Das könnte Ihnen auch gefallen
- ERCP Radiology Basics 2003Dokument6 SeitenERCP Radiology Basics 2003Alistair KohNoch keine Bewertungen
- Linear Energy Transfer and Relative Biological Effectiveness Investigation of Various Structures For A Cohort of Proton Patients With Brain TumorsDokument12 SeitenLinear Energy Transfer and Relative Biological Effectiveness Investigation of Various Structures For A Cohort of Proton Patients With Brain TumorsRaul Matute MartinNoch keine Bewertungen
- Review of The Most Common Pre-Processing Techniques For Near-Infrared SpectraDokument22 SeitenReview of The Most Common Pre-Processing Techniques For Near-Infrared SpectraHaesoo LeeNoch keine Bewertungen
- (2019) Time-Resolved Dosimetry of Pulsed Electron Beams in Very High Dose Rate FLASH Irradiaiton For Radiotherapy Preclinical LstudiesDokument11 Seiten(2019) Time-Resolved Dosimetry of Pulsed Electron Beams in Very High Dose Rate FLASH Irradiaiton For Radiotherapy Preclinical LstudiesJames RenaudNoch keine Bewertungen
- Advantages and Disadvantages of Luminescence DosimetryDokument6 SeitenAdvantages and Disadvantages of Luminescence DosimetrySUBHANoch keine Bewertungen
- In Vitro Microemboli Classification Using Neural Network Models and RF SignalsDokument6 SeitenIn Vitro Microemboli Classification Using Neural Network Models and RF SignalstalebNoch keine Bewertungen
- Barth, 2007Dokument29 SeitenBarth, 2007Marco Aurelio OliveiraNoch keine Bewertungen
- E 387 - 84 R95 - Rtm4ny04nfi5nuuxDokument10 SeitenE 387 - 84 R95 - Rtm4ny04nfi5nuuxpechugonisNoch keine Bewertungen
- Esplen 2022 Phys. Med. Biol. 67 105003Dokument25 SeitenEsplen 2022 Phys. Med. Biol. 67 105003souhaila soulNoch keine Bewertungen
- Friedman 2009Dokument11 SeitenFriedman 2009Allan Amaral da HoraNoch keine Bewertungen
- Spektro Raman USP 40Dokument9 SeitenSpektro Raman USP 40Kelas BNoch keine Bewertungen
- Spectrochimica Acta Part A: Molecular and Biomolecular SpectrosDokument7 SeitenSpectrochimica Acta Part A: Molecular and Biomolecular SpectrosJose Filipe Bacalhau RodriguesNoch keine Bewertungen
- Intercomparación DetectoresDokument5 SeitenIntercomparación DetectoresvictorNoch keine Bewertungen
- F 358 - 83 R02 - Rjm1oaDokument4 SeitenF 358 - 83 R02 - Rjm1oajayakumarNoch keine Bewertungen
- SafariDokument8 SeitenSafariman gobinda chowdhuryNoch keine Bewertungen
- FTIR Technical PaperDokument24 SeitenFTIR Technical PaperBalqis yasinNoch keine Bewertungen
- MP 15442Dokument14 SeitenMP 15442Hanna AnwarNoch keine Bewertungen
- Review of GaN-based Devices For Terahertz Operation Review of GaN-based Devices For Terahertz Operation by Kiarash AhiDokument15 SeitenReview of GaN-based Devices For Terahertz Operation Review of GaN-based Devices For Terahertz Operation by Kiarash AhiFancy LinNoch keine Bewertungen
- Ir 56 705Dokument21 SeitenIr 56 705MSNoch keine Bewertungen
- 10.1002@mrc.5095 - NMR of All AcetineDokument16 Seiten10.1002@mrc.5095 - NMR of All AcetineresearchNoch keine Bewertungen
- E 2059 - 00 - RtiwntkDokument20 SeitenE 2059 - 00 - RtiwntkPrakash MakadiaNoch keine Bewertungen
- An 906Dokument24 SeitenAn 906KamenriderNoch keine Bewertungen
- JRPR 41 4 339Dokument5 SeitenJRPR 41 4 339brandonzhen02Noch keine Bewertungen
- Mahuvava C Et Al. (2022)Dokument13 SeitenMahuvava C Et Al. (2022)Courage MahuvavaNoch keine Bewertungen
- Raman Spectroscopy DissertationDokument4 SeitenRaman Spectroscopy DissertationCheapPaperWritingServicesOmaha100% (1)
