Das könnte Ihnen auch gefallen
- Ati RN Nursing Care of Children Proctored Exam 2 RN Ati Nursing Care of Children Proctored ExDokument11 SeitenAti RN Nursing Care of Children Proctored Exam 2 RN Ati Nursing Care of Children Proctored ExPesh B NimmoNoch keine Bewertungen
- Mood Disorder QuestionsDokument4 SeitenMood Disorder QuestionsMackenzie Lehman0% (1)
- Pharmacology 2 Final Exam 2021-NkDokument16 SeitenPharmacology 2 Final Exam 2021-NkT'amo HanashNoch keine Bewertungen
- Test Questions From Barbara K. TimbyDokument5 SeitenTest Questions From Barbara K. Timbysuperrhengc0% (1)
- 2015 PM Lecture 4 Barium EnemaDokument62 Seiten2015 PM Lecture 4 Barium EnemaObrian ReidNoch keine Bewertungen
- P.E. and HealthDokument9 SeitenP.E. and Healthriza sibullasNoch keine Bewertungen
- April 1999 Paper 1 Clinical Nursing Essay - Type Test Items: Scenario 1 Item 1Dokument10 SeitenApril 1999 Paper 1 Clinical Nursing Essay - Type Test Items: Scenario 1 Item 1Aaron WallaceNoch keine Bewertungen
- Angina ManagementDokument14 SeitenAngina ManagementAaron WallaceNoch keine Bewertungen
- Gastro Key NotesDokument11 SeitenGastro Key NotesHannah aswini100% (1)
- D. NegligenceDokument11 SeitenD. NegligenceKing GeorgeNoch keine Bewertungen
- October 1997 Paper 1 Clinical Nursing Essay - Type Test ItemsDokument2 SeitenOctober 1997 Paper 1 Clinical Nursing Essay - Type Test ItemsTkNoch keine Bewertungen
- Burns: TEST I - Foundation of Professional Nursing PracticeDokument9 SeitenBurns: TEST I - Foundation of Professional Nursing PracticeMc SuanNoch keine Bewertungen
- G3 IAH and ACSDokument29 SeitenG3 IAH and ACSRoshin Mae E. TejeroNoch keine Bewertungen
- NCLEX Exam: Maternal and Child Health Nursing 2 (30 Items)Dokument8 SeitenNCLEX Exam: Maternal and Child Health Nursing 2 (30 Items)Karen Mae Santiago AlcantaraNoch keine Bewertungen
- Practice Nursing Test With Answers and RationaleDokument23 SeitenPractice Nursing Test With Answers and RationaleNorjetalexis CabreraNoch keine Bewertungen
- Please Prepare For Maternal Final Review by Answering The Following 50 QuestionsDokument12 SeitenPlease Prepare For Maternal Final Review by Answering The Following 50 QuestionsPanJan BalNoch keine Bewertungen
- Medical-Surg NursingDokument9 SeitenMedical-Surg Nursingأبوأحمد الحكيمNoch keine Bewertungen
- Influenza VirusDokument17 SeitenInfluenza Virusapi-458845511Noch keine Bewertungen
- Ob ExamDokument5 SeitenOb ExamShermeen Ann SanPedro BartolomeNoch keine Bewertungen
- 100Dokument48 Seiten100Jerome JucutanNoch keine Bewertungen
- Evolve Key Points and Questions For Test 2 Maternal Child CareDokument104 SeitenEvolve Key Points and Questions For Test 2 Maternal Child CareHeather100% (2)
- 2012 Practice Final Exam 2Dokument5 Seiten2012 Practice Final Exam 2rkwaughNoch keine Bewertungen
- Lippincott's REPRODUCTIVE PROBLEMSDokument14 SeitenLippincott's REPRODUCTIVE PROBLEMSNursyNurseNoch keine Bewertungen
- ZRN 13 Mental Health MockDokument14 SeitenZRN 13 Mental Health MockFan EliNoch keine Bewertungen
- Chapter 22 - Transition To ParenthoodDokument16 SeitenChapter 22 - Transition To ParenthoodJill HillNoch keine Bewertungen
- Political Action in NursingDokument66 SeitenPolitical Action in NursingDocRNNoch keine Bewertungen
- Practice Exam For Nursing NLE BLENDokument14 SeitenPractice Exam For Nursing NLE BLENLeizel ApolonioNoch keine Bewertungen
- Chapter 012Dokument15 SeitenChapter 012Karunakar100% (1)
- Fundamentals of Nursing QuizDokument7 SeitenFundamentals of Nursing QuizmiokitzNoch keine Bewertungen
