Beruflich Dokumente
Kultur Dokumente
Imaging Pulmonary Infection: Classic Signs and Patterns
Hochgeladen von
Christ'na De RedArmyOriginaltitel
Copyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
Imaging Pulmonary Infection: Classic Signs and Patterns
Hochgeladen von
Christ'na De RedArmyCopyright:
Verfügbare Formate
Cardiopulmonar y Imaging Review
FOCUS ON:
Imaging Pulmonary Infection:
Classic Signs and Patterns
Christopher M. Walker1 OBJECTIVE. The purposes of this article are to describe common and uncommon imag-
Gerald F. Abbott1 ing signs and patterns of pulmonary infections and to discuss their underlying anatomic and
Reginald E. Greene1 pathophysiologic basis.
Jo-Anne O. Shepard1 CONCLUSION. Imaging plays an integral role in the diagnosis and management of sus-
Dharshan Vummidi2 pected pulmonary infections and may reveal useful signs on chest radiographs and CT scans.
Detected early, these signs can often be used to predict the causative agent and pathophysi-
Subba R. Digumarthy1
ologic mechanism and possibly to optimize patient care.
American Journal of Roentgenology 2014.202:479-492.
P
ulmonary infections are among the Consolidation and Air
most common infections encoun- Bronchogram Sign
tered in outpatient and inpatient Consolidation is an alveolar-filling process
clinical care. According to the that replaces air within the affected airspac-
Centers for Disease Control and Prevention, in- es, increasing in pulmonary attenuation and
fluenza and pneumonia were combined as the obscuring the margins of adjacent airways
eighth leading cause of death in the United and vessels on radiographs and CT scans [2].
States in 2011 [1]. Imaging studies are critical Consolidation is one of the more common
for the diagnosis and management of pulmo- manifestations of pulmonary infection, and
nary infections. When the imaging manifes- its appearance is variable, dependent on the
tations of a known disease entity form a consis- causative organism.
tent pattern or characteristic appearance, those Air-filled bronchi may become visible when
manifestations may be regarded as an imaging surrounded by dense, consolidated lung paren-
sign of that disease. Imaging signs by them- chyma and may produce the air bronchogram
selves are sometimes nonspecific and may also sign (Fig. 1), initially described by Felix Fleischner
Keywords: abscess, fungus, infection, signs be manifestations of noninfectious diseases. in 1948 [3, 4]. In normal lung, air-filled bron-
Various imaging signs of thoracic infection can chi are not apparent on chest radiographs be-
DOI:10.2214/AJR.13.11463
be clinically useful, sometimes suggesting a cause they are surrounded by aerated lung pa-
Received June 26, 2013; accepted after revision specific diagnosis and often narrowing the dif- renchyma. In a patient with fever and cough,
August 16, 2013. ferential diagnosis. Clinical data, such as WBC this sign suggests the diagnosis of pneumonia.
1
count, results of microbiologic tests, and im- Though the sign is most commonly seen with
Department of Radiology, Thoracic Imaging Division,
mune status, should be correlated with the im- bacterial infection, any infection can manifest
Massachusetts General Hospital, 55 Fruit St, Boston,
MA 02114. Address correspondence to C. M. Walker aging sign and any additional findings to facili- the air bronchogram sign. Differential diag-
(walk0060@gmail.com). tate an accurate diagnosis. The objectives of nostic considerations include nonobstructive
this article are to discuss common and uncom- atelectasis, aspiration, and neoplasms, such as
2
Department of Radiology, University of Michigan, mon signs and findings of pulmonary infection adenocarcinoma and lymphoma. One can dif-
Ann Arbor, MI.
at radiography and CT, discuss the mechanisms ferentiate atelectasis from pneumonia by look-
This article is available for credit. and pathophysiologic factors that produce those ing for direct and indirect signs of volume loss,
findings, and highlight several noninfectious including bronchovascular crowding, fissural
AJR 2014; 202:479492 diseases that may present with similar findings. displacement, mediastinal shift, and diaphrag-
0361803X/14/2023479
This review is divided into signs that are most matic elevation. Detection of the air broncho-
commonly seen or associated with bac- terial, gram sign argues against the presence of a cen-
American Roentgen Ray Society viral, fungal, and parasitic infections. tral obstructing lesion.
AJR:202, March 2014 479
Walker et al.
Silhouette Sign (e.g., cystic fibrosis or immune deficiency), come to be recognized as a potential mani-
The silhouette sign was initially described diffuse panbronchiolitis, and adenocarcino- festation of other conditions, including me-
by Felson as a radiographic sign that enabled ma [11]. Aspiration generally results in de- tastasis, arteriovenous fistula, and pulmonary
the anatomic localization of abnormalities on pendent tree-in-bud opacities predominat- vasculitis [23]. Septic emboli should be con-
orthogonal chest radiographs [5]. The ing in the lower lung zones. Cystic fibrosis sidered when the feeding vessel sign is seen
silhouette sign describes loss of a normal should be considered when upper-lung-zone with cavitating and noncavitating nodules
lungsoft-tissue interface (loss of silhouette) predominant bronchiectasis, bronchial wall and subpleural wedge-shaped consolidation.
caused by any pathologic mechanism that re- thickening, mucus plugging, and mosaic at- The nodules usually have basal and peripher-
places or displaces air within the lung pa- tenuation are seen in combination with tree- al predominance and vary in size [24]. Arte-
renchyma. The silhouette sign is produced on in-bud opacities. Diffuse panbronchiolitis riovenous fistula is differentiated from septic
chest radiographs when the loss of inter- face should be considered when diffuse and uni- emboli by the finding not only of a feeding
occurs between structures in the same form tree-in-bud opacities are seen in a pa- artery but also of an enlarged draining vein.
anatomic plane within an image. This sign is tient of East Asian descent. Less commonly,
commonly applied to the interface between the tree-in-bud sign may be a manifestation Inhomogeneous Enhancement
the lungs and the heart, mediastinum, chest of vascular lesions (so-called vascular tree- Sign and Cavitation
wall, and diaphragm. Consolidation that ex- in-bud), including embolized tumor or for- In a patient with pneumonia, the CT de-
tends to the border of an adjacent soft-tissue eign material, due to the anatomic location of tection of inhomogeneous enhancement and
structure will obliterate its interface with that small arterioles as paired homologous struc- cavitation suggests the presence of necro-
structure [5]. For example, lingular pneumo- tures that course alongside the small airways tizing infection [25, 26]. Pulmonary necro-
nia obscures the left-heart border, and mid- in the centrilobular aspect of the secondary sis may become evident as hypoenhancing
dle lobe pneumonia obscures the right-heart pulmonary lobules [8, 1215] (Fig. 4). geographic areas of low lung attenuation that
American Journal of Roentgenology 2014.202:479-492.
border, because the areas of consolidation may be difficult to differentiate from ad-
and the respective heart borders are in the Bulging Fissure Sign jacent pleural fluid [25] (Fig. 7). This find-
same anatomic plane (Fig. 2). Conversely, The bulging fissure sign represents expan- ing is often seen before frank abscess forma-
with lower lobe pneumonia, the heart bor- der sive lobar consolidation causing fissural tion and is a predictor of a prolonged hospital
is preserved, but the ipsilateral hemidia- bulging or displacement by copious amounts course [26]. A cavity is defined as abnormal
phragm is frequently obscured (silhouetted). of inflammatory exudate within the affected lucency within an area of consolidation with
It is important to consider a diagnosis of bac- parenchyma. Classically associated with right or without an associated air-fluid level. Cav-
terial pneumonia in a patient with fever and upper lobe consolidation due to Klebsiella itation may be the result of suppurative or
cough when the silhouette sign is detected at pneumoniae (Fig. 5), any form of pneumonia caseous necrosis or lung infarction. Impor-
chest radiography. Other diseases that can can manifest the bulging fissure sign. The tantly, cavitation does not always indicate
manifest the silhouette sign include atelecta- sign is frequently seen in patients with pneu- a lung infection or abscess. Cavitation can
sis (segmental or lobar), aspiration, pleural mococcal pneumonia [16, 17]. The prevalence have noninfectious causes, including malig-
effusion, and tumor [5]. of this sign is decreasing, likely because of nancy, radiation therapy, and lung infarction
prompt administration of antibiotic therapy to [2]. Suppurative necrosis usually occurs with
Tree-in-Bud Sign patients with suspected pneumonia [18]. The infection by Staphylococcus aureus, gram-
The small airways or terminal bronchioles bulging fissure sign is also less com- monly negative bacteria, or anaerobes. Caseous ne-
are invisible on CT images because of their detected in patients with hospital-ac- quired crosis is a characteristic histologic feature of
small size (< 2 mm) and thin walls (< 0.1 Klebsiella pneumonia than in those with mycobacterial infection, but cavitation is a
mm). They may become indirectly visible on community-acquired Klebsiella infec- tion common pathologic and imaging feature of
CT images when filled with mucus, pus, flu- [19]. Other diseases that manifest a bulging angioinvasive fungal infections, such as as-
id, or cells, forming impactions that resemble fissure include any space-occupying process pergillosis and mucormycosis.