- Carlino 2018 End-To-End Tests Ry in Scanned Proton BeamsDokument17 SeitenCarlino 2018 End-To-End Tests Ry in Scanned Proton BeamsKanit TanthanawigraiNoch keine Bewertungen
- Medical Physics - 2021 - Lee - Medical X Band Linear Accelerator For High Precision RadiotherapyDokument16 SeitenMedical Physics - 2021 - Lee - Medical X Band Linear Accelerator For High Precision RadiotherapyNima SalianiNoch keine Bewertungen
- AIP Pros and Cons of LF MRIDokument10 SeitenAIP Pros and Cons of LF MRIStanislav VyrvaNoch keine Bewertungen
- Optical Emission Spectroscopy As An Analytical ToolDokument27 SeitenOptical Emission Spectroscopy As An Analytical ToolJayee NonickNoch keine Bewertungen
- E387-04 (2014) Standard Test Method For Estimating Stray Radiant Power Ratio of Dispersive Spectrophotometers by The Opaque Filter MethodDokument11 SeitenE387-04 (2014) Standard Test Method For Estimating Stray Radiant Power Ratio of Dispersive Spectrophotometers by The Opaque Filter Methodislamaktham100% (2)
- Pellegrini 1993 0352Dokument5 SeitenPellegrini 1993 0352Particle Beam Physics LabNoch keine Bewertungen
- Krauss 2010-LC-high Resolution MS in Environmental Analysis - From Target Screening To The Identification of UnknownsDokument9 SeitenKrauss 2010-LC-high Resolution MS in Environmental Analysis - From Target Screening To The Identification of UnknownsyenNoch keine Bewertungen
- 2.application of The Double Relaxation Oscillation Superconducting Quantum InterferenceDokument10 Seiten2.application of The Double Relaxation Oscillation Superconducting Quantum InterferenceΘοδωρής ΣτρατόπουλοςNoch keine Bewertungen
- Closed-Loop Atomic Force Microscopy-Infrared Spectroscopic Imaging For Nanoscale Molecular CharacterizationDokument10 SeitenClosed-Loop Atomic Force Microscopy-Infrared Spectroscopic Imaging For Nanoscale Molecular CharacterizationMedo MedicNoch keine Bewertungen
- Gamma Factors For XRAYDokument8 SeitenGamma Factors For XRAYcindy anggrilitaNoch keine Bewertungen
- Radiation OncDokument15 SeitenRadiation OncMihreta MustaficNoch keine Bewertungen
- Radiation Physics and Chemistry: M. Santibáñez, M. Vásquez, R.G. Figueroa, M. ValenteDokument7 SeitenRadiation Physics and Chemistry: M. Santibáñez, M. Vásquez, R.G. Figueroa, M. ValenteEdson Batista De Oliveira JuniorNoch keine Bewertungen
- Applications For Mid-IR Spectroscopy in The Pharmaceutical Process EnvironmentDokument4 SeitenApplications For Mid-IR Spectroscopy in The Pharmaceutical Process EnvironmentberkahNoch keine Bewertungen
- X-Ray Fluorescence Analysis of Polymers: A White Paper From Spectro Analytical InstrumentsDokument13 SeitenX-Ray Fluorescence Analysis of Polymers: A White Paper From Spectro Analytical Instruments475976550Noch keine Bewertungen
- Photo Accoustic ImagineDokument7 SeitenPhoto Accoustic ImagineArpan MannaNoch keine Bewertungen
- Signal-To-Noise Ratio in Direct-Detection Mid-Infrared Random-Modulation Continuous-Wave Lidar in The Presence of Colored Additive NoiseDokument14 SeitenSignal-To-Noise Ratio in Direct-Detection Mid-Infrared Random-Modulation Continuous-Wave Lidar in The Presence of Colored Additive NoiseFrontiersNoch keine Bewertungen
- Nima 56240Dokument6 SeitenNima 56240maghrabismNoch keine Bewertungen
- Optik 23Dokument14 SeitenOptik 23z.umul9031Noch keine Bewertungen
- Pha052 TG 9Dokument14 SeitenPha052 TG 9Alcea InguilloNoch keine Bewertungen
