Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Research Vegetable SiomaiDokument23 SeitenResearch Vegetable SiomaiPas Pas93% (14)
- Barclays Money Skills Toolkit - Aged 16 - 25Dokument107 SeitenBarclays Money Skills Toolkit - Aged 16 - 25Josh BurkeNoch keine Bewertungen
- Sample - Edible Insects Market Report, 2024Dokument61 SeitenSample - Edible Insects Market Report, 2024MARIANoch keine Bewertungen
- Product PlanDokument19 SeitenProduct Planlily30109150% (2)
- Central Nervous System Tumours: Professor David Snead Uhcw Nhs TrustDokument35 SeitenCentral Nervous System Tumours: Professor David Snead Uhcw Nhs TrustJosh BurkeNoch keine Bewertungen
- Physiology of Pregnancy - Pre-Eclampsia DiabetesDokument34 SeitenPhysiology of Pregnancy - Pre-Eclampsia DiabetesJosh BurkeNoch keine Bewertungen
- Antibiotics Study Guide 2017Dokument13 SeitenAntibiotics Study Guide 2017Josh BurkeNoch keine Bewertungen
- Neck LumpDokument18 SeitenNeck LumpJosh BurkeNoch keine Bewertungen
- Block 5 Anatomy Seminar 1 Perineum MG - 5MAY2016Dokument22 SeitenBlock 5 Anatomy Seminar 1 Perineum MG - 5MAY2016Josh BurkeNoch keine Bewertungen
- IV Fluid Management: DR Andrew Stein Consultant Nephrologist, UHCWDokument37 SeitenIV Fluid Management: DR Andrew Stein Consultant Nephrologist, UHCWJosh BurkeNoch keine Bewertungen
- Joint British Diabetes Societies Inpatient Care Group - The Management of Diabetic Ketoacidosis in Adults - Pathway PosterDokument1 SeiteJoint British Diabetes Societies Inpatient Care Group - The Management of Diabetic Ketoacidosis in Adults - Pathway PosterAllison Nadine MarchandNoch keine Bewertungen
- Abdo PainDokument35 SeitenAbdo PainJosh BurkeNoch keine Bewertungen
- Physical Exam Reasons: Test Diseases Physiology Hands - NailsDokument1 SeitePhysical Exam Reasons: Test Diseases Physiology Hands - NailsJosh BurkeNoch keine Bewertungen
- Hyponatraemia QuizDokument4 SeitenHyponatraemia QuizJosh BurkeNoch keine Bewertungen
- LVSDDokument6 SeitenLVSDJosh BurkeNoch keine Bewertungen
- Blood Sugars - DiabetesDokument31 SeitenBlood Sugars - DiabetesJosh BurkeNoch keine Bewertungen
- Niel Gows Lament For The Death of His Second Wife-Mandolin-Tab PDFDokument1 SeiteNiel Gows Lament For The Death of His Second Wife-Mandolin-Tab PDFJosh BurkeNoch keine Bewertungen
- Professional Behaviour and Fitness To Practise 0816.PDF 66085925Dokument84 SeitenProfessional Behaviour and Fitness To Practise 0816.PDF 66085925Josh BurkeNoch keine Bewertungen
- R IntroDokument105 SeitenR Introtp2006sterNoch keine Bewertungen
- Adult1 16-25 - 04sep16Dokument1 SeiteAdult1 16-25 - 04sep16Josh BurkeNoch keine Bewertungen
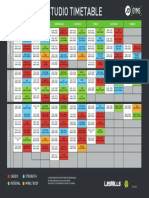
- Coventry Timetable SEP16Dokument1 SeiteCoventry Timetable SEP16Josh BurkeNoch keine Bewertungen
- PoCUS Program 1016Dokument3 SeitenPoCUS Program 1016Josh BurkeNoch keine Bewertungen
- R IntroDokument105 SeitenR Introtp2006sterNoch keine Bewertungen
- Handel HWV348 50hha - Violin1Dokument13 SeitenHandel HWV348 50hha - Violin1Josh BurkeNoch keine Bewertungen
- Anxiety and Panic Attacks: Symptoms and Risk FactorsDokument11 SeitenAnxiety and Panic Attacks: Symptoms and Risk FactorsJosh BurkeNoch keine Bewertungen
- Symptoms and Risk FactorsDokument4 SeitenSymptoms and Risk FactorsJosh BurkeNoch keine Bewertungen