a budding tree with branching nodular V- and in the lung, such as pulmonary hem- orrhage,
Y-shaped opacities that are referred to as the lung abscess, and tumor. Air-Fluid Level Sign
tree-in-bud sign [69] (Fig. 3). Because tree- In a patient with pneumonia, detection of
in-bud opacities form in the center of the sec- Feeding Vessel Sign an air-fluid level on chest radiographs or CT
ondary pulmonary lobule, they characteristi- The feeding vessel sign is the CT find- ing images suggests the presence of a lung ab-
cally spare the subpleural lung parenchyma, of a pulmonary vessel coursing to a dis- tal scess or empyema with bronchopleural fis-
including that adjacent to interlobar fissures. pulmonary nodule or mass. This sign was tula. The former typically requires medi- cal
Although initially thought to be diagnos- tic originally thought to indicate hematogenous treatment with antibiotics, and the latter
of mycobacterial infection, the tree-in- bud dissemination of disease [20, 21], but when it usually requires insertion of a chest tube for
sign may be an imaging manifestation of was studied on multiplanar reformatted drainage. Lung abscess is most commonly
various infections caused by bacteria, fungi, images, most of the so-called feeding ves- associated with aspiration pneumonia and
parasites, and viruses [6, 8, 10]. Tree-in-bud sels were actually pulmonary veins coursing septic pulmonary emboli. Common causative
opacities usually indicate infectious bron- from the nodule, and the pulmonary arteries organisms include anaerobes, Staphylococcus
chiolitis or aspiration but are less common- usually coursed around the nodule [22]. The aureus, and Klebsiella pneumoniae. Lung ab-
ly seen in other conditions, such as follicular feeding vessel sign was initially considered scess is associated with increased morbidity
bronchiolitis, chronic airways inflammation diagnostic of septic emboli (Fig. 6) but has and mortality. Prompt detection at imaging
480 AJR:202, March 2014
Imaging Pulmonary Infection
studies may improve patient care, enabling nant effusions (Fig. 10), hemothorax, and se- Air Crescent or Monad Sign
clinicians to treat patients with an appropri- quelae of previous talc pleurodesis, lobecto- of Mycetoma
ate course of antibiotic therapy [27]. my, or pneumonectomy. Hemothorax usually The air crescent sign of mycetoma, also re-
Detection of an air-fluid level at chest radi- has associated heterogeneously high attenua- ferred to as the Monad sign, is seen in an im-
ography should prompt evaluation of its loca- tion, and talc pleurodesis has attenuation sim- munocompetent host with preexisting cystic
tion as being in the lung parenchyma or with- ilar to that of calcium and is often clumped. or cavitary lung disease, usually from tuber-
in the pleural space. A lung abscess with an culosis or sarcoidosis [42]. The fungal ball or
air-fluid level can be differentiated from em- Halo Sign mycetoma develops within a preexisting lung
pyema with bronchopleural fistula by mea- The halo sign is the CT finding of a periph- cavity and may exhibit gravity dependence
surement and comparison of the lengths of eral rim of ground-glass opacity surrounding (Fig. 14). The mycetoma is composed of fun-
the visualized air-fluid level on orthogonal a pulmonary nodule or mass [2, 32]. When gal hyphae, mucus, and cellular debris. My-
chest radiographs. Because of the charac- detected in a febrile patient with neutrope- cetomas can cause hemoptysis. The treatment
teristic spherical shape of a lung abscess, an nia, this sign is highly suggestive of angio- options include surgical resection, bronchial
associated air-fluid level typically has equal invasive Aspergillus infection [3234] (Fig. artery embolization, and instillation of anti-
lengths on posteroanterior and lateral chest 11). The ground-glass opacity represents fungal agents into the cavity [40]. The air cres-
radiographs (Fig. 8). By contrast, empyema hemorrhage surrounding infarcted lung and is cent sign is not specific for Aspergillus infec-
typically forms lenticular collections of pleu- caused by vascular invasion by the fungus tion and can be seen in other conditions, such
ral fluid, and an associated air-fluid level [35]. The halo sign is typically seen early in as cavitating neoplasm, intracavitary clot, and
(e.g., bronchopleural fistula) usually exhibits the course of the infection. In a group of 25 Wegener granulomatosis [2, 43, 44].
length disparity when compared on postero- patients with invasive Aspergillus infection,
anterior and lateral chest radiographs. In ad- the halo sign was seen in 24 patients on day 0 Finger-in-Glove Sign
The finger-in-glove sign is the chest radio-
American Journal of Roentgenology 2014.202:479-492.
dition, both entities typically display a differ- and was detected in only 19% of patients by
ence in the angle of their interface with an day 14, highlighting the importance of per- graphic finding of tubular and branching tubu-
adjacent pleural surface. A lung abscess usu- forming CT early in the course of a suspect- lar opacities that appear to emanate from the
ally forms an acute angle when it intersects ed fungal infection [36]. In a large group of hila, said to resemble gloved fingers [45, 46].
with an adjacent pleural surface, and its wall immunocompromised patients with Asper- The tubular opacities represent dilated bronchi
is often thick and irregular. By contrast, em- gillus infection, Greene and colleagues [37] impacted with mucus. The CT finger-in-glove
pyema typically forms obtuse angles along its found that patients in whom the halo sign was sign is branching endobronchial opacities that
interface with adjacent pleura and usu- ally visualized at CT had improved surviv- al and course alongside neighboring pulmonary ar-
has smooth, thin, enhancing walls [28, 29]. response to antifungal treatment com- pared teries. The finding is classically associated
Other differential diagnostic consider- ations with those without the halo sign at CT. with allergic bronchopulmonary aspergillosis
for an intrathoracic air-fluid level in- clude Differential considerations for the halo sign (ABPA), seen in persons with asthma and pa-
hemorrhage into a cavity, lung cancer, and include other infections, such as mucormy- tients with cystic fibrosis (Fig. 15), but may
metastatic disease. cosis and Candida (Fig. 12), Pseudomonas, also occur as an imaging manifestation of en-
herpes simplex virus, and cytomegalovirus dobronchial tumor (Fig. 16), bronchial atresia,
Split-Pleura Sign infections, and other causes, such as Wegen- cystic fibrosis, and postinflammatory bronchi-
Normal visceral and parietal pleura are in- er granulomatosis, hemorrhagic metastasis, ectasis [4547]. Bronchoscopy may be nec-
distinguishable on CT images. In the presence and Kaposi sarcoma [38, 39]. essary to exclude endobronchial tumor as the
of an exudative pleural effusion with locula- cause of the finger-in-glove sign.
tion, inflammatory changes may thicken both Air Crescent Sign of Angioinvasive The tubular opacities that occur in ABPA
the visceral and parietal pleura that surround Aspergillus Infection result from hyphal masses and mucoid im-
the fluid collection and may become evident The air crescent sign is the CT finding of a paction and typically affect the upper lobes.
as the split-pleura sign, suggesting the pres- crescentic collection of air that separates a In 1928% of cases, the endobronchial opac-
ence of empyema [28, 30]. A loculated effu- nodule or mass from the wall of a surround- ities in ABPA may be calcified or hyperatten-
sion may have an atypical chest radiographic ing cavity [2]. This sign is seen in two types uating on unenhanced CT images (Fig. 15),
appearance when located within a fissure. The of Aspergillus infection: angioinvasive and probably because of the presence of calcium
split-pleura sign may be seen in combination mycetoma [40]. In angioinvasive Aspergillus salts, metals, and desiccated mucus [4750].
with the air-fluid level sign when a broncho- infection, the sign is caused by parenchymal
pleural fistula occurs within empyema. cavitation, typically occurs 2 weeks after de- Crazy-Paving Sign
Empyema should be considered when a tection of the initial radiographic abnormal- The crazy-paving sign is the CT finding of
patient presents with fever, cough, and chest ity, and coincides with the return of neutro- a combination of ground-glass opacity and
pain and CT shows the split-pleura sign. In a phil function (Fig. 13). The air crescent sign smooth interlobular septal thickening that re-
series of 58 patients with empyema, the split- is suggestive of a favorable patient prognosis sembles a masonry pattern used in walkways
pleura sign was seen in 68% [30] (Fig. 9). The [41]. The intracavitary nodule represents ne- [2]. The crazy-paving sign was originally de-
split-pleura sign is not specific for empyema crotic, retracted lung tissue that is separated scribed as a characteristic CT pattern detect-
but rather indicates the presence of an exuda- from peripheral viable but hemorrhagic lung ed in patients with pulmonary alveolar pro-
tive effusion [31]. Other important causes of parenchyma seen as outer consolidation or teinosis. The sign has come to be recognized,
this sign include parapneumonic and malig- ground-glass opacity [42]. however, as occurring in many other condi-
AJR:202, March 2014 481
Walker et al.
