Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Guyabano Research PaperDokument30 SeitenGuyabano Research PaperOhmyL3mmyNoch keine Bewertungen
- SCIENCE TECHNOLOGY SOCIETY Quiz 1 6 1Dokument35 SeitenSCIENCE TECHNOLOGY SOCIETY Quiz 1 6 1User Name100% (8)
- Management of Physiotherapy in Case Diabetes Mellitus Type 2 With MethodsDokument86 SeitenManagement of Physiotherapy in Case Diabetes Mellitus Type 2 With MethodsSefhia LestaryNoch keine Bewertungen
- Alkyne DiabetesDokument8 SeitenAlkyne DiabetestonoNoch keine Bewertungen
- Article WJPR 1611995787Dokument9 SeitenArticle WJPR 1611995787Sunil IndiaNoch keine Bewertungen
- Type 1 Diabetes DissertationDokument7 SeitenType 1 Diabetes DissertationPaperWriterUK100% (1)
- 17 Diagnostic Strategies For Gestational Diabetes MellitusreviewDokument10 Seiten17 Diagnostic Strategies For Gestational Diabetes MellitusreviewdianaNoch keine Bewertungen
- Nursing Care Plans: Assessment Nursing Diagnosis Planning Implementation Rationale EvaluationDokument2 SeitenNursing Care Plans: Assessment Nursing Diagnosis Planning Implementation Rationale EvaluationRheeanne Mae Amilasan100% (1)
- May Recall 2021Dokument47 SeitenMay Recall 2021school adressNoch keine Bewertungen
- Fhsis IndicatorDokument117 SeitenFhsis IndicatorTherese Mae MadroneroNoch keine Bewertungen
- Effect Al Hijama For Diabetes Type 2 PDFDokument6 SeitenEffect Al Hijama For Diabetes Type 2 PDFInyong Budiono100% (1)
- Pharmacotherapy of Diabetes Mellitus: Dr. Ave Olivia Rahman, Msc. Bagian Farmakologi Fkik UnjaDokument42 SeitenPharmacotherapy of Diabetes Mellitus: Dr. Ave Olivia Rahman, Msc. Bagian Farmakologi Fkik UnjaEya Prepti SerraNoch keine Bewertungen
- Bernardo, Ronachelle Anne G. BSN 2C Group 9: S: - Monitoring BloodDokument4 SeitenBernardo, Ronachelle Anne G. BSN 2C Group 9: S: - Monitoring Bloodwieka mawieNoch keine Bewertungen
- Iot in Healthcare: Research ReportDokument7 SeitenIot in Healthcare: Research ReportSaif-Ur -RehmanNoch keine Bewertungen
- Sample Diabetic DietDokument4 SeitenSample Diabetic DietNavya VadlamuriNoch keine Bewertungen
- Wulandari Ramadiyani 22010111110083 Lap - KTI Bab8 PDFDokument17 SeitenWulandari Ramadiyani 22010111110083 Lap - KTI Bab8 PDFZorofan Roronoa AzNoch keine Bewertungen
- Diabetes Mellitus Ada 2014 Standards of Medical Care in Diabetes Diabetes Care 1.2014Dokument67 SeitenDiabetes Mellitus Ada 2014 Standards of Medical Care in Diabetes Diabetes Care 1.2014George WinchesterNoch keine Bewertungen
- Dok 21Dokument2 SeitenDok 21dr. Noni PrisciliaNoch keine Bewertungen
- SBA Questions (No Answers)Dokument65 SeitenSBA Questions (No Answers)minayokiNoch keine Bewertungen
- Setiadi 2019 J. Phys. Conf. Ser. 1146 012009Dokument8 SeitenSetiadi 2019 J. Phys. Conf. Ser. 1146 012009Nelli Nur Indah SariNoch keine Bewertungen
- Diabetes Mellitus Aticle ApthaDokument6 SeitenDiabetes Mellitus Aticle ApthaRahul KirkNoch keine Bewertungen
- HNTR 1153 - Internet Diabetes Risk TestDokument1 SeiteHNTR 1153 - Internet Diabetes Risk TestSukmaNoch keine Bewertungen
- Research Dissemination PlanDokument5 SeitenResearch Dissemination PlanSamwel KangyNoch keine Bewertungen
- April: Application of Nursing Theory "Orem's Self-Care" Into PracticeDokument33 SeitenApril: Application of Nursing Theory "Orem's Self-Care" Into PracticeAli AlmarzoogeNoch keine Bewertungen
- Guias DIABETES CARE 2021Dokument244 SeitenGuias DIABETES CARE 2021johnbravo777Noch keine Bewertungen
- Salacia Reticulata (Kothala Himbutu) Revisited A Missed Opportunity To Treat Diabetes and Obesity?Dokument8 SeitenSalacia Reticulata (Kothala Himbutu) Revisited A Missed Opportunity To Treat Diabetes and Obesity?DEEPAK KUMARNoch keine Bewertungen
- Inpatient Pocket Card SetDokument10 SeitenInpatient Pocket Card SetMuhammad Ahmad bin makruf syammakuNoch keine Bewertungen
- RSSDI Diabetology Course ApprovedDokument6 SeitenRSSDI Diabetology Course ApprovedAsssNoch keine Bewertungen
- Functional Medicine PDF SCDokument10 SeitenFunctional Medicine PDF SCsavasthacareNoch keine Bewertungen
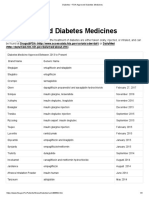
- Diabetes - FDA-Approved Diabetes MedicinesDokument3 SeitenDiabetes - FDA-Approved Diabetes MedicinesArunNoch keine Bewertungen