Das könnte Ihnen auch gefallen
- The Trigeminal and Facial NervesDokument7 SeitenThe Trigeminal and Facial NervesJose CastroNoch keine Bewertungen
- The Trigeminal and Facial NervesDokument7 SeitenThe Trigeminal and Facial NervesJose CastroNoch keine Bewertungen
- Koskas 2013Dokument15 SeitenKoskas 2013Okta Kurniawan SaputraNoch keine Bewertungen
- Ce 15403Dokument18 SeitenCe 15403Dita Wahyu RahmanNoch keine Bewertungen
- Cranial Nerves V, Ix, X, XiDokument89 SeitenCranial Nerves V, Ix, X, XiUloko Christopher100% (1)
- Trigeminal NerveDokument11 SeitenTrigeminal Nervekio josephNoch keine Bewertungen
- Patel BellPalsy 01Dokument7 SeitenPatel BellPalsy 01ubayyumrNoch keine Bewertungen
- Anatomy AssignmentDokument10 SeitenAnatomy AssignmentObansa JohnNoch keine Bewertungen
- Examen Neurologico en BovinosDokument8 SeitenExamen Neurologico en BovinosAlejandra AriasNoch keine Bewertungen
- Nerve Suply To Head and NeckDokument22 SeitenNerve Suply To Head and NeckrajtanniruNoch keine Bewertungen
- Nervo FacialeDokument15 SeitenNervo FacialeAndrea PescosolidoNoch keine Bewertungen
- Anatomy of The Facial NerveDokument75 SeitenAnatomy of The Facial NerveRao Rizwan Shakoor100% (1)
- Nervio Trigemino Articulo 2019Dokument8 SeitenNervio Trigemino Articulo 2019Wendy Alejandra NarvaezNoch keine Bewertungen
- Brainstem: Francisco E. Olucha BordonauDokument22 SeitenBrainstem: Francisco E. Olucha BordonauJean Pierre Chastre LuzaNoch keine Bewertungen
- Cranial NervesDokument30 SeitenCranial NervesNia RwNoch keine Bewertungen
- Bell's Palsy: Aetiology, Clinical Features and Multidisciplinary CareDokument8 SeitenBell's Palsy: Aetiology, Clinical Features and Multidisciplinary CareMarsya Yulinesia LoppiesNoch keine Bewertungen
- BIO-201L Lab 13: PNS and Cranial NervesDokument4 SeitenBIO-201L Lab 13: PNS and Cranial NervesdfgvsfdsfNoch keine Bewertungen
- Key Points:: Questions For StudentsDokument19 SeitenKey Points:: Questions For Studentssimi yNoch keine Bewertungen
- BellsPalsy JNNP 2015Dokument8 SeitenBellsPalsy JNNP 2015Marsya Yulinesia LoppiesNoch keine Bewertungen
- Bells PalsyDokument6 SeitenBells PalsyPhub TsheringNoch keine Bewertungen
- Draw It To Know It NotesDokument13 SeitenDraw It To Know It Noteskat9210Noch keine Bewertungen
- Anatomy of Trigeminal NerveDokument39 SeitenAnatomy of Trigeminal NerveBharath Kumar Uppuluri100% (1)
- 1 s2.0 S2211568413002052 MainDokument7 Seiten1 s2.0 S2211568413002052 MaindoraNoch keine Bewertungen
- Topognosis of Facial Nerve LesionsDokument11 SeitenTopognosis of Facial Nerve LesionsAudiologiaNoch keine Bewertungen
- Cranial Nerves. - Sensory Organs - General MedicineDokument100 SeitenCranial Nerves. - Sensory Organs - General MedicineHamdi AlaqalNoch keine Bewertungen
- The Nervus IntermediusDokument5 SeitenThe Nervus IntermediusDr. AtheerNoch keine Bewertungen
- Pares 2Dokument50 SeitenPares 2api-3701995Noch keine Bewertungen
- Circir Uk 20 88 3 370-376Dokument7 SeitenCircir Uk 20 88 3 370-376Lens AquosNoch keine Bewertungen
- Abducent Nerve 6CNDokument2 SeitenAbducent Nerve 6CNkio josephNoch keine Bewertungen
- Anatomy of The Facial NerveDokument75 SeitenAnatomy of The Facial NerveSerene Batra100% (2)
- Cranial NervesDokument7 SeitenCranial NerveshamnahrjunaidNoch keine Bewertungen
- 1 My Trigeminal NerveDokument23 Seiten1 My Trigeminal NerveDan 04Noch keine Bewertungen
