertungen
- Arterial Blood Gas AnalysisDokument24 SeitenArterial Blood Gas AnalysisDeepika PatelNoch keine Bewertungen
- Clinical Features and Diagnosis of Abdominal Aortic Aneurysm - UpToDateDokument53 SeitenClinical Features and Diagnosis of Abdominal Aortic Aneurysm - UpToDateALVARO ARIASNoch keine Bewertungen
- Jamaophthalmology Biswas 2016 Oi 160055Dokument8 SeitenJamaophthalmology Biswas 2016 Oi 160055Ghalia HayetNoch keine Bewertungen
- The GINA 2019 Asthma Treatment Strategy For Adults and Adolescents 12... Download Scientific DiagramDokument1 SeiteThe GINA 2019 Asthma Treatment Strategy For Adults and Adolescents 12... Download Scientific DiagramFatih AryaNoch keine Bewertungen