Das könnte Ihnen auch gefallen
- Borang Denggi PDFDokument1 SeiteBorang Denggi PDFAmiratuz Zalifah ZulkurnainNoch keine Bewertungen
- Influenza FormDokument2 SeitenInfluenza FormDipendra PoudelNoch keine Bewertungen
- Zika IcifDokument2 SeitenZika IcifMarav SymbNoch keine Bewertungen
- Laboratory Services: Patient Name Lab No Uhid Sample Date Age/Gender Receiving Date Referred by Report Date Report StatusDokument26 SeitenLaboratory Services: Patient Name Lab No Uhid Sample Date Age/Gender Receiving Date Referred by Report Date Report StatusTamzid Rabby TanmoyNoch keine Bewertungen
- Chikungunya FormDokument2 SeitenChikungunya FormTin Causaren-Gertos100% (1)
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument2 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Bharat BhushanNoch keine Bewertungen
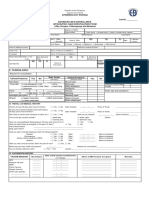
- Immediate/Case-based Surveillance Reporting Form IDSR 001ADokument58 SeitenImmediate/Case-based Surveillance Reporting Form IDSR 001ASalihu MustaphaNoch keine Bewertungen
- Laboratory Requisition Form 18062021Dokument2 SeitenLaboratory Requisition Form 18062021Sanja KostićNoch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument3 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)forged godNoch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument3 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Mohammed Shakeel khudusNoch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument2 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)ShakirShafiNoch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument2 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Lakshay JunejaNoch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument2 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Madhusmita MishraNoch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument2 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Madhusmita MishraNoch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument2 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)DevNoch keine Bewertungen
- Clinical Microbiology Laboratory Test RequisitionDokument1 SeiteClinical Microbiology Laboratory Test RequisitionRhodjane Dela Cruz0% (1)
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument3 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Lavanya LakshmiNoch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument2 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Harbrinder GurmNoch keine Bewertungen
- CIF PertussisDokument2 SeitenCIF PertussisDan Joseph AguilarNoch keine Bewertungen
- Crux 01Dokument8 SeitenCrux 01Rajkishor YadavNoch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument2 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)udayanNoch keine Bewertungen
- Final: 25 Years Female 28/07/2021 11:48 28/07/2021 11:48 29/07/2021 11:48Dokument2 SeitenFinal: 25 Years Female 28/07/2021 11:48 28/07/2021 11:48 29/07/2021 11:48meghna.maggidadhich123Noch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument2 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)narayanasmrithiNoch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument3 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)likhitNoch keine Bewertungen
- ESR Verification Form ReviseDokument4 SeitenESR Verification Form ReviseRouella DoverteNoch keine Bewertungen
- Ambrish Upadhyay ReportDokument4 SeitenAmbrish Upadhyay ReportpratikNoch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument3 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Shashi SagarNoch keine Bewertungen
- Case Investigation Form: DiphtheriaDokument3 SeitenCase Investigation Form: DiphtheriaSalihu MustaphaNoch keine Bewertungen