tions, including infection (e.g., Pneumocystis trilobular nodules are evenly spaced and do The hydatid cyst is composed of three lay-
jiroveci pneumonia, influenza, and infections not come into contact with adjacent pleural ers: an outer protective barrier consisting of
by other organisms) [51, 52]. In Pneumocystis surfaces. Perilymphatic nodules are distribut- modified host cells, called the pericyst; a
pneumonia, the histologic features that pro- ed along peribronchovascular structures, the middle acellular laminated membrane, called
duce the crazy-paving pattern are alveolar subpleural lung, and along interlobular sep- the ectocyst; and an inner germinal layer that
exudates containing the infective organisms ta. Random nodules forming the miliary pat- produces scolices, hydatid fluid, daughter
and cellular infiltration or edema in the alveo- tern are distributed uniformly throughout the vesicles, and daughter cysts, called the en-
lar walls and interlobular septa [52, 53]. An- lungs, and those in the periphery may come docyst [74, 75, 77]. The meniscus, Cumbo,
cillary clinical or radiographic features sug- into contact with a pleural surface [61, 62]. and water lily signs are all seen with pulmo-
gestive of Pneumocystis pneumonia include a Noninfectious causes of the miliary pattern nary echinococcal infection [7478]. These
history of immunosuppression, imaging include metastatic disease, IV injected for- signs are caused by air dissecting between the
findings of pulmonary cysts, and the occur- eign material, and rarely sarcoidosis [62, 63]. cyst layers, which are initially indistin-
rence of secondary spontaneous pneumotho- guishable on CT images because the cysts are
rax [54] (Fig. 17). Reverse Halo and Birds Nest Signs fluid filled (Fig. 22). With bronchial erosion,
Differential diagnostic considerations for The reverse halo sign is the CT finding of air dissects between the outer pericyst and
the crazy-paving sign can be categorized peripheral consolidation surrounding a cen- ectocyst to produce the meniscus sign (Fig.
according to the typical time course of the tral area of ground-glass opacity [64]. As- 23). Some radiologists believe that the me-
suspected diseases (Fig. 18). Diseases char- sociated irregular and intersecting areas of niscus sign is suggestive of impending cyst
acterized by an acute time course include stranding or irregular lines may be present rupture [76, 77]. As it accumulates further, air
pulmonary edema, pulmonary hemorrhage, within the area of ground-glass opacity and penetrates the endocyst layer and causes the
and infection. Those with a more chronic become evident as the birds nest sign [65] Cumbo sign, which comprises an air-flu- id
American Journal of Roentgenology 2014.202:479-492.
course include pulmonary alveolar proteino- (Fig. 21). These signs are suggestive of in- level in the endocyst and a meniscus sign
sis, pulmonary adenocarcinoma, and lipoid vasive fungal infection (e.g., angioinvasive (Fig. 23). Finally, the endocyst layer collaps-
pneumonia [52, 55]. Aspergillus infection or mucormycosis) in es and floats on fluid, forming the water lily
susceptible patient populations [66]. Major sign (Fig. 24).
Grape-Skin Sign predisposing factors for fungal infection in-
The grape-skin sign is the radiographic or clude stem cell or solid organ transplant, he- Burrow Sign of Paragonimiasis
CT finding of a very thin-walled cavitary le- matologic malignancy, diabetic ketoacidosis, Paragonimiasis is a zoonotic parasitic in-
sion that develops in lung parenchyma pre- and a depressed immune system. Imaging fea- fection caused by lung flukes [79]. Humans
viously affected by consolidation or lung tures that favor mucormycosis over Aspergillus serve as a definitive host when they ingest
granulomas that have undergone central ca- infection in a neutropenic patient are detec- raw or improperly cooked crab or crayfish [76].
seous necrosis [56]. As classically described, tion of the reverse halo or birds nest sign, Paragonimus westermani and Paragonimus
the grape-skin sign is a solitary finding of a multiplicity of pulmonary nodules (> 10), and kellicotti are the two pathogens endemic to
thin-walled cavity with central lucency that development of infection despite vori- Asia and North America, respectively. They
has been associated with chronic pulmonary conazole prophylaxis [6668]. The reverse produce similar imaging findings in the tho-
coccidioidomycosis infection [57, 58] (Fig. halo and birds nest signs are not specific for rax [7983].
19). Over time the lesion may deflate, or it invasive fungal infection and may also be The chest CT findings reflect the life cycle
may rupture into the pleural space, the result seen in other conditions, including crypto- of the parasite. The second form of the imma-
being pneumothorax [56, 59]. The differen- genic organizing pneumonia, bacterial pneu- ture organism lives in the crab or crayfish. Af-
tial diagnosis of this finding includes other monia, paracoccidioidomycosis, tuberculo- ter ingestion by a mammal, the parasite pen-
solitary cavitary or cystic lesions, such as re- sis, sarcoidosis, Wegener granulomatosis, etrates through the small bowel to enter the
activation tuberculosis infection, pneumato- and pulmonary infarction [64, 6873]. peritoneal cavity, where it incites an inflam-
cele, neoplasm (e.g., primary lung cancer or matory reaction. Several weeks later, the or-
metastasis), and other fungal infections. Meniscus, Cumbo, and Water Lily ganism migrates through the diaphragm to en-
Signs of Echinococcal Infection ter the pleural space. After finding mates, the
Miliary Pattern Pulmonary hydatid disease is a zoonotic parasites burrow through the visceral pleura
The miliary pattern consists of multiple parasitic infection caused by the larval stage into the lung parenchyma, where they produce
small (< 3 mm) pulmonary nodules of similar of Echinococcus tapeworms [74]. This ge- cysts that contain eggs. The eggs are extrud-
size that are randomly distributed throughout nus of worms is endemic in Alaska, South ed into bronchioles and expectorated by the
both lungs [2]. This pattern implies hematog- America, the Mediterranean region, Africa, infected mammal to complete the life cycle
enous dissemination of disease and is clas- and Australia. Humans can serve as interme- [79]. The burrow sign is a linear track extend-
sically associated with tuberculosis but can diate hosts after contact with a definitive host ing from the pleural surface or hemidiaphragm
also be seen with other infections, such as (e.g., dog or wolf) or after consuming con- to a cavitary or cystic pulmonary nodule. The
histoplasmosis and coccidioidomycosis, par- taminated vegetables or water [74]. The lung linear track represents the path followed by
ticularly in immunocompromised individuals is the second most common organ involved, the worms within the lung, and the cavitary
[60] (Fig. 20). Random pulmonary nodules after the liver, and is infected by either hema- or cystic pulmonary nodule contains both the
must be differentiated from those with a cen- togenous or direct transdiaphragmatic spread adult worms and their eggs (Fig. 25). There is
trilobular or perilymphatic distribution. Cen- from the liver [7476]. often associated pleural effusion, omental fat
482 AJR:202, March 2014
Imaging Pulmonary Infection
stranding, and anterior cardiophrenic and in- 11. Li Ng Y, Hwang D, Patsios D, Weisbrod G. Tree- L, Krivoruk V, Kramer MR. Factors predicting
ternal mammary lymphadenopathy. Patients in-bud pattern on thoracic CT due to pulmonary mortality of patients with lung abscess. Chest
occasionally present with pneumothorax [79 intravascular metastases from pancreatic adeno- 1999; 115:746750
83]. Recognizing the linear burrow track is the carcinoma. J Thorac Imaging 2009; 24:150151 28. Kuhlman JE, Singha NK. Complex disease of the
key to differentiating this entity from others, 12. Franquet T, Gimnez A, Prats R, Rodrguez-Arias pleural space: radiographic and CT evaluation.
such as malignancy, fungal infection, and tu- JM, Rodrguez C. Thrombotic microangiopathy of RadioGraphics 1997; 17:6379
berculosis [8083]. pulmonary tumors: a vascular cause of tree-in-bud 29. Kuhlman JE. Complex disease of the pleural
pattern on CT. AJR 2002; 179:897899 space: the 10 questions most frequently asked of
Conclusion 13. Bendeck SE, Leung AN, Berry GJ, Daniel D, the radiologistnew approaches to their answers
Imaging plays an important role in the di- Ruoss SJ. Cellulose granulomatosis presenting as with CT and MR imaging. RadioGraphics 1997;
agnosis of suspected pulmonary infection and centrilobular nodules: CT and histologic find- 17:10431050
may reveal useful signs at chest radiog- raphy ings. AJR 2001; 177:11511153 30. Stark DD, Federle MP, Goodman PC, Podrasky
and CT. Signs such as the water lily and 14. Tack D, Nollevaux MC, Gevenois PA. Tree-in- AE, Webb WR. Differentiating lung abscess and
burrow signs almost always indicate a bud pattern in neoplastic pulmonary emboli. AJR empyema: radiography and computed tomogra-
specific infection, whereas findings such as 2001; 176:14211422 phy. AJR 1983; 141:163167
the split-pleura sign often suggest a specif- ic 15. Shepard JA, Moore EH, Templeton PA, McLoud 31. Aquino SL, Webb WR, Gushiken BJ. Pleural ex-
diagnosis of empyema in the clinical set- ting TC. Pulmonary intravascular tumor emboli: di- udates and transudates: diagnosis with contrast-
of pneumonia. Several signs, such as the halo lated and beaded peripheral pulmonary arteries at enhanced CT. Radiology 1994; 192:803808
and reverse halo signs, may indicate po- CT. Radiology 1993; 187:797801 32. Pinto PS. The CT halo sign. Radiology 2004;
tentially serious fungal infections in an im- 16. Francis JB, Francis PB. Bulging (sagging) fissure 230:109110
munocompromised patient. Imaging signs of sign in Hemophilus influenzae lobar pneumonia. 33. Kuhlman JE, Fishman EK, Siegelman SS. Inva-
American Journal of Roentgenology 2014.202:479-492.