- Surgical Anatomy Facial NerveDokument4 SeitenSurgical Anatomy Facial NervedominicdefNoch keine Bewertungen
- Cranial Nerves Summary PDFDokument9 SeitenCranial Nerves Summary PDFMudassar SattarNoch keine Bewertungen
- Mrcpsych Paper 2 Revision Neurosciences Answers & Lecture Notes May 2010Dokument74 SeitenMrcpsych Paper 2 Revision Neurosciences Answers & Lecture Notes May 2010Naeem KhanNoch keine Bewertungen
- The Vestibulocochlear Nerve VIII 2013 Diagnostic and Interventional ImaginDokument8 SeitenThe Vestibulocochlear Nerve VIII 2013 Diagnostic and Interventional ImaginCristinna ANoch keine Bewertungen
- J Clinph 2005 04 020Dokument11 SeitenJ Clinph 2005 04 020Andres Rojas JerezNoch keine Bewertungen
- Cranial NervesDokument118 SeitenCranial NervesGan'sNoch keine Bewertungen
- Disorders of The Lower Cranial Nerves: Review ArticleDokument15 SeitenDisorders of The Lower Cranial Nerves: Review Articleamelia marhelesNoch keine Bewertungen
- NeuroradiologyCurrent and Future Imaging of The Peripheral NervoussystemDokument10 SeitenNeuroradiologyCurrent and Future Imaging of The Peripheral NervoussystemRyanNoch keine Bewertungen
- CVA Case ReportDokument76 SeitenCVA Case ReportpaulaNoch keine Bewertungen
- Facial Nerve Disroders and OtalgiaDokument39 SeitenFacial Nerve Disroders and Otalgiaياسر كوثر هانيNoch keine Bewertungen
- A Rare Case of Optic Nerve Schwannoma: Case Report and Review of The LiteratureDokument5 SeitenA Rare Case of Optic Nerve Schwannoma: Case Report and Review of The LiteratureloversockfulNoch keine Bewertungen
- Facial Nerve PalsyDokument3 SeitenFacial Nerve PalsySusan BensonNoch keine Bewertungen
- Facial NerveDokument128 SeitenFacial NervevaneetNoch keine Bewertungen
- The Functional Anatomy of The Cranial NervesDokument29 SeitenThe Functional Anatomy of The Cranial NervesRăzvan Moțoc100% (1)
- L18 Cranial NervesDokument2 SeitenL18 Cranial NervesmoshlingmomoNoch keine Bewertungen
- X ANATOMY HEAD AND NECKDokument16 SeitenX ANATOMY HEAD AND NECKArijeet77Noch keine Bewertungen
- Facial ParalysisDokument59 SeitenFacial ParalysisSUnil Kumar100% (1)
- Bloqueio de Nervos Cranianos para Tratamento Da CefaleiaDokument13 SeitenBloqueio de Nervos Cranianos para Tratamento Da CefaleiarflschalcherNoch keine Bewertungen
- Cranial NerveDokument39 SeitenCranial NerveСуджива Гунасинха100% (2)
- Trigeminal NerveDokument92 SeitenTrigeminal Nervemounika33% (3)
- Cranial Nerve Disorders: Ernest E. WangDokument13 SeitenCranial Nerve Disorders: Ernest E. Wangirsyad tsaniNoch keine Bewertungen
- 1 Trigeminal Neuralgia An Overview From Pathophysiology To Pharmacological TreatmentDokument18 Seiten1 Trigeminal Neuralgia An Overview From Pathophysiology To Pharmacological TreatmentGabriela Elizabeth Gomez CardenasNoch keine Bewertungen
- Cranial NervesDokument67 SeitenCranial NervesBahaa ShaabanNoch keine Bewertungen
- Trigeminal NerveDokument12 SeitenTrigeminal NerveTabata SantanaNoch keine Bewertungen
- Neuroscience Essay - Cranial NervesDokument3 SeitenNeuroscience Essay - Cranial NervesAkshaya RajangamNoch keine Bewertungen
- 6th Lecture - Physiology of The Brain Stem - CNS PhysiologyDokument13 Seiten6th Lecture - Physiology of The Brain Stem - CNS PhysiologyAnastasia SoareNoch keine Bewertungen
- Adekunle Seminar in Cranial NervDokument34 SeitenAdekunle Seminar in Cranial NervBamgbose OpeyemiNoch keine Bewertungen