- University of Luzon College of Nursing Ns-Ii2 P Oxygenation ProblemsDokument10 SeitenUniversity of Luzon College of Nursing Ns-Ii2 P Oxygenation ProblemsAhmad BaolayyanNoch keine Bewertungen
- Community Acquired Pneumonia CAP 1.28.21Dokument1 SeiteCommunity Acquired Pneumonia CAP 1.28.21Illaizah EdictoNoch keine Bewertungen
- Ob Review QuestionsDokument31 SeitenOb Review QuestionsRandyNoch keine Bewertungen
- Features FNCP:: Health Nursing ProblemsDokument12 SeitenFeatures FNCP:: Health Nursing Problemsrodeliza100% (2)
- Health Promotion Test QuestionsDokument5 SeitenHealth Promotion Test QuestionsAyesha khanNoch keine Bewertungen
- N120 Final Review PDFDokument7 SeitenN120 Final Review PDFsutopianoNoch keine Bewertungen
- Answer Key Midwifery 1 Final Term ExaminationDokument6 SeitenAnswer Key Midwifery 1 Final Term Examinationgladz25Noch keine Bewertungen
- Renal AnatomyDokument17 SeitenRenal AnatomyMuhammad Tauseef BashirNoch keine Bewertungen
- Chronic GlomerulonephritisDokument18 SeitenChronic GlomerulonephritisMarithe Joi Abarico AberosNoch keine Bewertungen
- CA CardiovascularDokument10 SeitenCA CardiovascularNina OaipNoch keine Bewertungen
- Medical Surgical QuizDokument12 SeitenMedical Surgical QuizLyka DimayacyacNoch keine Bewertungen
- Learning Objective: - Explain of Acute AbdomenDokument143 SeitenLearning Objective: - Explain of Acute AbdomenSamuel Sebastian SirapanjiNoch keine Bewertungen
- Teamworks! Game: Summary ReportDokument2 SeitenTeamworks! Game: Summary ReportAngela May Pustasa AllamNoch keine Bewertungen
- Urinary System DisordersDokument14 SeitenUrinary System DisordersGideon P. CasasNoch keine Bewertungen
- Nursing Q and A (Volume 2)Dokument7 SeitenNursing Q and A (Volume 2)Rem Yriz100% (1)
- E1 Fall 20Dokument10 SeitenE1 Fall 20Alexander BarbechoNoch keine Bewertungen
- Newborn CompetencyDokument3 SeitenNewborn CompetencyJem Tellain100% (1)
- تجميع اخير .-محول كااااااملDokument135 Seitenتجميع اخير .-محول كااااااملmanar ahmedNoch keine Bewertungen
- Pregnancy Induced Hypertension Case StudyDokument77 SeitenPregnancy Induced Hypertension Case StudyATEHAN BORDS100% (1)
- Dry Swabs: Diascan StripsDokument5 SeitenDry Swabs: Diascan StripsAaron WallaceNoch keine Bewertungen
- Which Activities Are The Circulating NurseDokument12 SeitenWhich Activities Are The Circulating NurseDENNIS N. MUÑOZNoch keine Bewertungen
- Positioning, SNLE KSADokument30 SeitenPositioning, SNLE KSAmarketing.ruhNoch keine Bewertungen
- Nutrition Study Guide - NursingDokument3 SeitenNutrition Study Guide - NursingKaren HutchinsonNoch keine Bewertungen
- Clinical ExemplarDokument5 SeitenClinical Exemplarapi-252750576Noch keine Bewertungen
- MCN Sample QuestionsDokument24 SeitenMCN Sample QuestionsADATO, Alaiza Mae S.Noch keine Bewertungen
- Antepartum 2Dokument3 SeitenAntepartum 2Emily Davis100% (2)
- NCLEX Addition QuestionDokument5 SeitenNCLEX Addition QuestionwildestbeeNoch keine Bewertungen
- Obstetric Nursing Care PlanDokument12 SeitenObstetric Nursing Care PlanfiercesheNoch keine Bewertungen
- Nclex-Pn Chapter 21 BwfinalDokument12 SeitenNclex-Pn Chapter 21 BwfinalatmojdNoch keine Bewertungen
- Nursing Practice IIIDokument34 SeitenNursing Practice IIIbeautifulme031690Noch keine Bewertungen
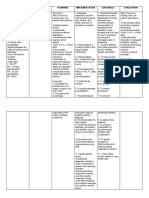
- Assessment Nursing Diagnosis Planning Implementation Rationale Evaluation Subjective DataDokument2 SeitenAssessment Nursing Diagnosis Planning Implementation Rationale Evaluation Subjective DataCheila CruzNoch keine Bewertungen