lung abscess, such the an air-fluid level sign South Med J 1978; 71:14521453 sive pulmonary aspergillosis in acute leukemia:
in a cavity, may also be predictive of progno- 17. Felson B, Rosenberg LS, Hamburger M. Roent- characteristic findings on CT, the CT halo sign,
sis and guide duration of therapy. gen findings in acute Friedlnders pneumonia. and the role of CT in early diagnosis. Radiology
Radiology 1949; 53:559565 1985; 157:611614
References 18. Korvick JA, Hackett AK, Yu VL, Muder RR. 34. Kuhlman JE, Fishman EK, Burch PA, Karp JE,
1. Hoyert DL, Xu J. Deaths: preliminary data for Klebsiella pneumonia in the modern era: clinico- Zerhouni EA, Siegelman SS. Invasive pulmonary
2011. Natl Vital Stat Rep 2012; 61:151 radiographic correlations. South Med J 1991; aspergillosis in acute leukemia: the contribution
2. Hansell DM, Bankier AA, MacMahon H, McLoud 84:200204 of CT to early diagnosis and aggressive manage-
TC, Mller NL, Remy J. Fleischner So- ciety: 19. Rafat C, Fihman V, Ricard JD. A 51-year-old man ment. Chest 1987; 92:9599
glossary of terms for thoracic imaging. Ra- presenting with shock and lower-lobe con- 35. Won HJ, Lee KS, Cheon JE, et al. Invasive pul-
diology 2008; 246:697722 solidation with interlobar bulging fissure. Chest monary aspergillosis: prediction at thin-section
3. Fleischner FG. The visible bronchial tree; a roent- 2013; 143:11671169 CT in patients with neutropeniaa prospective
gen sign in pneumonic and other pulmonary con- 20. Kuhlman JE, Fishman EK, Teigen C. Pulmonary study. Radiology 1998; 208:777782
solidations. Radiology 1948; 50:184189 septic emboli: diagnosis with CT. Radiology 36. Caillot D, Couaillier JF, Bernard A, et al. In-
4. Fleischner FG. Der sichtbare Bronchialbaum, ein 1990; 174:211213 creasing volume and changing characteristics of
differentialdiagnostisches Symptom im Rntgen- 21. Huang RM, Naidich DP, Lubat E, Schinella R, invasive pulmonary aspergillosis on sequential
bild der Pneumonia. Fortschr Geb Rontgenstr Garay SM, McCauley DI. Septic pulmonary em- thoracic computed tomography scans in patients
1927; 36:319323 boli: CT-radiographic correlation. AJR 1989; with neutropenia. J Clin Oncol 2001; 19:253259
5. Felson B, Felson H. Localization of intrathoracic 153:4145 37. Greene RE, Schlamm HT, Oestmann JW, et al.
lesions by means of the postero-anterior roent- 22. Dodd JD, Souza CA, Mller NL. High-resolution Imaging findings in acute invasive pulmonary
genogram; the silhouette sign. Radiology 1950; MDCT of pulmonary septic embolism: evaluation aspergillosis: clinical significance of the halo
55:363374 of the feeding vessel sign. AJR 2006; 187:623 sign. Clin Infect Dis 2007; 44:373379
6. Verma N, Chung JH, Mohammed TL. Tree-in- 629 38. Primack SL, Hartman TE, Lee KS, Mller NL.
bud sign. J Thorac Imaging 2012; 27:W27 23. Milne EN, Zerhouni EA. Blood supply of pulmo- Pulmonary nodules and the CT halo sign. Radi-
7. Eisenhuber E. The tree-in-bud sign. Radiology nary metastases. J Thorac Imaging 1987; 2:1523 ology 1994; 190:513515
2002; 222:771772 24. Han D, Lee KS, Franquet T, et al. Thrombotic and 39. Jamadar DA, Kazerooni EA, Daly BD, White CS,
8. Rossi SE, Franquet T, Volpacchio M, Gimnez A, nonthrombotic pulmonary arterial embo- lism: Gross BH. Pulmonary zygomycosis: CT appear-
Aguilar G. Tree-in-bud pattern at thin-section CT spectrum of imaging findings. Radio- Graphics ance. J Comput Assist Tomogr 1995; 19:733738
of the lungs: radiologic-pathologic overview. Ra- 2003; 23:15211539 40. Buckingham SJ, Hansell DM. Aspergillus in the
dioGraphics 2005; 25:789801 25. Ketai L, Jordan K, Marom EM. Imaging infec- lung: diverse and coincident forms. Eur Radiol
9. Collins J, Blankenbaker D, Stern EJ. CT patterns tion. Clin Chest Med 2008; 29:77105 2003; 13:17861800
of bronchiolar disease: what is tree-in-bud? AJR 26. Donnelly LF, Klosterman LA. Pneumonia in 41. Abramson S. The air crescent sign. Radiology
1998; 171:365370 children: decreased parenchymal contrast en- 2001; 218:230232
10. Im JG, Itoh H, Shim YS, et al. Pulmonary tuber- hancementCT sign of intense illness and im- 42. McAdams HP, Rosado-de-Christenson ML, Tem-
culosis: CT findingsearly active disease and pending cavitary necrosis. Radiology 1997; 205: pleton PA, Lesar M, Moran CA. Thoracic myco-
sequential change with antituberculous therapy. 817820 ses from opportunistic fungi: radiologic-patholog-
Radiology 1993; 186:653660 27. Hirshberg B, Sklair-Levi M, Nir-Paz R, Ben-Sira ic correlation. RadioGraphics 1995; 15:271286
AJR:202, March 2014 483
Walker et al.
43. Bard R, Hassani N. Crescent sign in pulmonary 57. Chong S, Lee KS, Yi CA, Chung MJ, Kim TS, 70. Gasparetto EL, Escuissato DL, Davaus T, et al.
hematoma. Respiration 1975; 32:247251 Han J. Pulmonary fungal infection: imaging find- Reversed halo sign in pulmonary paracoccidioi-
44. Cubillo-Herguera E, McAlister WH. The pulmo- ings in immunocompetent and immunocompro- domycosis. AJR 2005; 184:19321934
nary meniscus sign in a case of bronchogenic car- mised patients. Eur J Radiol 2006; 59:371383 71. Marchiori E, Grando RD, Simes Dos Santos CE,
cinoma. Radiology 1969; 92:12991300 58. Kim KI, Leung AN, Flint JD, Mller NL. Chron- et al. Pulmonary tuberculosis associated with the
45. Nguyen ET. The gloved finger sign. Radiology ic pulmonary coccidioidomycosis: computed to- reversed halo sign on high-resolution CT. Br J Ra-
2003; 227:453454 mographic and pathologic findings in 18 patients. diol 2010; 83:e58e60
46. Mintzer RA, Neiman HL, Reeder MM. Mucoid im- Can Assoc Radiol J 1998; 49:401407 72. Marchiori E, Zanetti G, Mano CM, Hochhegger B,
paction of a bronchus. JAMA 1978; 240:13971398 59. McAdams HP, Rosado-de-Christenson ML, Lesar Irion KL. The reversed halo sign: another atyp- ical
47. Agarwal R, Aggarwal AN, Gupta D. High-attenu- M, Templeton PA, Moran CA. Thoracic mycoses manifestation of sarcoidosis. Korean J Radiol
ation mucus in allergic bronchopulmonary asper- from endemic fungi: radiologic-pathologic correla- 2010; 11:251252
gillosis: another cause of diffuse high-attenuation tion. RadioGraphics 1995; 15:255270 73. Mango VL, Naidich DP, Godoy MC. Reversed
pulmonary abnormality. AJR 2006; 186:904 60. Burrill J, Williams CJ, Bain G, Conder G, Hine halo sign after radiofrequency ablation of a lung
48. Agarwal R, Gupta D, Aggarwal AN, Saxena AK, AL, Misra RR. Tuberculosis: a radiologic review. nodule. J Thorac Imaging 2011; 26:W150W152
Chakrabarti A, Jindal SK. Clinical significance of RadioGraphics 2007; 27:12551273 74. Pedrosa I, Saz A, Arrazola J, Ferreirs J, Pedrosa
hyperattenuating mucoid impaction in allergic 61. Gruden JF, Webb WR, Naidich DP, McGuinness CS. Hydatid disease: radiologic and pathologic
bronchopulmonary aspergillosis: an analysis of G. Multinodular disease: anatomic localization at features and complications. RadioGraphics 2000;
155 patients. Chest 2007; 132:11831190 thin-section CTmultireader evaluation of a 20:795817
49. Logan PM, Mller NL. High-attenuation mucous simple algorithm. Radiology 1999; 210:711720 75. Polat P, Kantarci M, Alper F, Suma S, Koruyucu
plugging in allergic bronchopulmonary aspergil- 62. Lee KS, Kim TS, Han J, et al. Diffuse micronodu- MB, Okur A. Hydatid disease from head to toe.
losis. Can Assoc Radiol J 1996; 47:374377 lar lung disease: HRCT and pathologic findings. J RadioGraphics 2003; 23:475494
American Journal of Roentgenology 2014.202:479-492.