- Transport of Intensity Equation A TutorialDokument98 SeitenTransport of Intensity Equation A TutorialdgNoch keine Bewertungen
- Sum Signal Dosimetry: A New Approach For High Dose Quality Assurance With Gafchromic EBT3Dokument10 SeitenSum Signal Dosimetry: A New Approach For High Dose Quality Assurance With Gafchromic EBT3Kurbonali KhujaevNoch keine Bewertungen
- Qi2018 Article InvestigationOfTheRadiosensitiDokument8 SeitenQi2018 Article InvestigationOfTheRadiosensitiJohnnie LópezNoch keine Bewertungen
- Spectroscopy: For Grape and Wine AnalysisDokument9 SeitenSpectroscopy: For Grape and Wine AnalysisSandraNoch keine Bewertungen
- Excitation Spectra and Brightness Optimization of Two-Photon Excited ProbesDokument11 SeitenExcitation Spectra and Brightness Optimization of Two-Photon Excited ProbesCLPHtheoryNoch keine Bewertungen
- Maintaining Image Quality While Reducing Acoustic Noise and Switched GradientDokument11 SeitenMaintaining Image Quality While Reducing Acoustic Noise and Switched GradientArsy ZygomaticNoch keine Bewertungen
- RV 5146Dokument16 SeitenRV 5146Mr.WasgehtsiedasanNoch keine Bewertungen
- Excitation of Plasmonic Waves in Graphene by Guided-Mode ResonancesDokument8 SeitenExcitation of Plasmonic Waves in Graphene by Guided-Mode ResonancesHabibe DurmazNoch keine Bewertungen
- Broadband Picometer-Scale Resolution On-Chip Spectrometer With Reconfigurable PhotonicsDokument10 SeitenBroadband Picometer-Scale Resolution On-Chip Spectrometer With Reconfigurable PhotonicsarashmokhtariNoch keine Bewertungen
- Slow Light Nanocoatings For Ultrashort Pulse Compression: ArticleDokument7 SeitenSlow Light Nanocoatings For Ultrashort Pulse Compression: ArticleEfimov AlexeyNoch keine Bewertungen
- Zhao-2007-Automated Autofluorescence Background Subtraction Algorithm For Biomedical Raman SpectrosDokument8 SeitenZhao-2007-Automated Autofluorescence Background Subtraction Algorithm For Biomedical Raman SpectrosWiJan CheungNoch keine Bewertungen
- NMR OptimizacijaDokument7 SeitenNMR OptimizacijaEdi TopićNoch keine Bewertungen
- Measurement of Nanoparticles by Light-Scattering Techniques: Satinder K. Brar, M. VermaDokument14 SeitenMeasurement of Nanoparticles by Light-Scattering Techniques: Satinder K. Brar, M. VermaGhimis Simona BiancaNoch keine Bewertungen
- Ir Spectroscopy 2021 SkoogDokument48 SeitenIr Spectroscopy 2021 SkoogAlan MathewNoch keine Bewertungen
- Infrared Spectroscopy A Tool For Determination ofDokument5 SeitenInfrared Spectroscopy A Tool For Determination ofIsma WatiNoch keine Bewertungen
- Infrared and Raman Spectroscopy: Principles and Spectral InterpretationVon EverandInfrared and Raman Spectroscopy: Principles and Spectral InterpretationBewertung: 3 von 5 Sternen3/5 (1)
- LogarithmicDokument1 SeiteLogarithmicVictorM.LópezGuadalupeNoch keine Bewertungen
- Radiotherapy of Advanced Mycosis Fungoides PDFDokument6 SeitenRadiotherapy of Advanced Mycosis Fungoides PDFVictorM.LópezGuadalupeNoch keine Bewertungen
- Self Organization and Entropy Reduction in Living CellDokument21 SeitenSelf Organization and Entropy Reduction in Living CellVictorM.LópezGuadalupeNoch keine Bewertungen
- The Use of Monte Carlo Technique To Optimize The Dose Distribution in Total Skin IrradiationDokument2 SeitenThe Use of Monte Carlo Technique To Optimize The Dose Distribution in Total Skin IrradiationVictorM.LópezGuadalupeNoch keine Bewertungen
