Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Senile Cataract Clinical Presentation and CausesDokument4 SeitenSenile Cataract Clinical Presentation and CausesAhmad Fahrozi100% (1)
- Prevention and Management of Glucocorticoid-Induced Side Effects: A Comprehensive ReviewDokument9 SeitenPrevention and Management of Glucocorticoid-Induced Side Effects: A Comprehensive ReviewAhmad FahroziNoch keine Bewertungen
- Polyhydramnios and Oligohydramnios - Background, Pathophysiology, EtiologyDokument4 SeitenPolyhydramnios and Oligohydramnios - Background, Pathophysiology, EtiologyAhmad FahroziNoch keine Bewertungen
- Jcdsa 2017030715443559Dokument14 SeitenJcdsa 2017030715443559Ahmad FahroziNoch keine Bewertungen
- Prevention and Management of Glucocorticoid-Induced Side Effects: A Comprehensive ReviewDokument9 SeitenPrevention and Management of Glucocorticoid-Induced Side Effects: A Comprehensive ReviewAhmad FahroziNoch keine Bewertungen
- Pasztor Norbet Thesis BookletDokument14 SeitenPasztor Norbet Thesis BookletAhmad FahroziNoch keine Bewertungen
- Oligohydramnios Imaging - Overview, WorkupDokument6 SeitenOligohydramnios Imaging - Overview, WorkupAhmad FahroziNoch keine Bewertungen
- Oligohydramnion PDFDokument6 SeitenOligohydramnion PDFhusain abdul halimNoch keine Bewertungen
- Topical Corticosteroid Misuse Among Females Attending at Dermatology Outpatient Department in Ethiopia TCOJ 1 108Dokument4 SeitenTopical Corticosteroid Misuse Among Females Attending at Dermatology Outpatient Department in Ethiopia TCOJ 1 108Ahmad FahroziNoch keine Bewertungen
- TVP 2017 0304 Column Nutrition Notes FORWEBDokument10 SeitenTVP 2017 0304 Column Nutrition Notes FORWEBAhmad FahroziNoch keine Bewertungen
- Polyhydramnios and Oligohydramnios Clinical ExamDokument2 SeitenPolyhydramnios and Oligohydramnios Clinical ExamAhmad FahroziNoch keine Bewertungen
- Dilation and Curettage: The American College of Obstetricians and GynecologistsDokument2 SeitenDilation and Curettage: The American College of Obstetricians and GynecologistsDellaNoch keine Bewertungen
- Oligohydramnion PDFDokument6 SeitenOligohydramnion PDFhusain abdul halimNoch keine Bewertungen
- Dilation and Curettage: The American College of Obstetricians and GynecologistsDokument2 SeitenDilation and Curettage: The American College of Obstetricians and GynecologistsDellaNoch keine Bewertungen
- Pregnancy Outcome Among Patients With Oligohydramnios and Suggested Plan of ActionDokument11 SeitenPregnancy Outcome Among Patients With Oligohydramnios and Suggested Plan of ActionIOSRjournalNoch keine Bewertungen
- Polyhydramnios and Oligohydramnios Medication - Prostaglandin InhibitorsDokument1 SeitePolyhydramnios and Oligohydramnios Medication - Prostaglandin InhibitorsAhmad FahroziNoch keine Bewertungen
- Polyhydramnios and Oligohydramnios Workup - Approach Considerations, Laboratory Studies, Imaging StudiesDokument3 SeitenPolyhydramnios and Oligohydramnios Workup - Approach Considerations, Laboratory Studies, Imaging StudiesAhmad Fahrozi100% (1)