- JurnalDokument120 SeitenJurnalIman PradanaNoch keine Bewertungen
- Embolization of Epistaxis and Juvenile Nasopharyngeal AngiofibromasDokument10 SeitenEmbolization of Epistaxis and Juvenile Nasopharyngeal AngiofibromasIman PradanaNoch keine Bewertungen
- An Exploration OF Feeding Difficulties in Children With DownDokument14 SeitenAn Exploration OF Feeding Difficulties in Children With DownIman PradanaNoch keine Bewertungen
- Review: Inhaled Corticosteroids and GrowthDokument10 SeitenReview: Inhaled Corticosteroids and GrowthIman PradanaNoch keine Bewertungen
- Efficacy and Safety of Mometasone Furoate Nasal Spray in Allergic Rhinitis Acute Rhinosinusitis and Nasal Polyposis PDFDokument14 SeitenEfficacy and Safety of Mometasone Furoate Nasal Spray in Allergic Rhinitis Acute Rhinosinusitis and Nasal Polyposis PDFIman PradanaNoch keine Bewertungen
- Adolescence: Physical and Cognitive Development: Development Across The LifespanDokument46 SeitenAdolescence: Physical and Cognitive Development: Development Across The LifespanChhaya RathodNoch keine Bewertungen
- For Success N Access 1022168537 - DBVE8685Dokument10 SeitenFor Success N Access 1022168537 - DBVE8685vanam tejasviNoch keine Bewertungen
- Bone Marrow Aspiration ThesisDokument5 SeitenBone Marrow Aspiration Thesisfjf1y2rz100% (1)
- Ehlers-Danlos Panel: ExpertDokument17 SeitenEhlers-Danlos Panel: ExpertMalika ButtNoch keine Bewertungen
- Questions ENT 2021Dokument28 SeitenQuestions ENT 2021Ranjan Prasad100% (1)
- Protein QuantificationDokument60 SeitenProtein Quantificationkiedd_0491% (11)
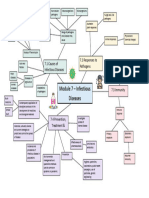
- Module 7 Mind Map BiologyDokument1 SeiteModule 7 Mind Map BiologyAltSpace TimeNoch keine Bewertungen
- Icici Lombard Complete Health Insurance Proposal FormDokument4 SeitenIcici Lombard Complete Health Insurance Proposal FormMonal RajNoch keine Bewertungen
- Lepy 103Dokument19 SeitenLepy 103Syed FerozNoch keine Bewertungen
- New Language Leader Intermediate Unit 9 KeyDokument7 SeitenNew Language Leader Intermediate Unit 9 KeyHa TranNoch keine Bewertungen
- J Jacc 2023 01 049 PDFDokument25 SeitenJ Jacc 2023 01 049 PDFRaquel AguilarNoch keine Bewertungen
- Acute PancreatitisDokument3 SeitenAcute PancreatitisZeynep YılmaztürkNoch keine Bewertungen
- Evidence For A Connection Between Coronavirus Disease 19 and ExposureDokument16 SeitenEvidence For A Connection Between Coronavirus Disease 19 and ExposureJamile XavierNoch keine Bewertungen
- AD01.ALL Forms New StudentDokument10 SeitenAD01.ALL Forms New StudentAdeline Elpedia GarciaNoch keine Bewertungen
- Booklet On Covid-19 Vaccines: Luisa Fernanda Londoño Cadavid Mariana Restrepo Londoño Fernando Mejia QuinteroDokument3 SeitenBooklet On Covid-19 Vaccines: Luisa Fernanda Londoño Cadavid Mariana Restrepo Londoño Fernando Mejia QuinteroMariana RestrepoNoch keine Bewertungen
- Quiz Sheet - 2: Test Center Log in Home PageDokument11 SeitenQuiz Sheet - 2: Test Center Log in Home PageJignasha VadiNoch keine Bewertungen
- Nursing Assessment in Family Nursing PracticeDokument22 SeitenNursing Assessment in Family Nursing PracticeHydra Olivar - PantilganNoch keine Bewertungen
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationDokument10 SeitenAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationJobelle AcenaNoch keine Bewertungen
- AMOS Revision PaedsDokument2 SeitenAMOS Revision PaedsDeborah AnneNoch keine Bewertungen