- The Use of Monte Carlo Technique To Optimize The Dose Distribution in Total Skin IrradiationDokument2 SeitenThe Use of Monte Carlo Technique To Optimize The Dose Distribution in Total Skin IrradiationVictorM.LópezGuadalupeNoch keine Bewertungen
- Acute Toxicity and Risk of Infection During Total Skin Electron Beam Therapy For Mycosis FungoidesDokument7 SeitenAcute Toxicity and Risk of Infection During Total Skin Electron Beam Therapy For Mycosis FungoidesVictorM.LópezGuadalupeNoch keine Bewertungen
- Experience With Total Skin Electron Beam Therapy in Combination With ExtracorporealDokument7 SeitenExperience With Total Skin Electron Beam Therapy in Combination With ExtracorporealVictorM.LópezGuadalupeNoch keine Bewertungen
- The UK Primary Standard Calorimeter For Photon Beam Absorbed Dose MeasurmentDokument15 SeitenThe UK Primary Standard Calorimeter For Photon Beam Absorbed Dose MeasurmentVictorM.LópezGuadalupeNoch keine Bewertungen
- Energy Depos HCPDokument18 SeitenEnergy Depos HCPVictorM.LópezGuadalupeNoch keine Bewertungen
- Electron Beam Total Skin Irradiation PDFDokument1 SeiteElectron Beam Total Skin Irradiation PDFVictorM.LópezGuadalupeNoch keine Bewertungen
- Experience With Total Skin Electron Beam Therapy in Combination With ExtracorporealDokument7 SeitenExperience With Total Skin Electron Beam Therapy in Combination With ExtracorporealVictorM.LópezGuadalupeNoch keine Bewertungen
- Absorbed DoseDokument13 SeitenAbsorbed DoseRio RadNoch keine Bewertungen
- Levi-Civita SymbolDokument4 SeitenLevi-Civita SymbolarslanpasaNoch keine Bewertungen
- Electron Beams Clinical AspectsDokument24 SeitenElectron Beams Clinical AspectsVictorM.LópezGuadalupeNoch keine Bewertungen
- Determination of Calibration Factors in Terms of Air Kerma and Absorbed Dose To Water in The 60co Gamma RaysDokument11 SeitenDetermination of Calibration Factors in Terms of Air Kerma and Absorbed Dose To Water in The 60co Gamma RaysVictorM.LópezGuadalupeNoch keine Bewertungen
- Beam Configuration and Physical Parameters of Clinical High Energy Photon Beam For Total Body IrradiationDokument6 SeitenBeam Configuration and Physical Parameters of Clinical High Energy Photon Beam For Total Body IrradiationVictorM.LópezGuadalupeNoch keine Bewertungen
- Water Calorimetry The Heat Defect.Dokument12 SeitenWater Calorimetry The Heat Defect.VictorM.LópezGuadalupeNoch keine Bewertungen
- (Pruitt Et Al 1981) The Graphite Calorimeter As A Standard of Absorbed Dose For Cobalt 60 Gamma RadiationDokument8 Seiten(Pruitt Et Al 1981) The Graphite Calorimeter As A Standard of Absorbed Dose For Cobalt 60 Gamma RadiationVictorM.LópezGuadalupeNoch keine Bewertungen
- Liang Fu Et Al - Majorana Fermions in Topological InsulatorsDokument14 SeitenLiang Fu Et Al - Majorana Fermions in Topological InsulatorsPo48HSDNoch keine Bewertungen
- Ptolemy and Copernicus and FinalDokument2 SeitenPtolemy and Copernicus and FinalLance BassettNoch keine Bewertungen
- Qada Qadar Dan Parallel UniverseDokument14 SeitenQada Qadar Dan Parallel Universeambiya086114Noch keine Bewertungen
- Koutandos 23Dokument4 SeitenKoutandos 23Κουταντου ΕφηNoch keine Bewertungen
- Experiment 5 (Physics)Dokument3 SeitenExperiment 5 (Physics)Christopher PaladioNoch keine Bewertungen
- Formulas and Reference Chart EocDokument3 SeitenFormulas and Reference Chart Eocapi-87739323Noch keine Bewertungen
- 21041.heat Transfer Thermal Management of ElectronicsDokument526 Seiten21041.heat Transfer Thermal Management of ElectronicsAli Adnan100% (3)