50. Agarwal R. High attenuation mucoid impaction in Comput Assist Tomogr 1999; 23:99106 76. Martnez S, Restrepo CS, Carrillo JA, et al. Tho-
allergic bronchopulmonary aspergillosis. World J 63. Koyama T, Ueda H, Togashi K, Umeoka S, Kata- racic manifestations of tropical parasitic infec-
Radiol 2010; 2:4143 oka M, Nagai S. Radiologic manifestations of sar- tions: a pictorial review. RadioGraphics 2005;
51. Murch CR, Carr DH. Computed tomography ap- coidosis in various organs. RadioGraphics 2004; 25:135155
pearances of pulmonary alveolar proteinosis. Clin 24:87104 77. Balikian JP, Mudarris FF. Hydatid disease of the
Radiol 1989; 40:240243 64. Walker CM, Mohammed TL, Chung JH. Re- lungs: a roentgenologic study of 50 cases. Am J Roent-
52. Rossi SE, Erasmus JJ, Volpacchio M, Franquet T, versed halo sign. J Thorac Imaging 2011; 26:W80 genol Radium Ther Nucl Med 1974; 122:692707
Castiglioni T, McAdams HP. Crazy-paving pattern 65. Vogl TJ, Hinrichs T, Jacobi V, Bhme A, Hoelzer D. 78. McPhail JL, Arora TS. Intrathoracic hydatid dis-
at thin-section CT of the lungs: radiologic-patho- Computed tomographic appearance of pulmonary ease. Dis Chest 1967; 52:772781
logic overview. RadioGraphics 2003; 23:15091519 mucormycosis [in German]. Rofo 2000; 172:604608 79. Procop GW. North American paragonimiasis
53. Marchiori E, Mller NL, Soares Souza A, Escuis- 66. Georgiadou SP, Sipsas NV, Marom EM, Kontoyi- (caused by Paragonimus kellicotti) in the context
sato DL, Gasparetto EL, Franquet T. Pulmonary annis DP. The diagnostic value of halo and reversed of global paragonimiasis. Clin Microbiol Rev
disease in patients with AIDS: high-resolution CT halo signs for invasive mold infections in compro- 2009; 22:415446
and pathologic findings. AJR 2005; 184:757764 mised hosts. Clin Infect Dis 2011; 52:11441155 80. Henry TS, Lane MA, Weil GJ, Bailey TC, Bhalla
54. Kanne JP, Yandow DR, Meyer CA. Pneumocystis 67. Chamilos G, Marom EM, Lewis RE, Lionakis MS, S. Chest CT features of North American para-
jiroveci pneumonia: high-resolution CT findings Kontoyiannis DP. Predictors of pulmonary zygomy- gonimiasis. AJR 2012; 198:10761083
in patients with and without HIV infection. AJR cosis versus invasive pulmonary aspergillosis in 81. Im JG, Whang HY, Kim WS, Han MC, Shim YS,
2012; 198:[web]W555W561 patients with cancer. Clin Infect Dis 2005; 41:6066 Cho SY. Pleuropulmonary paragonimiasis: radio-
55. Franquet T, Gimnez A, Bordes R, Rodrguez- 68. Chung JH, Godwin JD, Chien JW, Pipavath SJ. logic findings in 71 patients. AJR 1992; 159:3943
Arias JM, Castella J. The crazy-paving pattern in Case 160: pulmonary mucormycosis. Radiology 82. Kim TS, Han J, Shim SS, et al. Pleuropulmonary
exogenous lipoid pneumonia: CT-pathologic cor- 2010; 256:667670 paragonimiasis: CT findings in 31 patients. AJR
relation. AJR 1998; 170:315317 69. Kim SJ, Lee KS, Ryu YH, et al. Reversed halo 2005; 185:616621
56. McGahan JP, Graves DS, Palmer PE, Stadalnik sign on high-resolution CT of cryptogenic orga- 83. Im JG, Kong Y, Shin YM, et al. Pulmonary para-
RC, Dublin AB. Classic and contemporary imaging nizing pneumonia: diagnostic implications. AJR gonimiasis: clinical and experimental studies.
of coccidioidomycosis. AJR 1981; 136:393404 2003; 180:12511254 RadioGraphics 1993; 13:575586
(Figures start on next page)
484 AJR:202, March 2014
Imaging Pulmonary Infection
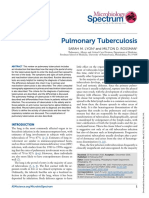
Gambar 1. pria 49 tahun dengan pneumonia lobus kiri bawah. Contoh tanda Gambar 2. gadis 4 tahun dengan pneumonia lingular. Contoh tanda silhoutte.
air bronchogram. Posteroanterior radiografi (kiri) dan coronal CT gambar Posteroanterior radiografi menunjukkan gambaran normal (kanan) dan hilangnya
American Journal of Roentgenology 2014.202:479-492.
(kanan) menunjukkan konsolidasi lobus kiri bawah dan tanda bronchogram gambaran normal paru-paru dan perbatasan bagian kiri jantung (kiri), seperti
udara (panah). itulah kelainan pada lokasi lingula.
Gambar 3. Pria 45 tahun dengan reaktivasi tuberkulosis. Contoh untuk tanda
tree-in-bud. Foto (atas) menunjukkan budding tree. foto CT bagian Axial
(bawah) menunjukkan banyaknya kekeruhan pada tree-in-bud dengan
bentuk V dan Y.
AJR:202, March 2014 485
Walker et al.
Gambar 4. Pria 40 tahun setelah suntikan IV dari Gambar 5. Pria 75 tahun dengan alkoholisme dan Klebsiella pneumonia. Contoh tanda bulging
tablet morfin sulfat yang hancur. Contoh tanda tree- fissure. Pada radiografi posteroanterior (kiri) dan lateral (kanan) menunjukkan konsolidasi lobus kanan
in-bud. Proyeksi gambaran axial dengan intensitas atas menyebabkan penonjolan bagian inferior pada fisura minor (panah hitam), penonjolan posterior
maksimum menunjukkan difus vaskular tree-in-bud dari fisura mayor (panah putih), dan perpindahan inferomedial dari bronkus intermedius (tanda
opasitas dan pelebaran pada arteri pulmonalis bintang).
American Journal of Roentgenology 2014.202:479-492.
utama. Temuan serupa melibatkan semua aspek
pada kedua paru-paru. Infeksius bronkiolitis atau
aspirasi tidak mungkin mendapatkan hasil distribusi
bilateral yang difus pada kekeruhan tree-in-bud, dan
kondisi lain, seperti panbronchiolitis difus dan injeksi
bahan asing, seperti dalam kasus ini, harus
dipertimbangkan sebagai diagnosis alternatif.
Gambar 6. Pria 45 tahun dengan emboli septik. Contoh tanda feeding Gambar 7. Pria 55 tahun dengan proses nekrosis
vessel. Gambar CT coronal menunjukkan emboli septik paru sebagai pada aspirasi pneumonia. Contoh peningkatan
nodul perifer yang solid dan kavitas paru dengan berbagai ukuran. homogen. Peningkatan aksial pada gambar CT
Banyak nodul yang memperlihatkan tanda feeding vessel (panah). menunjukkan peningkatkan gambaran
konsolidasi yang heterogen pada lobus kanan
bawah (panah) dicurigai sebagai permulaan
nekrosis di paru. Juga tampak adalah fokus
udara (panah) mewakili awal pembentukan
abses dan efusi pleura kanan pada lokulasi kecil
(tanda bintang).
486 AJR:202, March 2014
Imaging Pulmonary Infection
A B
Gambar 8. pria berusia 35 tahun dengan pneumonia Staphylococcus aureus membentuk abses paru. Contoh tanda air fluid level.
A, Gambaran radiografi posteroanterior (kiri) dan lateral (kanan) menunjukkan kavitas pada lobus kanan bawah dengan air fluid level (panah) dengan panjang yang
sama pada kedua pandangan orthogonal. Tebal, dinding tidak teratur ciri khas abses paru yang jelas.
B, Gambaran axial padal CT menunjukkan lokasi kavitas pada parenkim lobus kanan bawah dengan air fluid level, kontur internal yang tidak teratur, dan bronkus
yang terkait (panah) menyebabkan lesi.
Gambar 9. Wanita 48 tahun dengan empiema. Contoh tanda split-pleura. Gambar 10. Pria 65 tahun dengan efusi pleura ganas. Contoh tanda split-pleura.