- CIF DiphDokument2 SeitenCIF DiphIvy marie BonNoch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument3 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)ARSLANNoch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument2 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)umera shah aliNoch keine Bewertungen
- Test - Report 24 - 01 - 2022Dokument3 SeitenTest - Report 24 - 01 - 2022Habib Ur RahmanNoch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument2 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Rahul KumarNoch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument2 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Sashibhusan NayakNoch keine Bewertungen
- Tropmed 83 690 PDFDokument6 SeitenTropmed 83 690 PDFabbhyasa5206Noch keine Bewertungen
- Discharge Planning TBDokument2 SeitenDischarge Planning TBNurida LatipahNoch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument3 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Pravat TiadiNoch keine Bewertungen
- ReportDokument2 SeitenReportRahul V SNoch keine Bewertungen
- In The Past1 4 Da S, Did You Have Any of Thefollowing:: SheetDokument1 SeiteIn The Past1 4 Da S, Did You Have Any of Thefollowing:: SheetLeoni FrancNoch keine Bewertungen
- Comp13 Unit6 (Belmont) Lecture SlidesDokument44 SeitenComp13 Unit6 (Belmont) Lecture SlidesBobNoch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument2 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)gopimicroNoch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument3 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Rohit KarhadeNoch keine Bewertungen
- Sample Report Blood Group SubDokument1 SeiteSample Report Blood Group SubAyrusNoch keine Bewertungen
- Sample Report Blood Group SubDokument1 SeiteSample Report Blood Group SubNarayan ChauhanNoch keine Bewertungen
- Needle Stick Injury FormatDokument1 SeiteNeedle Stick Injury Formatquality qualityNoch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument3 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)SgNoch keine Bewertungen
- Dharmila BhattDokument1 SeiteDharmila BhattytrdfghjjhgfdxcfghNoch keine Bewertungen
- Clinical Treatment PDFDokument1 SeiteClinical Treatment PDFDanielle YoderNoch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument3 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Anilkumar m rNoch keine Bewertungen
- Test Requisition FormDokument1 SeiteTest Requisition FormPreeti DesaiNoch keine Bewertungen
- VirologyDokument11 SeitenVirologyMarcoNoch keine Bewertungen
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Dokument3 SeitenIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)annapurna samalNoch keine Bewertungen
- Emt Physical FormDokument1 SeiteEmt Physical FormLeeann LopezNoch keine Bewertungen
- 19/jun/2021 06:14PM 32 Yrs/Male 19/jun/2021 12:08PM Dr. G.H. 01190178Dokument3 Seiten19/jun/2021 06:14PM 32 Yrs/Male 19/jun/2021 12:08PM Dr. G.H. 01190178Nitin GuptaNoch keine Bewertungen
- Typhoid Fever Surveillance ReportDokument2 SeitenTyphoid Fever Surveillance ReportMarketing HydNoch keine Bewertungen
- LL Gastroenteritis OutbreakDokument3 SeitenLL Gastroenteritis OutbreakHANS BENNoch keine Bewertungen
- Histopathology Reporting: Guidelines for Surgical CancerVon EverandHistopathology Reporting: Guidelines for Surgical CancerDavid P. BoyleNoch keine Bewertungen
- Natural Hosts of SIV: Implication in AIDSVon EverandNatural Hosts of SIV: Implication in AIDSAftab A. AnsariNoch keine Bewertungen
- Epidemiology and Biostatistics: Practice Problem WorkbookVon EverandEpidemiology and Biostatistics: Practice Problem WorkbookNoch keine Bewertungen
- Evaluation of Antibacterial Activity of Leaf and Root Extracts of Sansevieria Zeylanica On UTI Among Students in University of Benin, Edo StateDokument8 SeitenEvaluation of Antibacterial Activity of Leaf and Root Extracts of Sansevieria Zeylanica On UTI Among Students in University of Benin, Edo StateTunde EgunjobiNoch keine Bewertungen