- B4 - Engenharia Térmica (Thermal Engineering), Vol. 14 - No. 2 - December 2015 - P. 43-46Dokument4 SeitenB4 - Engenharia Térmica (Thermal Engineering), Vol. 14 - No. 2 - December 2015 - P. 43-46pstrobelNoch keine Bewertungen
- The First Century of Chemical EngineeringDokument6 SeitenThe First Century of Chemical EngineeringFredericoNoch keine Bewertungen
- Rubber Mixing SimulationDokument147 SeitenRubber Mixing Simulationalperen52100% (2)
- 1 Year Study Plan For IIT JEE MainDokument9 Seiten1 Year Study Plan For IIT JEE MainShubham kumar100% (1)
- Schweiger-The Role of Advanced Constitutive Models in Geotechnical EngineeringDokument9 SeitenSchweiger-The Role of Advanced Constitutive Models in Geotechnical EngineeringRuben RubiñosNoch keine Bewertungen
- Which Drill Pipe Is The Less Resistant To Buckling Steel, Aluminum or Titanium Drill PipeDokument11 SeitenWhich Drill Pipe Is The Less Resistant To Buckling Steel, Aluminum or Titanium Drill PipeMejbahul SarkerNoch keine Bewertungen
- SSS 1 3RD TermDokument21 SeitenSSS 1 3RD TermabiodunokoyaNoch keine Bewertungen
- CS407 Neural Computation: Neural Networks For Constrained Optimization. Lecturer: A/Prof. M. BennamounDokument51 SeitenCS407 Neural Computation: Neural Networks For Constrained Optimization. Lecturer: A/Prof. M. Bennamounanant_nimkar9243Noch keine Bewertungen
- Meteodyn Complex Terrain Modeling CFD Software Bolund Hill Round Robin TestDokument18 SeitenMeteodyn Complex Terrain Modeling CFD Software Bolund Hill Round Robin TestMeteodyn_UrbawindNoch keine Bewertungen
- A Closed Form Ula For The Riemann Normal Coordinate ExpansionDokument10 SeitenA Closed Form Ula For The Riemann Normal Coordinate ExpansionGabriel GomezNoch keine Bewertungen
- 1 PDFDokument126 Seiten1 PDFSalvador Arcos100% (1)
- What Is Buoyancy?: Archimedes' PrincipleDokument1 SeiteWhat Is Buoyancy?: Archimedes' PrincipleYelchuri Kumar PhanindraNoch keine Bewertungen
- Tutorial Sheet 10Dokument2 SeitenTutorial Sheet 10dineshazm83Noch keine Bewertungen
- Unit h556 01 Modelling Physics Sample Assessment MaterialsDokument48 SeitenUnit h556 01 Modelling Physics Sample Assessment MaterialsY4NISMTNoch keine Bewertungen
- CF 23Dokument25 SeitenCF 23赵子杰Noch keine Bewertungen
- 5 1doneDokument3 Seiten5 1doneeperlaNoch keine Bewertungen
- YCEF Presentaion-Derivation of Wind LoadingDokument57 SeitenYCEF Presentaion-Derivation of Wind LoadingVictor OmotoriogunNoch keine Bewertungen
- Shimizu, S. (2020) - Formulating Rationally Via Statistical Thermodynamics. Curr. Opin. Colloid Interface Sci. 48, 53-64Dokument12 SeitenShimizu, S. (2020) - Formulating Rationally Via Statistical Thermodynamics. Curr. Opin. Colloid Interface Sci. 48, 53-64marco_ravelo_10Noch keine Bewertungen
- Acceleration vs. Time GraphDokument16 SeitenAcceleration vs. Time Graphlea pagusaraNoch keine Bewertungen
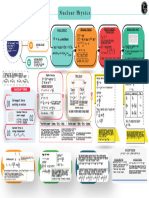
- Nuclear Physics - Mind Map - Lakshya NEET 2024Dokument1 SeiteNuclear Physics - Mind Map - Lakshya NEET 2024aanyakaurchonaNoch keine Bewertungen
- OML751 Testing of MaterialsDokument39 SeitenOML751 Testing of MaterialsVikashini GNoch keine Bewertungen
- AAA - Stability - Lecture - SummaryDokument146 SeitenAAA - Stability - Lecture - SummaryIvan EstradaNoch keine Bewertungen
- Karmaveer Bhaurao Patil College Vashi, Navi Mumbai Autonomous CollegeDokument21 SeitenKarmaveer Bhaurao Patil College Vashi, Navi Mumbai Autonomous Collegemathers maddyNoch keine Bewertungen