Pada kontras gambar CT yang ditingkatkan Aksial (kiri) dan sagital (kanan) Pada kontras gambar CT yang ditingkatkan Aksial (kiri) dan sagital (kanan)
menunjukkan menebal visceral(Panah) dan parietal (panah putih) pleura menunjukkan penebalan visceral (panah) dan parietal (panah) pleura dengan
terpisah dari keadaan normal mereka (yaitu, split) untuk mengelilingi lokulasi efusi terkait. Tanda split-pleura hanya menunjukkan adanya efusi eksudatif dan
empiema. atelektasis yang berdekatan jelas terkihat pada lobus kanan bawah. harus berkorelasi dengan temuan klinis dan thorakosentesis untuk menegakkan
tanda split-pleura tidak spesifik untuk empiema melainkan menjadi indikasi diagnosis yang akurat.
adanya efusi eksudatif. chest tube adalah tidak terlihat secara utuh (panah
hitam).
AJR:202, March 2014 487
Walker et al.
American Journal of Roentgenology 2014.202:479-492.
Gambar 11. Pria 35 tahun dengan demam, neutropenia, dan infeksi Aspergillus Gambar 12. Pria 47 tahun dengan kandidiasis yang menyebar. Contoh
angioinvasif. Contoh tanda halo. Radiografi posteroanterior dan gambar aksial tanda halo. Gambar axial CT menunjukkan beberapa nodul bilateral pada
CT menunjukkan massa lobus kanan atas dengan gambaran cahaya bulat paru dengan sekitar gambaran cahaya bulat pada kekeruhan.
dipinggir kekeruhan (panah) yang merupakan tanda halo.
Fig. 1338-year-old man Gambar 13. Pria 38 tahun dengan infeksi Gambar14. Wanita 65tahun dengan misetomaIntrakaviter. Contohtandaair crescent atauMonad.
Aspergillus angioinvasif. Contoh tanda air crescent. Gambar CT aksial gambarCT supineaxial(kiri)danprone(kanan)menunjukkan bolajamur(misetoma)yangmengikuti
(kiri) dan koronal (kanan) menunjukkan tanda crescent sign (panah), gravitasi.Tandaaircrescentdarimisetomaterjadipadapasiendenganimunokompeten.Jamurbola
yang terjadi pada pasien pemulihan netrofil dengan berkembangdalamkavitasyangsudahadasebelumnya,biasanyaberhubungandengantuberkulosis
immunokompromise. nodul intrakaviter (tanda bintang) merupakan atausarcoidosis.
jaringan paru-paru nekrotik.
.
488 AJR:202, March 2014
Imaging Pulmonary Infection
Fig. 1525-year-old
woman with allergic
bronchopulmonary
aspergillosis (ABPA).
Example of finger-in-
glove sign.
A, Posteroanterior
radiograph shows
branching tubular
opacities (arrows)
emanating from both hila.
B, Unenhanced axial
(left) and oblique sagittal
(right) CT images show
branching tubular
opacities (arrows)
with high attenuation.
Opacities in ABPA are
composed of hyphal
masses, and mucoid
impaction and may be
calcified on CT images in
as many as 28% of cases.
American Journal of Roentgenology 2014.202:479-492.
A B
Fig. 1663-year-old man with squamous cell lung cancer. Example of finger-in- Fig. 1724-year-old man with HIV infection and
glove sign. Posteroanterior radiograph (top left) and corresponding coronal (top Pneumocystis pneumonia. Example of crazy-paving
right) and axial (bottom) CT images show branching tubular opacity (arrows) in sign. Axial CT image shows diffuse ground-glass
right upper lobe. Proximal portion of branching opacity was FDG avid (not shown) opacity with areas of superimposed interlobular
and represented tumor, whereas rest of opacity represented mucoid impaction in septal thickening (combination that forms crazy-
dilated bronchus. paving pattern) and multiple thin-walled cysts. In
HIV-positive patient with dyspnea, findings are most
consistent with Pneumocystis pneumonia.
AJR:202, March 2014 489
Walker et al.
American Journal of Roentgenology 2014.202:479-492.
Fig. 18CT scans show crazy-paving sign in patients with various disorders. Differential diagnostic
considerations are influenced by patients clinical presentation and disease course. In patients with acute
symptoms, crazy-paving sign may represent pulmonary edema, pulmonary hemorrhage, or infection. In patients
with chronic symptoms, crazy-paving sign may represent lipoid pneumonia, lung cancer, or pulmonary alveolar
proteinosis (PAP).
Fig. 1955-year-old man with chronic Fig. 2029-year-old man with AIDS (CD4 count,
coccidioidomycosis infection. Example of grape-skin 10/L) and disseminated histoplasmosis. Example
sign. Posteroanterior radiograph shows thin-walled of miliary pattern. Axial CT image shows multiple
grape-skin cyst (arrows). Axial CT image (inset) small pulmonary nodules distributed uniformly
shows that over time cavity may deflate and acquire throughout both lungs. Some nodules are in contact
slightly thicker wall. with major fissure and subpleural lung and have no
relation to secondary pulmonary lobules. Differential
considerations for randomly distributed pulmonary
nodules include miliary infection (e.g., tuberculosis,
histoplasmosis), metastatic disease, and rarely
sarcoidosis.
490 AJR:202, March 2014
Imaging Pulmonary Infection
Fig. 2144-year-old man with febrile neutropenia and pulmonary mucormycosis.
Example of reverse halo and birds nest signs. Axial (left) and coronal (right) CT
images show peripheral rim of consolidation (arrows) surrounding central ground-
glass opacity, reticulation, and nodularity. This appearance has been likened
to birds nest and reverse halo. Early diagnosis of mucormycosis pneumonia is
imperative because standard voriconazole therapy is not effective for treatment.
(Courtesy of Chou S, University of Washington, Seattle, WA)
American Journal of Roentgenology 2014.202:479-492.
Fig. 22Drawings show normal hydatid cyst and meniscus, Cumbo, and water lily signs. (Courtesy of Loomis S,
REMS Media Services, Mass General Imaging, Boston, MA)
AJR:202, March 2014 491
Walker et al.
Fig. 2349-year-old man with pulmonary hydatid disease. Example of meniscus Fig. 2427-year-old woman with pulmonary hydatid
(left) and Cumbo (right) signs. Chest CT images show air between pericyst and disease. Example of water lily sign. Posteroanterior
ectocyst layers (arrows) consistent with meniscus sign. Air-fluid level in endocyst radiograph shows large right lower lobe thick-walled
(arrowhead) in combination with meniscus sign forms Cumbo sign. (Courtesy of cavity with lobulated airsoft-tissue interface
Rossi S, Centro de Diagnostico Dr Enrique Rossi, Buenos Aires, Argentina) representing floating endocyst (arrow). Coronal
CT image (inset) from earlier examination shows
unruptured cyst.
American Journal of Roentgenology 2014.202:479-492.
A B
Fig. 2532-year-old man with North American paragonimiasis after ingestion of raw crayfish. Example of burrow sign. (Courtesy of
Henry T, Emory University, Atlanta, GA)
A, Axial CT images in soft-tissue (left) and lung (right) windows shows linear burrow track (arrows) extending from thickened pleura to
pulmonary nodule.
B, Axial CT image shows long linear burrow track (arrow) in right upper lobe and small pneumothorax.
This article is available for CME and Self-Assessment (SA-CME) credit that satisfies Part II requirements for
maintenance of certification (MOC). To access the examination for this article, follow the prompts associated with
the online version of the article.
492 AJR:202, March 2014
This article has been cited by:
1. Mandeep Garg, Nidhi Prabhakar, P. Kiruthika, Ritesh Agarwal, Ashutosh Aggarwal, Ajay Gulati, Niranjan Khandelwal. 2017.
Imaging of Pneumonia: An Overview. Current Radiology Reports 5:4. . [CrossRef]
2. Gracijela Bozovic, Catharina Adlercreutz, Peter Hglund, Isabella Bjrkman-Burtscher, Peter Reinstrup, Richard Ingemansson,
Cornelia Schaefer-Prokop, Roger Siemund, Mats Geijer. 2017. Imaging of the Lungs in Organ Donors and its Clinical
Relevance. Journal of Thoracic Imaging 32:2, 107-114. [CrossRef]
3. R. Perolat, O. Stephanov, A. Mounier, A. Thiebaut, A. Pirvu, R. Hamidfar, G. Ferretti. 2017. Signe du halo invers chez un
patient neutropnique fbrile. Revue des Maladies Respiratoires . [CrossRef]
4. Subba R. DigumarthyThe Radiographic Patterns of Common Lung Diseases 37-58. [CrossRef]
5. Anagha P. Parkar, Panchakulasingam Kandiah. 2016. Differential Diagnosis of Cavitary Lung Lesions. Journal of the Belgian
Society of Radiology 100:1. . [CrossRef]
6. Satish Kumar Bajaj, Bernd Tombach. 2016. Respiratory infections in immunocompromised patients: Lung findings using chest
computed tomography. Radiology of Infectious Diseases . [CrossRef]
7. Nicolas Alberti, Xavier Buy, Nora Frulio, Michel Montaudon, Mathieu Canella, Afshin Gangi, Amandine Crombe, Jean
Palussire. 2016. Rare complications after lung percutaneous radiofrequency ablation: Incidence, risk factors, prevention and
management. European Journal of Radiology 85:6, 1181-1191. [CrossRef]
8. Niranjan Khandelwal, Kushaljit Singh Sodhi, Anindita Sinha, Jyothi G. Reddy, Eshwar N. Chandra. 2016. Multidetector
Computed Tomography and MR Imaging Findings in Mycotic Infections. Radiologic Clinics of North America 54:3, 503-518.