- Beriot Method Part 1Dokument78 SeitenBeriot Method Part 1Caitriona HollandNoch keine Bewertungen
- Leclair 6 Sonatas Op.3 Nos 4 6Dokument25 SeitenLeclair 6 Sonatas Op.3 Nos 4 6Josh Burke100% (2)
- Bruni 6 Duettini Op.34Dokument24 SeitenBruni 6 Duettini Op.34Josh BurkeNoch keine Bewertungen
- Crockpot RecipiesDokument45 SeitenCrockpot RecipiescpantsulaNoch keine Bewertungen
- Softship SeabearDokument1 SeiteSoftship SeabearJosh BurkeNoch keine Bewertungen
- 491 Exam 1 KEYDokument10 Seiten491 Exam 1 KEYLily M Mo100% (1)
- P CLS14 Powertec Compact Leg Sled ManualDokument15 SeitenP CLS14 Powertec Compact Leg Sled ManualElizabeth GuzmanNoch keine Bewertungen
- AOE - Hiral Labs LTD Company Brochure 20180416170521Dokument20 SeitenAOE - Hiral Labs LTD Company Brochure 20180416170521Dr VENKAT1 LUNoch keine Bewertungen
- Anatomi Dan Fisiologi Mata 1Dokument61 SeitenAnatomi Dan Fisiologi Mata 1MAWANNoch keine Bewertungen
- Table Saw Safety FinalDokument24 SeitenTable Saw Safety Finalvolatileyasser100% (1)
- 00 - 7565 SigmaTherm 350Dokument3 Seiten00 - 7565 SigmaTherm 350Elcio VilanculoNoch keine Bewertungen
- ROICAM7 BookletDokument99 SeitenROICAM7 BookletPopy HalifahNoch keine Bewertungen
- 27 ASL For Teacher S BookDokument28 Seiten27 ASL For Teacher S BookNur Syazwani KhamisNoch keine Bewertungen
- Swab Contact MethodDokument7 SeitenSwab Contact Methodaca suki. haiNoch keine Bewertungen
- CPRDokument45 SeitenCPRJames Elwood DoyolaNoch keine Bewertungen
- Red Hill ComplaintDokument109 SeitenRed Hill ComplaintHonolulu Star-AdvertiserNoch keine Bewertungen
- Healing Elements of Therapeutic ConversationDokument16 SeitenHealing Elements of Therapeutic ConversationFERNANDO CABRERA SANTOSNoch keine Bewertungen
- Ethiopia - Design Gudeline Final - OromiaDokument71 SeitenEthiopia - Design Gudeline Final - OromiaEphrem Gizachew100% (15)
- Automated Sf8 ApitongDokument32 SeitenAutomated Sf8 Apitongjocelyn berlin100% (2)
- How Long To Cook A Turkey (Chart and Tips!) Taste of HomeDokument1 SeiteHow Long To Cook A Turkey (Chart and Tips!) Taste of HomefredNoch keine Bewertungen
- Coonrad Morrey ElbowDokument2 SeitenCoonrad Morrey Elbowgcif88Noch keine Bewertungen
- Routes of Drug AdministrationDokument24 SeitenRoutes of Drug Administrationmftaganas100% (1)
- Taylan Competency NeedsDokument32 SeitenTaylan Competency NeedsLovejoice Cha NnelNoch keine Bewertungen
- Travel Nurse Pdf1Dokument2 SeitenTravel Nurse Pdf1Med NetNoch keine Bewertungen
- Scientific Point of ViewDokument2 SeitenScientific Point of Viewpavans EnglishNoch keine Bewertungen
- Essay (DUNGARAN, JOHN KLENN) (BSCE-1CDokument2 SeitenEssay (DUNGARAN, JOHN KLENN) (BSCE-1CJohn KlennNoch keine Bewertungen
- Quiz BukasDokument3 SeitenQuiz BukasDYRAH GRACE COPAUSNoch keine Bewertungen
- Headache Management Guideline For Adults Version 10Dokument6 SeitenHeadache Management Guideline For Adults Version 10TomiNoch keine Bewertungen
- Rigging TechniquesDokument27 SeitenRigging TechniquesDeepak ShettyNoch keine Bewertungen
- X120MN12Dokument6 SeitenX120MN12mini p shendeNoch keine Bewertungen
- Nghe 4Dokument13 SeitenNghe 4ToánNoch keine Bewertungen
- Yaourt Foodand Health 2016Dokument10 SeitenYaourt Foodand Health 2016Patrick ParraNoch keine Bewertungen