Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- A Study On The Employee PerceptionDokument66 SeitenA Study On The Employee PerceptionRoyal Projects100% (2)
- ICO Advanced 115 MCQs 2015-2019Dokument69 SeitenICO Advanced 115 MCQs 2015-2019mrs eleven100% (1)
- Cataract and Implant Surgery: Dominic Mchugh MD Frcs London, UkDokument33 SeitenCataract and Implant Surgery: Dominic Mchugh MD Frcs London, UkVigneshNoch keine Bewertungen
- Eye MCQDokument18 SeitenEye MCQSafa Abdualrahaman Ali Hamad100% (1)
- Surgical Vs Medical Treatments For Type 2 Diabetes Mellitus A Randomized Clinical TrialDokument9 SeitenSurgical Vs Medical Treatments For Type 2 Diabetes Mellitus A Randomized Clinical TrialRofi MarhendraNoch keine Bewertungen
- Open Access Research: ObjectiveDokument13 SeitenOpen Access Research: ObjectiveRofi MarhendraNoch keine Bewertungen
- Jurnal KeratitisDokument7 SeitenJurnal KeratitisRofi MarhendraNoch keine Bewertungen
- Copy Right AgreementDokument1 SeiteCopy Right AgreementRofi MarhendraNoch keine Bewertungen
- Health 2016072214463557Dokument10 SeitenHealth 2016072214463557Rofi MarhendraNoch keine Bewertungen
- Jurnal KatarakDokument11 SeitenJurnal KatarakRofi MarhendraNoch keine Bewertungen
- DAFTAR PUSTAKA RevisiDokument3 SeitenDAFTAR PUSTAKA RevisiRofi MarhendraNoch keine Bewertungen
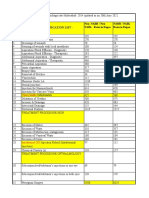
- Sr. No. Cghs Treatment Procedure/Investigation List (Patna) UPDATED ON 03.05.2021Dokument41 SeitenSr. No. Cghs Treatment Procedure/Investigation List (Patna) UPDATED ON 03.05.2021rupeshNoch keine Bewertungen
- 02 Lec 2Dokument14 Seiten02 Lec 2Mursalin SonnetNoch keine Bewertungen
- A-SME Platinum Brochure (SST) 20180901 v1Dokument64 SeitenA-SME Platinum Brochure (SST) 20180901 v1khamini dilly kannan100% (1)
- SanglahDokument13 SeitenSanglahIzzarIzzarNoch keine Bewertungen
- Extended Depth-Of-Field Intraocular LensesDokument7 SeitenExtended Depth-Of-Field Intraocular LensesAnh Nguyen DucNoch keine Bewertungen
- 200468-001 - ANTERION - ANTERION-Image-Book - EN PDFDokument13 Seiten200468-001 - ANTERION - ANTERION-Image-Book - EN PDFJulio AtencioNoch keine Bewertungen
- Tindakan Mata Icd 9 CMDokument15 SeitenTindakan Mata Icd 9 CMrekam medisNoch keine Bewertungen
- CV - Arvind GaurDokument3 SeitenCV - Arvind GaurArvind GaurNoch keine Bewertungen
- WOC2012 Scientific ProgramDokument130 SeitenWOC2012 Scientific Programpriti089Noch keine Bewertungen
- 4-Lens and CataractDokument59 Seiten4-Lens and CataractSa'adah Munawaroh HDNoch keine Bewertungen
- CHUA Website MCQs OpticsDokument45 SeitenCHUA Website MCQs Opticsdoaa naieemNoch keine Bewertungen
- Brochure - STAAR Surgical - EVO Visian ICL (Surgeon Brochure) (En)Dokument12 SeitenBrochure - STAAR Surgical - EVO Visian ICL (Surgeon Brochure) (En)Andreea L. MihalceaNoch keine Bewertungen
- 2011 Assessment of Corneal Optical QualityDokument4 Seiten2011 Assessment of Corneal Optical Qualitymoni7777Noch keine Bewertungen
- Cmeseries 28Dokument88 SeitenCmeseries 28ashishNoch keine Bewertungen
- TECNIS Synergy Spec SheetDokument2 SeitenTECNIS Synergy Spec SheetGuilherme Bender LimaNoch keine Bewertungen
- Cataracts PACESDokument2 SeitenCataracts PACESDheeshana SayakkarageNoch keine Bewertungen
- CGHS Rates - PuneDokument46 SeitenCGHS Rates - PunePrachi KhandelwalNoch keine Bewertungen
- Concept Map CATARACTDokument2 SeitenConcept Map CATARACTJrBong Semanero100% (1)
- IMA NHB Suggested Package Amount For Negotiation With Insurance CompaniesDokument5 SeitenIMA NHB Suggested Package Amount For Negotiation With Insurance Companiesmonikparmar1Noch keine Bewertungen
- Anterior VitrectomyDokument6 SeitenAnterior VitrectomyEdward Alexander Lindo RojasNoch keine Bewertungen
- Defining The Future of Monofocals.: Model: DIB00Dokument2 SeitenDefining The Future of Monofocals.: Model: DIB00jajajNoch keine Bewertungen
- CGHS Rates 2014 - HyderabadDokument60 SeitenCGHS Rates 2014 - HyderabadPradeep PaswanNoch keine Bewertungen
- Updates in Ophthalmic Anaesthesia in AdultsDokument7 SeitenUpdates in Ophthalmic Anaesthesia in AdultsJossiel OlivaresNoch keine Bewertungen
- Predisposing Factors and Surgical Outcomes of Intraocular Lens Dislocation After PhacoemulsificationDokument7 SeitenPredisposing Factors and Surgical Outcomes of Intraocular Lens Dislocation After PhacoemulsificationUmmul AzizahNoch keine Bewertungen
- Option 1 - A-Life Med Regular BrochureDokument8 SeitenOption 1 - A-Life Med Regular BrochureAIA Sunnie YapNoch keine Bewertungen
- Perfect Surgery, Unhappy Patient?Dokument1 SeitePerfect Surgery, Unhappy Patient?marco_gklothNoch keine Bewertungen