- Special Stains in Histopathology: Movat'S Pentachrome StainDokument27 SeitenSpecial Stains in Histopathology: Movat'S Pentachrome StainambadepravinNoch keine Bewertungen
- GRADE 4 Module W2Dokument2 SeitenGRADE 4 Module W2Gerald Pante ValenzuelaNoch keine Bewertungen
- Reading Sub-Test: Part ADokument17 SeitenReading Sub-Test: Part AVijayalakshmi Narayanaswami78% (9)
- Parasitology:: Classification of ParasitesDokument17 SeitenParasitology:: Classification of ParasitesIrfan Pathan KakarNoch keine Bewertungen
- Reflections On Aphantasia: SciencedirectDokument2 SeitenReflections On Aphantasia: SciencedirectJORGE ENRIQUE CAICEDO GONZ�LESNoch keine Bewertungen
- Acute Respiratory Distress SyndromeDokument30 SeitenAcute Respiratory Distress SyndromeOya Zuraini KamalNoch keine Bewertungen
- Gastrointestinal Drugs HandoutDokument3 SeitenGastrointestinal Drugs Handoutcriselda desistoNoch keine Bewertungen
- Current Concept For Management of Neuropathic PainDokument55 SeitenCurrent Concept For Management of Neuropathic Painmpm8471Noch keine Bewertungen
- Speci C Protein Analysis System: DiagnosticsDokument2 SeitenSpeci C Protein Analysis System: DiagnosticsAniket dubeyNoch keine Bewertungen
- PSM Volume 2 (2015) PDFDokument219 SeitenPSM Volume 2 (2015) PDFLeo GyiNoch keine Bewertungen
- Republic of The Philippines Samar State University Catbalogan, CityDokument23 SeitenRepublic of The Philippines Samar State University Catbalogan, CityChe SkaNoch keine Bewertungen
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (30)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Von EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Bewertung: 3 von 5 Sternen3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (404)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 4 von 5 Sternen4/5 (4)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 5 von 5 Sternen5/5 (81)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsVon EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsBewertung: 4.5 von 5 Sternen4.5/5 (170)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 4 von 5 Sternen4/5 (5)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisVon EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisBewertung: 5 von 5 Sternen5/5 (8)
- Empath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainVon EverandEmpath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainBewertung: 4 von 5 Sternen4/5 (95)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeVon EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeBewertung: 4.5 von 5 Sternen4.5/5 (253)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessVon EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessBewertung: 4.5 von 5 Sternen4.5/5 (328)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedBewertung: 4 von 5 Sternen4/5 (61)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- The Marshmallow Test: Mastering Self-ControlVon EverandThe Marshmallow Test: Mastering Self-ControlBewertung: 4.5 von 5 Sternen4.5/5 (59)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesVon EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesBewertung: 4.5 von 5 Sternen4.5/5 (1412)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryVon EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryBewertung: 4 von 5 Sternen4/5 (45)