American Journal of Roentgenology 2014.202:479-492.
[CrossRef]
9. Catherine Beigelman-Aubry, Sabine SchmidtPulmonary Infections: Imaging with CT 131-161. [CrossRef]
10. Edson Marchiori, Glucia Zanetti, Myrna C. B. Godoy. 2014. Can Morphologic Characteristics of the Reversed Halo Sign
Narrow the Differential Diagnosis of Pulmonary Infections?. American Journal of Roentgenology 203:5, W557-W558. [Citation]
[Full Text] [PDF] [PDF Plus]
11. Christopher M. Walker, Subba R. Digumarthy. 2014. Reply to Can Morphologic Characteristics of the Reversed Halo Sign
Narrow the Differential Diagnosis of Pulmonary Infections?. American Journal of Roentgenology 203:5, W559-W559. [Citation]
[Full Text] [PDF] [PDF Plus]
Das könnte Ihnen auch gefallen
- Medical Mnemonic Sketches : Pulmonary DiseasesVon EverandMedical Mnemonic Sketches : Pulmonary DiseasesNoch keine Bewertungen
- Imaging Pulmonary Infection: Classic Signs and PatternsDokument14 SeitenImaging Pulmonary Infection: Classic Signs and PatternsSanti ParambangNoch keine Bewertungen
- Imaging Pulmonary Infection: Classic Signs and PatternsDokument18 SeitenImaging Pulmonary Infection: Classic Signs and Patternssofiana debbyNoch keine Bewertungen
- Infection PulmonaryDokument14 SeitenInfection Pulmonaryvina_vina100% (1)
- Imaging of Pulmonary Infection: Tomás Franquet and Johnathan H. ChungDokument13 SeitenImaging of Pulmonary Infection: Tomás Franquet and Johnathan H. ChungVictor ChiabaiNoch keine Bewertungen
- Rheumatoid Lung DisDokument28 SeitenRheumatoid Lung DisariceghaNoch keine Bewertungen
- Imaging in Chronic Obstructive Pulmonary DiseaseDokument9 SeitenImaging in Chronic Obstructive Pulmonary DiseasePramusetya SuryandaruNoch keine Bewertungen
- J6. Chest X-Ray Manifestations of Pneumonia - Das 2009Dokument3 SeitenJ6. Chest X-Ray Manifestations of Pneumonia - Das 2009Irwan DesriandaNoch keine Bewertungen
- Medical Progress: Review ArticleDokument9 SeitenMedical Progress: Review ArticleNicolás MateoJrNoch keine Bewertungen
- Imaging Pulmonary Infection: Classic Signs and PatternsDokument18 SeitenImaging Pulmonary Infection: Classic Signs and PatternsRizky MaulydaNoch keine Bewertungen
- NIH Public Access: Pulmonary Emphysema Subtypes On Computed Tomography in SmokersDokument23 SeitenNIH Public Access: Pulmonary Emphysema Subtypes On Computed Tomography in SmokersNurulAzizahAnNoch keine Bewertungen
- Diagnostic Evaluation of BronchiectasisDokument16 SeitenDiagnostic Evaluation of BronchiectasisAinun Jariah MuliadiNoch keine Bewertungen
- Smoking-Related Lung DiseaseDokument11 SeitenSmoking-Related Lung Diseaseasalizwa ludlalaNoch keine Bewertungen
- Macfarlane2021 - Bronquectasias (Review)Dokument7 SeitenMacfarlane2021 - Bronquectasias (Review)Nicolas SuarezNoch keine Bewertungen
- Organizing Pneumonia Following Covid19 PneumoniaDokument4 SeitenOrganizing Pneumonia Following Covid19 PneumoniaKhangNoch keine Bewertungen
- Lung Adenocarcinoma With Solitary MetastDokument88 SeitenLung Adenocarcinoma With Solitary MetastMikmik bay BayNoch keine Bewertungen
- Clinical Review - FullDokument5 SeitenClinical Review - FullAhmad SaifuddinNoch keine Bewertungen
- NeumoniaDokument14 SeitenNeumoniaPedro TumbacoNoch keine Bewertungen
- Blush 2012 Acute Bronchitis PDFDokument7 SeitenBlush 2012 Acute Bronchitis PDFMarimar FilardoNoch keine Bewertungen
- Key Points: Diagnostic Imaging in Adult Non-Cystic Fibrosis BronchiectasisDokument8 SeitenKey Points: Diagnostic Imaging in Adult Non-Cystic Fibrosis BronchiectasisAmirah SilinoNoch keine Bewertungen
- How To Investigate A Patient WithDokument6 SeitenHow To Investigate A Patient WithISABEL SOFIA CABARCAS COGOLLONoch keine Bewertungen
- Gharib2001 Radiologi Pneumonia-DikonversiDokument31 SeitenGharib2001 Radiologi Pneumonia-Dikonversitsamara24_Noch keine Bewertungen
- Murray 1988Dokument4 SeitenMurray 1988mesacarvajalinoNoch keine Bewertungen
- Pneumonia AspirasiDokument17 SeitenPneumonia Aspirasirini9384Noch keine Bewertungen
- Yossi Yarnic PDFDokument11 SeitenYossi Yarnic PDFAldo Pravando JulianNoch keine Bewertungen
- Other Conditions of The Lung (Abscesses, Inhaled Foreign Bodies, Bullous Lung Disease, Hydatid)Dokument5 SeitenOther Conditions of The Lung (Abscesses, Inhaled Foreign Bodies, Bullous Lung Disease, Hydatid)Zilvia TambengiNoch keine Bewertungen
- mc2985 1216Dokument8 Seitenmc2985 1216ade hajizah br ritongaNoch keine Bewertungen
- Pulmonary PerspectiveDokument8 SeitenPulmonary PerspectiveTony AndersonNoch keine Bewertungen
- RG 2018170048 PDFDokument21 SeitenRG 2018170048 PDFDiana CaballeroNoch keine Bewertungen
- Clinical and Radiological Evaluation of Emphysematous Chest - A Prospective StudyDokument5 SeitenClinical and Radiological Evaluation of Emphysematous Chest - A Prospective StudyTony AndersonNoch keine Bewertungen
- Pulmonary Tuberculosis 2017Dokument13 SeitenPulmonary Tuberculosis 2017GioNoch keine Bewertungen
- BronchiolitisDokument9 SeitenBronchiolitisretnomardiyantiNoch keine Bewertungen
- 1 s2.0 S0140673622014398 MainDokument14 Seiten1 s2.0 S0140673622014398 MainsilviaNoch keine Bewertungen
- What Is Pneumonia?: ReviewDokument6 SeitenWhat Is Pneumonia?: ReviewDavid SoaresNoch keine Bewertungen
- Peng Et Al-2020-Intensive Care Medicine PDFDokument2 SeitenPeng Et Al-2020-Intensive Care Medicine PDFTeodor ŞişianuNoch keine Bewertungen
- Microbiolspec - TNMI7 0032 2016Dokument13 SeitenMicrobiolspec - TNMI7 0032 2016Dhea Dwi AnandaNoch keine Bewertungen
- Bronquiolite DiagnosticoDokument14 SeitenBronquiolite DiagnosticoFrederico PóvoaNoch keine Bewertungen
- Respiratory Medicine Case ReportsDokument8 SeitenRespiratory Medicine Case ReportsdiahNoch keine Bewertungen
- Nihms 18315373Dokument36 SeitenNihms 18315373Kofi NekaNoch keine Bewertungen
- Parasitic Infections of The Lung: A Guide For The Respiratory PhysicianDokument9 SeitenParasitic Infections of The Lung: A Guide For The Respiratory Physicianحسام الدين إسماعيلNoch keine Bewertungen
- Parasitic Infections of The Lung: A Guide For The Respiratory PhysicianDokument9 SeitenParasitic Infections of The Lung: A Guide For The Respiratory PhysicianSuria KumarNoch keine Bewertungen
- Printed MaterialsDokument10 SeitenPrinted Materialsjesiegutay21Noch keine Bewertungen
- Absceso PulmonarDokument5 SeitenAbsceso PulmonarExpress Centro de copiadoNoch keine Bewertungen
- Desepida Finals FUNDALEC ReviewerDokument43 SeitenDesepida Finals FUNDALEC Reviewerethan lapidNoch keine Bewertungen
- 1 s2.0 S2211568412001702 Main PDFDokument10 Seiten1 s2.0 S2211568412001702 Main PDFGordana PuzovicNoch keine Bewertungen
- Chronic Airspace DiseasesDokument31 SeitenChronic Airspace DiseasesAnkita ShahNoch keine Bewertungen