- Senile Cataract (Age-Related Cataract) Medication - Mydriatics, Nonsteroidal Anti-Inflammatory Ophthalmics, Combination Ophthalmics, Corticosteroids, AntibioticsDokument4 SeitenSenile Cataract (Age-Related Cataract) Medication - Mydriatics, Nonsteroidal Anti-Inflammatory Ophthalmics, Combination Ophthalmics, Corticosteroids, AntibioticsAhmad FahroziNoch keine Bewertungen
- Senile Cataract Clinical Presentation and CausesDokument4 SeitenSenile Cataract Clinical Presentation and CausesAhmad FahroziNoch keine Bewertungen
- Senile Cataract (Age-Related Cataract) Differential Diagnoses PDFDokument1 SeiteSenile Cataract (Age-Related Cataract) Differential Diagnoses PDFAhmad FahroziNoch keine Bewertungen
- Senile Cataract (Age-Related Cataract) - Practice Essentials, Background, PathophysiologyDokument5 SeitenSenile Cataract (Age-Related Cataract) - Practice Essentials, Background, PathophysiologyAhmad FahroziNoch keine Bewertungen
- Polyhydramnios and Oligohydramnios - Background, Pathophysiology, EtiologyDokument4 SeitenPolyhydramnios and Oligohydramnios - Background, Pathophysiology, EtiologyAhmad FahroziNoch keine Bewertungen
- Senile Cataract (Age-Related Cataract) Treatment & Management - Medical Care, Surgical Care, ConsultationsDokument5 SeitenSenile Cataract (Age-Related Cataract) Treatment & Management - Medical Care, Surgical Care, ConsultationsAhmad FahroziNoch keine Bewertungen
- Senile Cataract (Age-Related Cataract) Follow-Up - Further Outpatient Care, Further Inpatient Care, Inpatient & Outpatient MedicationsDokument3 SeitenSenile Cataract (Age-Related Cataract) Follow-Up - Further Outpatient Care, Further Inpatient Care, Inpatient & Outpatient MedicationsAhmad FahroziNoch keine Bewertungen
- Senile Cataract (Age-Related Cataract) Workup - Laboratory Studies, Imaging Studies, Other TestsDokument2 SeitenSenile Cataract (Age-Related Cataract) Workup - Laboratory Studies, Imaging Studies, Other TestsAhmad FahroziNoch keine Bewertungen
- Senile Cataract (Age-Related Cataract) Differential DiagnosesDokument1 SeiteSenile Cataract (Age-Related Cataract) Differential DiagnosesAhmad FahroziNoch keine Bewertungen
- Journal Reading English and Indonesian VersionDokument24 SeitenJournal Reading English and Indonesian VersionAhmad FahroziNoch keine Bewertungen
- EngDokument66 SeitenEngAhmad FahroziNoch keine Bewertungen
- Gonorrhea - 2015 STD SurveillanceDokument4 SeitenGonorrhea - 2015 STD SurveillanceAhmad FahroziNoch keine Bewertungen
- First Announcement JSOF 5 Tahun - Revisi 3Dokument12 SeitenFirst Announcement JSOF 5 Tahun - Revisi 3Wasisto YudisaputroNoch keine Bewertungen
- Table 32-7Dokument1 SeiteTable 32-7Dragutin PetrićNoch keine Bewertungen
- Oikawa's NPD and PTSDDokument2 SeitenOikawa's NPD and PTSDDannis NgoNoch keine Bewertungen
- Hon. TA Odera, Senior Principal Magistrate (SPM)Dokument3 SeitenHon. TA Odera, Senior Principal Magistrate (SPM)dyttoNoch keine Bewertungen
- Lipo Contrast Cryo BrochureDokument5 SeitenLipo Contrast Cryo BrochureSerenity ZhangNoch keine Bewertungen
- Adenosine Therapy for Supraventricular TachycardiaDokument17 SeitenAdenosine Therapy for Supraventricular TachycardiaKirsten Padilla Chua0% (1)