- Breathing PatternDokument4 SeitenBreathing PatternVince John SevillaNoch keine Bewertungen
- Mood Disorders: C. Baker-Burke MSCN, BSCN, RNDokument39 SeitenMood Disorders: C. Baker-Burke MSCN, BSCN, RNObrian ReidNoch keine Bewertungen
- Assess The Contributions Made To Popular Culture in The Region by The Following PersonsDokument7 SeitenAssess The Contributions Made To Popular Culture in The Region by The Following PersonsObrian Reid100% (1)
- Factors That Promote or Hinder DevelopmentDokument3 SeitenFactors That Promote or Hinder DevelopmentObrian ReidNoch keine Bewertungen
- FC2 M2022apccp044 Q3Dokument3 SeitenFC2 M2022apccp044 Q319BPS147 Shravanthi PadmanabanNoch keine Bewertungen
- Funda NotesDokument55 SeitenFunda NotesKristine CastilloNoch keine Bewertungen
- Chronic ConfusionDokument7 SeitenChronic Confusionners_gunNoch keine Bewertungen
- Apharmac Nice OneDokument113 SeitenApharmac Nice OneSupriyoGhoshNoch keine Bewertungen
- Candito 6 Week ProgramDokument16 SeitenCandito 6 Week ProgramSyed ArbabNoch keine Bewertungen
- At The Gym: Lingua House Lingua HouseDokument4 SeitenAt The Gym: Lingua House Lingua HousediogofffNoch keine Bewertungen
- Sandbag 101 SampleDokument11 SeitenSandbag 101 Samplebarna284Noch keine Bewertungen
- Build BeginnerDokument14 SeitenBuild BeginnerBurcu SenolNoch keine Bewertungen
- CORE PE and Health Module 1Dokument3 SeitenCORE PE and Health Module 1Princess CunananNoch keine Bewertungen
- BMR, DBW, Sda, BmiDokument37 SeitenBMR, DBW, Sda, BmiSarte Rachelle AnneNoch keine Bewertungen
- Basic Yoga ExercisesDokument30 SeitenBasic Yoga ExercisesCatherine FadriquelanNoch keine Bewertungen
- P.E. Module 1-Converted (1) - Converted - 3333Dokument6 SeitenP.E. Module 1-Converted (1) - Converted - 3333Minnhela Gwen MarcosNoch keine Bewertungen
- Insanity WorksheetDokument1 SeiteInsanity WorksheetShuvajoyyyNoch keine Bewertungen
- Januari 2020Dokument15 SeitenJanuari 2020Andira AzzahraNoch keine Bewertungen
- First Beat: GarminDokument23 SeitenFirst Beat: GarminJeeEianYannNoch keine Bewertungen
- Modern Concept of Child CareDokument209 SeitenModern Concept of Child CareSadhu PriyankaNoch keine Bewertungen
- The Educational Benefits of Videogames: Mark GriffithsDokument5 SeitenThe Educational Benefits of Videogames: Mark GriffithsAngelo ChaustreNoch keine Bewertungen
- Introduction To Unit 6 You May ScoffDokument8 SeitenIntroduction To Unit 6 You May Scoffmoli84736Noch keine Bewertungen
- Nutrition Care Plan - Febrile Client With Hepatitis ADokument3 SeitenNutrition Care Plan - Febrile Client With Hepatitis AElaine ArsagaNoch keine Bewertungen
- Norma Portuguesa NP 37 de 2009Dokument10 SeitenNorma Portuguesa NP 37 de 2009aspereiraNoch keine Bewertungen
- Orem Self Care DeficitDokument59 SeitenOrem Self Care DeficitAndy TolentinoNoch keine Bewertungen
- 0849370655Dokument450 Seiten0849370655Luisa LopezNoch keine Bewertungen
- DEFENDED (Charot)Dokument43 SeitenDEFENDED (Charot)Carmela DiazNoch keine Bewertungen
- Insanity CalendarDokument4 SeitenInsanity CalendarMaks “Karas Nur Li” FedorovNoch keine Bewertungen
- Weight ManagementDokument50 SeitenWeight Managementzia ullahNoch keine Bewertungen
- FD Buttbible 2018 EbookDokument155 SeitenFD Buttbible 2018 EbookIsabel SeabraNoch keine Bewertungen
- Culinary Nutrition ProgramsDokument11 SeitenCulinary Nutrition ProgramsMalbido, Ela T.Noch keine Bewertungen
- Atomy IndiaDokument4 SeitenAtomy IndiamaheshNoch keine Bewertungen
- Healthy LifeDokument15 SeitenHealthy Lifeenle chenNoch keine Bewertungen