- Maed 06 224Dokument6 SeitenMaed 06 224rizki romadaniNoch keine Bewertungen
- A 28 Year Old Man With Chest Pain, Shortness of BRDokument4 SeitenA 28 Year Old Man With Chest Pain, Shortness of BRagamerocallejasNoch keine Bewertungen
- Idiopathic Pulmonary FibrosisDokument13 SeitenIdiopathic Pulmonary FibrosisRaul David Maldonado LearyNoch keine Bewertungen
- Ipaf 2019Dokument10 SeitenIpaf 2019Edoardo CavigliNoch keine Bewertungen
- 2017 - PneumoniaDokument8 Seiten2017 - PneumoniablueicelandNoch keine Bewertungen
- Pneumonia PDFDokument17 SeitenPneumonia PDFRila NurulNoch keine Bewertungen
- Respiratory Symptoms and Signs: Key PointsDokument9 SeitenRespiratory Symptoms and Signs: Key PointsAna LopezNoch keine Bewertungen
- Fpi Nejm Clincal Practice 2018Dokument13 SeitenFpi Nejm Clincal Practice 2018cjonderedsonNoch keine Bewertungen
- Complicatii PneumonieDokument9 SeitenComplicatii PneumonieTatiana JalbaNoch keine Bewertungen
- Acremonium Pneumonia: Case Report and Literature Review: TanaffosDokument5 SeitenAcremonium Pneumonia: Case Report and Literature Review: TanaffosNurmawati AtNoch keine Bewertungen
- Chaaban 2013Dokument6 SeitenChaaban 2013Gede Brian Nugraha DenaNoch keine Bewertungen
- Acute Respiratory Distress Syndrome: Learning ObjectivesDokument5 SeitenAcute Respiratory Distress Syndrome: Learning ObjectivesElsa AivarNoch keine Bewertungen
- Imaging in Medical RehabilitationDokument76 SeitenImaging in Medical RehabilitationandrewNoch keine Bewertungen
- Aen Kelompok 1Dokument10 SeitenAen Kelompok 1mahkda anjaniNoch keine Bewertungen
- EXCEL CWH-harapanDokument10 SeitenEXCEL CWH-harapanChrist'na De RedArmyNoch keine Bewertungen
- Gan NingDokument1 SeiteGan NingChrist'na De RedArmyNoch keine Bewertungen
- Frekuensi Poli DewasaDokument9 SeitenFrekuensi Poli DewasaChrist'na De RedArmyNoch keine Bewertungen
- Frekuensi Poli DewasaDokument9 SeitenFrekuensi Poli DewasaChrist'na De RedArmyNoch keine Bewertungen
- Zhao YuDokument1 SeiteZhao YuChrist'na De RedArmyNoch keine Bewertungen
- Sun ShangDokument1 SeiteSun ShangChrist'na De RedArmyNoch keine Bewertungen
- Diao ChanDokument1 SeiteDiao ChanChrist'na De RedArmyNoch keine Bewertungen
- Zhao YunDokument1 SeiteZhao YunChrist'na De RedArmyNoch keine Bewertungen
- Zhuge LiangDokument1 SeiteZhuge LiangChrist'na De RedArmyNoch keine Bewertungen
- Zhuge LiangDokument1 SeiteZhuge LiangChrist'na De RedArmyNoch keine Bewertungen
- Zhao YunDokument1 SeiteZhao YunChrist'na De RedArmyNoch keine Bewertungen
- Manta ApsDokument1 SeiteManta ApsChrist'na De RedArmyNoch keine Bewertungen
- ZANISDokument1 SeiteZANISChrist'na De RedArmyNoch keine Bewertungen
- ZephysDokument1 SeiteZephysChrist'na De RedArmyNoch keine Bewertungen
- Ajr 13 11463Dokument15 SeitenAjr 13 11463Christ'na De RedArmyNoch keine Bewertungen
- RB 48 05 0275Dokument7 SeitenRB 48 05 0275Christ'na De RedArmyNoch keine Bewertungen
- Ajr 13 11463Dokument5 SeitenAjr 13 11463Christ'na De RedArmyNoch keine Bewertungen
- Man at at at Tatatata PPDokument1 SeiteMan at at at Tatatata PPChrist'na De RedArmyNoch keine Bewertungen
- Ajr 13 11463Dokument5 SeitenAjr 13 11463Christ'na De RedArmyNoch keine Bewertungen
- Ajr 13 11463Dokument25 SeitenAjr 13 11463Christ'na De RedArmyNoch keine Bewertungen
- MEdical Surgical REVEWERDokument86 SeitenMEdical Surgical REVEWERennaedNoch keine Bewertungen
- Practicum III by Dr. TC LeungDokument37 SeitenPracticum III by Dr. TC LeungAnonymous bQmwD4Noch keine Bewertungen
- NaloxoneDokument3 SeitenNaloxoneTracyNoch keine Bewertungen
- Indian Healthcare Sector Report at ConsultingDokument33 SeitenIndian Healthcare Sector Report at Consultingjyotichauhankv1Noch keine Bewertungen
- Superfical Parotidectomy Is Contraindicated in Patients With Sialectasis BecauseDokument24 SeitenSuperfical Parotidectomy Is Contraindicated in Patients With Sialectasis BecauseAbouzr Mohammed Elsaid100% (1)
- Hospitalpharmacy PDFDokument13 SeitenHospitalpharmacy PDFBhavin DesaiNoch keine Bewertungen
- Quality of Nursing Care Provided For PreDokument16 SeitenQuality of Nursing Care Provided For PreAmmar Mustafa Mahadi AlzeinNoch keine Bewertungen
- Nclex-Rn Essential Questions and RationalesDokument96 SeitenNclex-Rn Essential Questions and RationalesGloryJane100% (1)
- Pediatric Case StudyDokument29 SeitenPediatric Case Studyapi-296281683Noch keine Bewertungen
- Ethical Dilemmas of End of Life Care in Intensive Care Unit: A Literature ReviewDokument9 SeitenEthical Dilemmas of End of Life Care in Intensive Care Unit: A Literature ReviewEviNoch keine Bewertungen
- Aneurizma Bazilarke I TrombolizaDokument4 SeitenAneurizma Bazilarke I TrombolizaAnja LjiljaNoch keine Bewertungen
- Dysphagia in The Elderly PDFDokument11 SeitenDysphagia in The Elderly PDFangie villaizanNoch keine Bewertungen
- Mental Health Screening ToolsDokument2 SeitenMental Health Screening ToolsMinozu AryantiNoch keine Bewertungen
- Nur 129 Exam 2Dokument4 SeitenNur 129 Exam 2Stephanie DuvergeNoch keine Bewertungen
- ECG Definition: - PurposeDokument2 SeitenECG Definition: - PurposeJustine Karl Pablico100% (1)
- Physical and DiagnosticDokument20 SeitenPhysical and DiagnosticHaziq MarsNoch keine Bewertungen
- Diagnosis and Management of Meniscal Injury: PresentationDokument4 SeitenDiagnosis and Management of Meniscal Injury: PresentationemilyNoch keine Bewertungen
- Biological Explanations of Aggression: Sychology ActsheetsDokument4 SeitenBiological Explanations of Aggression: Sychology ActsheetsAyse Kerim100% (1)
- Comfort Theory Kolcaba EnglishDokument4 SeitenComfort Theory Kolcaba EnglishRahayu SavitriNoch keine Bewertungen
- GNU HealthDokument1 SeiteGNU Healthbhupendrapawar279Noch keine Bewertungen
- Gabriela Lara-Resume UpdatedDokument1 SeiteGabriela Lara-Resume Updatedapi-489922181Noch keine Bewertungen
- PFP Bedboard User GuideDokument87 SeitenPFP Bedboard User GuideSrinivas BhupathiNoch keine Bewertungen
- Death CertificateDokument16 SeitenDeath CertificateWisnu Agung WiyanggaNoch keine Bewertungen
- Admission Note TemplateDokument4 SeitenAdmission Note TemplateTauhid Mahmud100% (2)
- SOGC Clinical Guideline LiomyomaDokument22 SeitenSOGC Clinical Guideline LiomyomaSarah MuharomahNoch keine Bewertungen
- Trauma Wajah Tutorial - PPTX RevDokument49 SeitenTrauma Wajah Tutorial - PPTX RevShinta Andi SarasatiNoch keine Bewertungen
- Pediatric Basic Life SupportDokument50 SeitenPediatric Basic Life SupportnurmauliarizkyNoch keine Bewertungen
- Individual Case StudyDokument13 SeitenIndividual Case Studyankita mandalNoch keine Bewertungen
- Cerumen Management PDFDokument10 SeitenCerumen Management PDFHimawan WidyatmikoNoch keine Bewertungen
- The Health Insurance SpecialistDokument8 SeitenThe Health Insurance SpecialistsaranyaNoch keine Bewertungen