- Igenex PricesDokument2 SeitenIgenex Pricesapi-316589352Noch keine Bewertungen
- Quanti-Cult Plus ENG Dos PasesDokument4 SeitenQuanti-Cult Plus ENG Dos Pasessagor sagorNoch keine Bewertungen
- Iej 04 2009Dokument104 SeitenIej 04 2009Israel CurveloNoch keine Bewertungen
- Gopu.R:::: Patient Age / Sex 30 Y / Male BranchDokument1 SeiteGopu.R:::: Patient Age / Sex 30 Y / Male BranchGopu RNoch keine Bewertungen
- National Polio Eradication ProgramDokument36 SeitenNational Polio Eradication Programayushi rainaNoch keine Bewertungen
- A Century of The Phage - Past, Present and FutureDokument10 SeitenA Century of The Phage - Past, Present and Futureambreensaba.btconNoch keine Bewertungen
- THT RhinosinusitisDokument8 SeitenTHT RhinosinusitismeiliaNoch keine Bewertungen
- The Main Themes of MicrobiologyDokument31 SeitenThe Main Themes of MicrobiologyJhon VincentNoch keine Bewertungen
- DysenteryDokument9 SeitenDysenteryFareed KhanNoch keine Bewertungen
- Cory Ne BacteriumDokument28 SeitenCory Ne BacteriumDayana PrasanthNoch keine Bewertungen
- Guide To Utilization of The Microbiology Laboratory For Diagnosis of Infectious Diseases 2024 Update by IDSA-ASMDokument244 SeitenGuide To Utilization of The Microbiology Laboratory For Diagnosis of Infectious Diseases 2024 Update by IDSA-ASMmicrobehunter0070% (1)
- MicroLab - Identification of Bacteria - Dr. Sia-CuncoDokument17 SeitenMicroLab - Identification of Bacteria - Dr. Sia-CuncoRyn ShadowNoch keine Bewertungen
- HerpesDokument3 SeitenHerpesNizam UddinNoch keine Bewertungen
- Makalah Virus Corona 19Dokument11 SeitenMakalah Virus Corona 19SadiliRedhaNoch keine Bewertungen
- Feline Worming FactsheetDokument2 SeitenFeline Worming FactsheetPilar Mitra QurbanNoch keine Bewertungen
- A Brief Guide To Poultry Diseases ManagementDokument29 SeitenA Brief Guide To Poultry Diseases ManagementGrowel Agrovet Private Limited.83% (6)
- Nervous Tissue Anti-Rabies Vaccine For Human UseDokument2 SeitenNervous Tissue Anti-Rabies Vaccine For Human UseLet BNoch keine Bewertungen
- Mancuso 2018Dokument19 SeitenMancuso 2018Jessica Martinez CortezNoch keine Bewertungen
- Microbiology: OrthomyxovirusDokument3 SeitenMicrobiology: OrthomyxovirusJustin TayabanNoch keine Bewertungen
- Growth and Physiology of BactDokument3 SeitenGrowth and Physiology of Bactyam pdNoch keine Bewertungen
- Tuberculin Skin Test. Prevention of Tuberculosis.: 2. The Department of Tuberculosis of KSMA. Doc. Fydorova S.VDokument46 SeitenTuberculin Skin Test. Prevention of Tuberculosis.: 2. The Department of Tuberculosis of KSMA. Doc. Fydorova S.VMadabout MusicNoch keine Bewertungen
- Pneumococci MIcro LabDokument52 SeitenPneumococci MIcro LabSandy AtefNoch keine Bewertungen
- Micro-Organisms QA WorksheetDokument7 SeitenMicro-Organisms QA WorksheetHina HussainNoch keine Bewertungen
- BioLumix NutraCBioLumix RMM Platform Featured in Latest Edition of NutraCos Journalos-Revise FINALDokument3 SeitenBioLumix NutraCBioLumix RMM Platform Featured in Latest Edition of NutraCos Journalos-Revise FINALAnnabel ElizabethNoch keine Bewertungen
- WJL Topic 2 - GeneTransfer - SDokument99 SeitenWJL Topic 2 - GeneTransfer - Sjuinshin.wee23Noch keine Bewertungen
- Jurnal SkripsiDokument10 SeitenJurnal Skripsinorma. nlmhNoch keine Bewertungen
- Lyme Disease in Dogs: Borrelia SPPDokument2 SeitenLyme Disease in Dogs: Borrelia SPPHector UsamanNoch keine Bewertungen
- Virus TableDokument3 SeitenVirus TableFrozenManNoch keine Bewertungen
- Food Safety Case - The Fat Duck Norovirus Outbreak, UK - 2009Dokument16 SeitenFood Safety Case - The Fat Duck Norovirus Outbreak, UK - 2009OPGJrNoch keine Bewertungen