- Dentigerous Cyst RadiolucencyDokument25 SeitenDentigerous Cyst RadiolucencyDr. Deepanshi SutariaNoch keine Bewertungen
- Definition, Symptoms, and Causes of NeurastheniaDokument2 SeitenDefinition, Symptoms, and Causes of NeurastheniaAlmustapha Babangida DanganiNoch keine Bewertungen
- Inj OctreotideDokument11 SeitenInj OctreotideMuhammad Azhar QureshiNoch keine Bewertungen
- Pericarditis - Morning ReportDokument51 SeitenPericarditis - Morning ReportMaria DodonNoch keine Bewertungen
- APPROACH TO MANAGING JOINT PAINDokument44 SeitenAPPROACH TO MANAGING JOINT PAINKavya Anoop100% (1)
- Neonatal JaundiceDokument12 SeitenNeonatal JaundiceGiska T PutriNoch keine Bewertungen
- Rheumatic Heart DiseaseDokument47 SeitenRheumatic Heart DiseaseGideon K. MutaiNoch keine Bewertungen
- Functional neurological disorder new subtypes and shared mechanisms - CLINICALKEY - Dr Rivas (1)Dokument14 SeitenFunctional neurological disorder new subtypes and shared mechanisms - CLINICALKEY - Dr Rivas (1)Fernando Pérez MuñozNoch keine Bewertungen
- Medical Nutrition Therapy For Diseases of The MusculoskeletalDokument55 SeitenMedical Nutrition Therapy For Diseases of The MusculoskeletalSie ningsih100% (1)
- ID Analisis Sistem Manajemen Program p2 Ispa Di Puskesmas Pegandan Kota PDFDokument10 SeitenID Analisis Sistem Manajemen Program p2 Ispa Di Puskesmas Pegandan Kota PDFFarida HanumNoch keine Bewertungen
- Endometrial CancerDokument192 SeitenEndometrial CancerAbhishek VijayakumarNoch keine Bewertungen
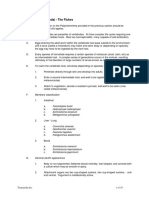
- Class Digenea (Trematoda) - The FlukesDokument10 SeitenClass Digenea (Trematoda) - The FlukesAmr EldemardashNoch keine Bewertungen
- Congenital Hip DislocationDokument6 SeitenCongenital Hip DislocationPaola CamainNoch keine Bewertungen
- Cicatricial Atelectasis - Print Friendly - STATdxDokument2 SeitenCicatricial Atelectasis - Print Friendly - STATdxmihaelaNoch keine Bewertungen
- ModuleIV RespiratoryEmergencies CHF COPD AsthmaDokument96 SeitenModuleIV RespiratoryEmergencies CHF COPD AsthmaSaiKiranNoch keine Bewertungen
- Disability Category ChartDokument4 SeitenDisability Category Chartapi-325700981100% (1)
- ECMO For COVID 19 Updated 2021 Guidelines From.98326Dokument42 SeitenECMO For COVID 19 Updated 2021 Guidelines From.98326risanataliasiburianNoch keine Bewertungen
- Celluar and Neural Regulation StudentDokument52 SeitenCelluar and Neural Regulation StudentCruz YrNoch keine Bewertungen
- Ob NCP 2Dokument2 SeitenOb NCP 2Kimberly Mondala (SHS)Noch keine Bewertungen
- DUPUYTREN'S SYNDROME TestDokument15 SeitenDUPUYTREN'S SYNDROME TestreyNoch keine Bewertungen
- Genetic Disorders SourcebookDokument748 SeitenGenetic Disorders Sourcebookpaconscribd100% (1)
- Ayurvedic Diabetes CureDokument13 SeitenAyurvedic Diabetes CureYassine KrineNoch keine Bewertungen
- Multiple Organ Failure As A Cause of DeaDokument6 SeitenMultiple Organ Failure As A Cause of DeaEliza DiaconescuNoch keine Bewertungen
- Analisis Metode Certainty Factor Pada Sistem Pakar Diagnosa Penyakit THTDokument6 SeitenAnalisis Metode Certainty Factor Pada Sistem Pakar Diagnosa Penyakit THTryuzen000Noch keine Bewertungen