Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Vestibular Adaptation: Recalibration, Substitution, and Alternative StrategiesDokument15 SeitenVestibular Adaptation: Recalibration, Substitution, and Alternative StrategiesCarito RivasNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Odonto Legal FinalDokument15 SeitenOdonto Legal FinalCarito RivasNoch keine Bewertungen
- APUNTE 1 Anatomia OrbitariaDokument12 SeitenAPUNTE 1 Anatomia OrbitariaCarito RivasNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Vestibular Adaptation: Recalibration, Substitution, and Alternative StrategiesDokument15 SeitenVestibular Adaptation: Recalibration, Substitution, and Alternative StrategiesCarito RivasNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Asha - BeraDokument36 SeitenAsha - BeraCarito Rivas100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- RHB CompensionDokument9 SeitenRHB CompensionCarito RivasNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Target BodybuildingDokument285 SeitenTarget Bodybuildingdlsppp88% (8)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Katame No KataDokument44 SeitenKatame No Katachristopher_kephart1100% (2)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Current Diagnosis Treatment in Rheumatology 4Th Edition John A Stone Full ChapterDokument51 SeitenCurrent Diagnosis Treatment in Rheumatology 4Th Edition John A Stone Full Chaptercindy.turner467100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Acumed Surgical Technique EN Acutrak Headless Compression Screw System SPF00 03 CDokument20 SeitenAcumed Surgical Technique EN Acutrak Headless Compression Screw System SPF00 03 CMark SharonNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Top 5 Strength Exercises For RugbyDokument4 SeitenTop 5 Strength Exercises For RugbyPaul Tinashe KatuliibaNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Course TA1 Jeffrey Okeson Management of TMDDokument6 SeitenCourse TA1 Jeffrey Okeson Management of TMDheidyNoch keine Bewertungen
- DDH - PFDokument34 SeitenDDH - PFAnnisa Oktoviani MursidaNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Intercostal SpaceDokument38 SeitenIntercostal SpaceDrravikumar BhandariNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Full Course Material Can Be Downloaded FromDokument21 SeitenFull Course Material Can Be Downloaded FromMuthu JSSCPTNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Medicina: Ffect of A Combined Stretching and StrengthDokument12 SeitenMedicina: Ffect of A Combined Stretching and StrengthKimum KimúmNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- B 1375 23 030 1 - 122100 - SRT - SMR Axioma TT Metal Back - enDokument52 SeitenB 1375 23 030 1 - 122100 - SRT - SMR Axioma TT Metal Back - enviaje68Noch keine Bewertungen
- 1914 - BAMNH033a35 - CORYTHOSAURUS CASUARIUSDokument12 Seiten1914 - BAMNH033a35 - CORYTHOSAURUS CASUARIUSKanekoNoch keine Bewertungen
- Odontoid FractureDokument40 SeitenOdontoid FractureMOHMAMMEDSNoch keine Bewertungen
- Strength For FootballDokument141 SeitenStrength For Footballkc016Noch keine Bewertungen
- Anh Van 3 - Buoi 4 - MAtchingDokument10 SeitenAnh Van 3 - Buoi 4 - MAtchingthi toNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Achilles Tendon Repair Smith Nephew Knotless TechniqueDokument8 SeitenAchilles Tendon Repair Smith Nephew Knotless TechniqueJacob DoughertyNoch keine Bewertungen
- Winged Scapula Caused by Dorsal Scapular.21Dokument4 SeitenWinged Scapula Caused by Dorsal Scapular.21emilio9fernandez9gatNoch keine Bewertungen
- Robert Oberst Creating A MonsterDokument24 SeitenRobert Oberst Creating A Monsterallenjtone85% (13)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- (P) Both Bone Forearm Fracture ORIFDokument3 Seiten(P) Both Bone Forearm Fracture ORIFkrissh20Noch keine Bewertungen
- Peng Qi Guan Ding (Qi Exchange) - Zhineng Qigong Society SingaporeDokument1 SeitePeng Qi Guan Ding (Qi Exchange) - Zhineng Qigong Society SingaporejimNoch keine Bewertungen
- Penatalaksanaan Fisioterapi Pada Kasus Low: Back Pain (LBP) Akibat Spondylosis DenganDokument12 SeitenPenatalaksanaan Fisioterapi Pada Kasus Low: Back Pain (LBP) Akibat Spondylosis Denganhafshoh lylaNoch keine Bewertungen
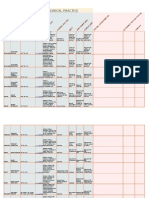
- Goniometry For Clinical PracticeDokument7 SeitenGoniometry For Clinical Practicedramitsaini33% (3)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Distosia BahuDokument48 SeitenDistosia BahuFardimayantiNoch keine Bewertungen
- The Sternomastoid "Tumor" of Infancy.Dokument12 SeitenThe Sternomastoid "Tumor" of Infancy.Dr. Ammar KhalilNoch keine Bewertungen
- BPT PDFDokument206 SeitenBPT PDFQwertNoch keine Bewertungen
- Penelitian Comparison of Musculoskeletal Disorder Risk Based On Gender in High SchoolDokument8 SeitenPenelitian Comparison of Musculoskeletal Disorder Risk Based On Gender in High SchoolAnonymous p7w1kCCtdJNoch keine Bewertungen
- Week 8 QuestionsDokument8 SeitenWeek 8 Questionsapi-479716004Noch keine Bewertungen
- Anatomia VeterináriaDokument836 SeitenAnatomia Veterináriafxmendes100% (3)
- Regional FlapsDokument55 SeitenRegional Flapsswethakari100% (1)
- Recruit The GlutesDokument9 SeitenRecruit The GlutesJoannaCamyNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)